
Abstract
The objective of this study was to determine the role of oxidant stress in cell injury produced by in vivo copper overload of isolated rat hepatocytes. Rats were maintained on diets with elevated or normal copper content, and hepatocytes were isolated and then incubated for 4 h in physiologic buffer at physiologic oxygen saturations. In hepatocytes from copper-overloaded rats, a significant loss of cell viability (trypan blue exclusion) over 4 h compared with control cells was associated with a significant increase in lipid peroxidation (thiobarbituric acid-reacting substances). Incubation of copper-overloaded hepatocytes with the copper chelator, 2,3,2-tetramine, had a partial protective effect. Incubation with D-α-tocopheryl succinate completely ameliorated the copper-induced changes in viability and lipid peroxidation. We conclude that antioxidants may protect the isolated hepatocyte from copper toxicity and should be explored as potential therapeutic agents in states of copper overload.
Similar content being viewed by others
Main
Human and animal copper-overload states are associated with severe hepatic injury, culminating in fulminant hepatic failure or cirrhosis(1, 2). In patients with Wilson's disease, a genetic defect in intracellular copper transport(3, 4) causes failure of hepatocyte excretion of copper into bile and impairment of secretion of ceruloplasmin, the major hepatic-derived circulating copper transport protein(1). The resultant accumulation of hepatocellular copper invariably leads to hepatic injury, fibrosis, cirrhosis, and death if not treated(1). In addition, other organs and tissues accumulate copper after the hepatic storage capacity has been exceeded, leading to basal ganglion, renal, corneal, and other lesions(1, 2). Hepatic copper toxicity also plays a role in Indian childhood cirrhosis(5) and in idiopathic North American childhood cirrhosis(6), although the etiology of copper overload in these disorders has not been fully elucidated. Recent evidence suggests an increased ingestion of copper-contaminated milk or water may be involved in the latter two disorders(7).
Treatment of human copper overload disorders is based on the chelating and cupriuretic effect of several agents(1, 2) and the impairment of copper absorption induced by oral zinc therapy(8). Despite general improvement in the hepatic injury if chelation therapy is started relatively early in the course of liver damage(2, 9), many patients fail to have a significant response to chelation therapy and eventually require liver transplantation to avoid death(10, 11). A similar lack of response to chelation therapy has been demonstrated in advanced Indian childhood cirrhosis(12). Moreover, in fulminant hepatic failure caused by Wilson's disease, copper chelation and zinc therapy is completely ineffective(1, 2, 13). Therefore, there is a continued need for the development of improved treatment for copper-overload conditions.
To develop treatment strategies for copper-overload diseases requires a thorough understanding of the underlying cellular and molecular mechanisms by which copper damages the liver. Previous studies in copper-overloaded rats(14, 15), dogs(16), and humans with Wilson's disease(16) have documented evidence of oxidant injury to hepatic mitochondria, suggesting that free radicals may be involved in copper hepatic toxicity. These studies led to the proposal that antioxidant therapy might be of value in states of copper overload. To test this hypothesis, we have attempted to develop an in vitro hepatocyte system in which copper toxicity and antioxidant status could be manipulated. Initial attempts were directed at incubating hepatocytes isolated from normal rats with toxic doses of cupric chloride and with antioxidants(17); however, the applicability of thisin vitro model to in vivo copper overload states is not clