
Abstract
It has been argued that the growth rate of exclusively breast-fed infants may be limited by their protein intake. This issue was examined using data from an intervention study in Honduras in which infants were randomly assigned to be exclusively breast-fed for the first 6 mo (EBF; n = 50), or to receive preprepared solid foods (including egg yolk) in addition to breast milk beginning at 4 mo (n = 91). Neither weight gain nor length gain from 4 to 6 mo differed between groups despite a 20% higher protein intake (as well as significantly higher intakes of iron, zinc, calcium, vitamin A, and riboflavine) in the latter group. The 20 infants with the highest protein intakes in that group were matched to 20 EBF infants on the basis of energy intake; protein intake was 1.46 ± 0.09 versus 1.10 ± 0.17 g/kg/d, respectively (p < 0.001), but growth rate did not differ between groups. Similarly, the 20 infants with the lowest protein intakes in the EBF group were matched (by energy intake) to 20 infants given solid foods; protein intake was very low in the former compared with the latter (0.81 ± 0.13 versus 1.04 ± 0.20 g/kg/d;p < 0.001), yet there was still no difference in growth. Infant morbidity was relatively low and did not influence the results. These analyses indicate that protein intake is not likely to be a limiting factor with regard to growth of breast-fed infants from 4 to 6 mo of age.
Similar content being viewed by others

Main
In most estimates of nutrient requirements, the EBF infant is used as the model for the first 6 mo of life. However, in the case of protein, doubts have been raised about whether the amount consumed by breast-fed infants is truly optimal(1). It has been argued that the composition of human milk represents an evolutionary compromise between the needs of the infant and the needs of the mother, and that lower milk protein concentrations may protect the lactating mother from becoming nutritionally depleted. The observation that breast-fed infants gain weight less rapidly than do formula-fed infants after the first 2-3 mo(2–4) leads some to question whether breast-fed infants are really meeting their protein requirements.
In formula-fed infants, slower growth rates have been observed when they are fed formulas with a protein content closer to that of human milk than when they are fed standard, higher protein formulas(5), but this may be due to lower utilization of protein from formulas than from human milk. In observational studies of breast-fed infants, absolute protein intake(grams/d) is also positively associated with weight gain(6). However, it is difficult to separate the effect of protein from that of energy intake, as these two are highly correlated. When controlling for energy intake, protein intake (i.e. protein per 100 kcal) has not been found to be associated with growth rate of breast-fed infants during the first year of life(6).
Definitive answers to the question of whether breast-fed infants need more protein can be obtained only through intervention studies. The purpose of this study is to report data on protein intake and growth from an intervention trial in which infants exclusively breast-fed for 4 mo were randomized to continue exclusive breast-feeding until 6 mo or to receive complementary foods from 4 to 6 mo of age. Because the complementary foods given were relatively high in protein, the design of this study provides an opportunity to evaluate protein needs of breast-fed infants. The main results of the intervention trial have been reported elsewhere(7). This report focuses on relationships between protein intake and growth.
METHODS
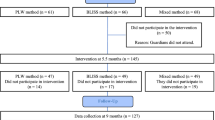
Study design. Data for these analyses come from results of a randomized intervention trial conducted in an urban population in San Pedro Sula, Honduras. The study was approved by the Human Subjects Review Committee at the University of California, Davis. Details of the intervention trial are described elsewhere(7). Briefly, low income, primiparous women who had given birth to healthy, term infants were recruited from two public hospitals. Lactation guidance was provided during regular home visits to promote exclusive breast-feeding during the first 4 mo postpartum. At 16 wk, subjects who were exclusively breast-feeding were randomly assigned by week of birth to one of three groups: 1) control (n = 50): EBF to 26 wk; no other liquids (water, milk, formula) or solids; 2) SF (n = 47): introduction of SF at 16 wk, with ad libitum breast-feeding, or 3) SF-M (n = 44): introduction of SF at 16 wk, with maintenance of preintervention breast-feeding frequency.
At 16 wk subjects stayed at a central unit for 3 d to collect baseline data on breast milk intake and composition. After completing the baseline measurements, infants assigned to the SF and SF-M groups were given their first SF and their mothers were instructed to feed them twice per day thereafter. Commercial baby foods in jars were provided to avoid the potentially confounding influence of increased morbidity or nutritional inadequacy if home-prepared foods had been used. The combination of foods provided (rice cereal with egg yolk, fruits, and vegetables) was selected to meet or exceed the nutrient density (per 100 kcal) required to satisfy the recommended dietary allowances(8) for infants for 14 nutrients (protein, vitamin A, vitamin C, thiamine, riboflavine, niacin, vitamin B6, folate, vitamin B12, calcium, phosphorus, magnesium, iron, and zinc), if these foods had been the only source of energy. The rice cereal + egg yolk product (prepared by Gerber Products Company) was already fortified with iron at the levels normally used in the wet rice cereal; zinc and calcium were also added to meet the above nutrient density criterion. In this product, about 80% of the protein came from egg yolk and 20% from rice.
Between 16 and 26 wk mothers were visited weekly to assess infant growth and morbidity, and to deliver baby foods and feeding instructions to the SF groups. All subjects returned to the central unit at 21 and 26 wk to repeat the intake measurements.
Anthropometry. Birth weight was recorded from the birth certificate or from parental recall. Infant weight was measured (to the nearest 100 g using a Salter scale) at wk 1, 2, 6, 10, and 14, and weekly between 16 and 26 wk. Infant length was measured to the nearest 0.1 cm on a recumbent board at wk 16, 21, and 26. Weights and lengths were adjusted (by linear interpolation) when they were measured more than 1 wk from the target date. Maternal height (to the nearest 0.1 cm) was measured initially, and weight (to the nearest 0.2 kg) was measured on a regular basis.
Infant intake. During the visits to the central unit, breast milk intake was measured by weighing before and after each feeding for 48 h using an electronic balance (Sartorius, Göttingen, FRG) accurate to 1 g. Twenty-four-hour breast milk intake was calculated correcting for insensible water loss during feedings, as described elsewhere(7).
After the 48-h test-weighing period, breast milk samples were collected for 24 h using the alternate breast expression method(9). Samples of milk proportional to the volume pumped at each feeding were pooled and frozen for later analysis. Lipid concentration was determined by a modified Folch extraction(10). Total nitrogen and non-protein nitrogen concentration were determined by the micro-Kjeldahl procedure(11) using a block digestor; protein concentration was calculated as the difference. Lactose was analyzed in a sub-sample (46 subjects, 134 samples) using a colorimetric assay(12). This subsample was used to develop prediction equations for milk energy density based on lipid concentration alone, using values of 0.039 MJ/g (9.25 kcal/g) of lipid, 0.024 MJ/g (5.65 kcal/g) of protein, and 0.017 MJ/g (3.95 kcal/g) of lactose(13). Energy intake from breast milk was calculated as milk intake multiplied by energy density. To estimate micronutrient content of breast milk, values from the literature were used for vitamin A and riboflavine in mature milk(14) and for iron, zinc, and calcium at 5-6 mo postpartum(15).
At 5 and 6 mo, intake of SF in the SF and SF-M groups was weighed to the nearest gram during the same 48-h period in which breast milk intake was measured. Values were adjusted to account for the fact that there was a lower intake of SF in the home than in the central unit, as described elsewhere(7). Nutrient intake from SF was calculated using the manufacturer's values.
Morbidity. Information on infant illness was collected at each home visit by maternal recall of specific symptoms (e.g. nasal discharge, cough, and fever). Mothers kept a daily record of stool frequency and consistency. Diarrhea was defined as more than three liquid stools in 24 h. Upper respiratory illness was defined by the presence of both nasal discharge and cough.
Data analysis. For these analyses, the SF and SF-M groups were combined into an SF-combined group because nutrient intakes in these two subgroups were very similar; this maximizes our power to detect significant differences between the EBF and SF-combined groups. Comparisons of intake and growth from 4 to 6 mo between these two groups were made using analysis of variance. When weight or length gain from 4 to 6 mo was the outcome variable, analyses were also performed using initial weight or length at 4 mo as a covariate, and controlling for any other potentially confounding variables.
The relationships between protein intake and growth, with all groups combined, were examined using both Pearson correlations and multiple regression analysis controlling for initial weight or length at 4 mo and infant morbidity (percentage of days with diarrhea, respiratory illness, or fever) during the 2-mo study period from 4 to 6 mo of age. Protein intake was expressed in several ways: as absolute intake (grams/d), intake per kg(grams/kg/d), and as the residual of protein intake when regressed on energy intake. The latter variable adjusts for the fact that energy and protein intakes are highly correlated, and is the best choice for examining the independent effects of protein intake on growth.
To examine whether there were any differences in growth associated with the extremes of the distribution of protein intake, two sets of matched subgroups were created. For the first (the high protein “match”), we selected the 20 infants in the two SF groups (SF-combined), with the highest protein intakes per kg at 5-6 mo, and matched them to 20 infants in the EBF group on the basis of energy intake per kg (averaged over the three measurements at 4, 5, and 6 mo). For the second (the low protein“match”), we selected the 20 infants in the EBF group with the lowest protein intakes per kg at 5-6 mo, and matched them to 20 infants in the combined SF and SF-M groups on the basis of energy intake per kg from 4 to 6 mo. Comparisons between the selected subgroups for each match were made using analysis of variance, with and without controlling for any differences in characteristics of the two matched groups.
RESULTS
As shown in Table 1, the EBF and SF-combined groups were similar in most characteristics, except that the latter group was less likely to have received prenatal care. Average energy intake from 4 to 6 mo(megajoules/d) did not differ significantly between groups, but because infants in the EBF group were somewhat heavier, intake per kg body weight was significantly lower in that group. After the introduction of SF, average protein intake (grams/kg/d) of the SF-combined group was about 20% higher than that of the EBF group. About 25% of protein intake in the SF-combined group came from SF. Intakes of iron, zinc, calcium, vitamin A, and riboflavine were also significantly higher in the SF-combined group, primarily due to fortification of the cereal-egg yolk product with iron, zinc, and calcium.
Despite these differences in intake, there was no significant difference between groups in weight or length gain from 4 to 6 mo, either in the unadjusted means, or when the means were adjusted for initial weight or length at 4 mo and maternal prenatal care.
With all groups combined (n = 141), protein and energy intake per kg were highly correlated (r = 0.82, p < 0.0001, for the average of values at 5 and 6 mo). Absolute protein intake at 5 and 6 mo(grams/d) was positively correlated with weight gain (r = 0.28,p < 0.001), but not with length gain (r = 0.02) from 4 to 6 mo. Protein intake per kg was not significantly correlated with weight(r = -0.08) or length (r = -0.08) gain from 4 to 6 mo, nor was the residual variable for protein intake (adjusted for energy intake;r = -0.07 and r = 0.06 for weight and length gain, respectively). Within the EBF group, there was no relationship between infant growth and either breast milk protein concentration or the percentage of energy from protein in milk. None of the above relationships was changed when initial weight or length at 4 mo and the infant morbidity variables were included in multiple regression analysis.
In the subgroups selected for the high protein “match,” average protein intake was 33% higher in the SF-combined subgroup than in the EBF subgroup (1.46 versus 1.10 g/kg/d, p < 0.0001). There were no significant differences in weight or length gain from 4 to 6 mo between these subgroups (989 ± 327 versus 1164 ± 394 g weight gain and 3.7 ± 1.2 versus 3.9 ± 1.4 cm length gain in the SF-combined versus EBF subgroups, respectively), with or without controlling for characteristics that differed between subgroups. In the low protein “match,” average protein intake of the infants in the EBF subgroup was 0.81 g/kg/d, compared with 1.04 g/kg/d in the matched SF-combined subgroup (p < 0.0001). Despite the very low protein intakes of this EBF subgroup, their weight and length gains from 4 to 6 mo did not differ significantly from those of the SF-combined subgroup (1059 ± 284 versus 1088 ± 348 g weight gain and 4.0 ± 1.0versus 4.1 ± 1.4 cm length gain in the SF-combinedversus EBF subgroups, respectively), with or without controlling for characteristics that differed between subgroups.
DISCUSSION
These results indicate that the extra protein provided by complementary feeding of breast-fed infants does not alter their rate of growth in either weight or length from 4 to 6 mo. Although this study was carried out in a low income population in a developing country, the rates of diarrhea and other illnesses in these infants in the first 6 mo of life were very low and did not differ between groups, presumably because the infants were fully breast-fed and the foods given were hygienically prepared and packaged. Thus, morbidity is not likely to have been a limiting factor in the potential for a growth response from 4 to 6 mo. Similarly, the protein quality of the foods provided is unlikely to have been a limiting factor because egg yolk provided most of the protein. The micronutrient quality of the foods provided was also very high, and because of this estimated intakes of iron, zinc, calcium, vitamin A, and riboflavin were all significantly higher among infants given SF, yet there was no impact on growth. It is unlikely that energy intake limited a growth response to protein, as there was evidence that the infants were meeting their energy needs: on average they left unconsumed about 100 g/d of“residual” breast milk(16), and in the groups receiving SF, none of the infants consumed all of the food made available to them each day.
The results of this study are consistent with those from an observational study of breast-fed infants in an affluent population (the DARLING study)(6), in which protein density of the diet was unrelated to growth throughout the first year of life. Intakes of energy and protein by the Honduran infants at 4-6 mo (shown in Table 1) were similar to those of the DARLING breast-fed infants at 6 mo, which averaged 0.34 MJ/kg/d (80.1 kcal/kg/d) and 1.06 g/kg/d, respectively. Growth of the Honduran and DARLING breast-fed infants was also very similar from 4 to 6 mo, although weight gain in the first 4 mo of life was significantly greater in the Honduran infants (presumably due to their lower average birth weight)(17). On the basis of the evidence from both of these studies, it could be concluded that extra protein has no beneficial impact on growth of exclusively breast-fed infants. However, it is possible that the outcome would be different if the foods containing the extra protein did not displace breast milk intake. In this study, infants given SF consumed less breast milk after SF were introduced(7), and thus they may have been at a disadvantage in certain other respects. The displacement of breast milk that occurs when SF are introduced appears to be due to infant self-regulation of energy intake(6, 18), and thus is likely to be unavoidable. Therefore, the ideal test of the hypothesis that human milk protein is limiting would be to conduct an experiment in which concentrated protein with minimal energy content was provided, to minimize displacement of breast milk. However, even if such an experiment were to result in accelerated growth, from a public health perspective this approach would be unrealistic, as the only practical way of supplementing breast-fed infants with extra protein is through foods.
Another possibility to consider is that the growth response to increased protein could not occur because intake of some other nutrient was limiting, despite the fortification of the infant cereal provided. The bioavailability of nutrients such as iron and zinc may be compromised when SF are added to the diet of a breast-fed infant(19, 20). Without further information on the absorption of these micronutrients under these circumstances, it is difficult to evaluate this possibility. However, given that the group given SF received twice as much zinc and 25 times as much iron(in the form of ferrous sulfate) as the exclusively breast-fed group, it seems unlikely that the availability of either of these nutrients was inadequate for growth. Zinc bioavailability could have been impaired by phytate in the rice cereal, but the estimated phytate to zinc molar ratio of the diet (<10) was lower than the level considered to interfere with zinc absorption(21). Similarly, the relatively high iron to zinc molar ratio (4.5) theoretically might have affected zinc absorption, but clinical trials generally have not shown any evidence of this effect in adults(22) or infants(23) when the iron is consumed in meals.
To conclude, we have demonstrated that protein intake of exclusively breast-fed infants is not likely to be a limiting factor with respect to growth from 4 to 6 mo of age. Thus, there is no evidence that the difference in growth velocity between breast-fed and formula-fed infants at that age(2–4) is a function of marginal protein intake in the former group.
Abbreviations
- EBF:
-
exclusively breast-fed
- SF:
-
solid food
- SF-M:
-
solid food with maintenance of breast-feeding frequency
References
Fomon SJ 1993 Nutrition of Normal Infants. Mosby-Year Book, St. Louis, pp 121–139
Dewey KG, Heinig MJ, Nommsen LA, Peerson JM, Lonnerdal B 1992 Growth of breast-fed and formula-fed infants from 0 to 18 months: the DARLING study. Pediatrics 89: 1035–1041
Duncan B, Schaefer C, Sibley B, Fonseca NM 1984 Reduced growth velocity in exclusively breast-fed infants. Am J Dis Child 138: 309–313
Salmenpera L, Perheentupa J, Siimes M 1985 Exclusively breast-fed healthy infants grow slower than reference infants. Pediatr Res 19: 307–312
Axelsson IE, Jakobsson I, Raiha NCR 1988 Formula with reduced protein content: effects on growth and protein metabolism during weaning. Pediatr Res 24: 297–301
Heinig MJ, Nommsen LA, Peerson JM, Lonnerdal B, Dewey KG 1993 Energy and protein intakes of breast-fed and formula-fed infants during the first year of life and their association with growth velocity: the DARLING study. Am J Clin Nutr 58: 152–161
Cohen RJ, Brown KH, Canahuati J, Landa Rivera L, Dewey KG 1994 Effects of age of introduction of complementary foods on infant breast milk intake, total energy intake and growth: a randomized intervention study in Honduras. Lancet 344: 288–293
Food and Nutrition Board. 1989 Recommended Dietary Allowances. National Academy Press, Washington, DC
Nommsen LA, Lovelady CA, Heinig MJ, Lonnerdal B, Dewey KG 1991 Determinants of energy, protein, lipid, and lactose concentrations in human milk during the first 12 mo of lactation: the DARLING study. Am J Clin Nutr 53: 457–465
Folch J, Lees M, Sloan SGH 1957 A simple method for the isolation and purification of total lipids from animal tissue. J Biol Chem 226: 497–509
Hambraeus L, Forsum E, Abrahamsson L, Lonnerdal B 1976 Automatic total nitrogen analysis in nutritional evaluations using a block digestor. Anal Biochem 72: 78–85
Dahlqvist A 1964 Method for assay of intestinal disaccharidases. Anal Biochem 7: 18–25
Garza C, Butte NF, Dewey KG 1985 Determination of the energy content of human milk. In: Jensen RG, Neville MC (eds) Human Lactation. I. Milk Components and Methodologies. Plenum Press, New York, pp 121–125
Institute of Medicine 1991 Nutrition during Lactation. National Academy Press, Washington, DC, p 116
Dewey KG, Lonnerdal B 1983 Milk and nutrient intake of breast-fed infants from 1 to 6 months: relation to growth and fatness. J Pediatr Gastroenterol Nutr 2: 497–506
Perez-Escamilla R, Cohen RJ, Brown KH, Landa Rivera L, Canahuati J, Dewey KG . 1995 Maternal anthropometric status and lactation performance in a low-income Honduran population: evidence for the role of infants. Am J Clin Nutr 61: 528–534
Cohen RC, Brown KH, Canahuati J, Landa Rivera L, Dewey KG . 1995 Determinants of growth from birth to 12 months among breast-fed Honduran infants in relation to age of introduction of complementary foods. Pediatrics 96: 504–510
Stuff JE, Nichols BL 1989 Nutrient intake and growth performance of older infants fed human milk. J Pediatr 115: 959–968
Bell JG, Keen CL, Lonnerdal B 1987 Effect of infant cereals on zinc and copper absorption during weaning. Am J Dis Child 141: 1128–1132
Oski FA, Landaw SA 1980 Inhibition of iron absorption from human milk by baby food. Am J Dis Child 134: 459–460
Ellis R, Kelsay JL, Reynolds RD, Morris ER, Moser PB, Frazier CW 1987 Phytate: zinc and phytate calcium:zinc millimolar ratios in self-selected diets of Americans, Asian Indians, and Nepalese. J Am Diet Assoc 87: 1043–1047
Sandstrom B, Davidsson L, Cederblad A, Lonnerdal B 1985 Oral iron, dietary ligands and zinc absorption. J Nutr 115: 411–414
Haschke F, Ziegler EE, Edwards BB, Fomon SJ 1986 Effect of iron fortification of infant formula on trace mineral absorption. J Pediatr Gastroenterol Nutr 5: 768–773
Acknowledgements
We are grateful to the Honduran research team for their dedicated work on the project, to the La Leche League/Honduras staff and the Ministry of Health/Honduras for their cooperation, and to the mothers of San Pedro Sula for their willingness to participate in the study. Rafael Perez-Escamilla and Laurie Rivers provided invaluable assistance in analyzing the milk samples.
Author information
Authors and Affiliations
Additional information
Supported jointly by the Thrasher Research Fund; the World Health Organization; UNICEF/Honduras; and the Institute for Reproductive Health(formerly the Institute for International Studies in Natural Family Planning), Georgetown University, under a Cooperative Agreement with the United States Agency for International Development (A.I.D.) (DPE-3040-A-00-5064-00 and DPE-3061-A-00-1029-00). The views expressed by the authors do not necessarily reflect the views of these institutions. Complementary foods were provided at reduced cost by Gerber Products Company.
Rights and permissions
About this article
Cite this article
Dewey, K., Cohen, R., Rivera, L. et al. Do Exclusively Breast-Fed Infants Require Extra Protein?. Pediatr Res 39, 303–307 (1996). https://doi.org/10.1203/00006450-199602000-00019
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199602000-00019
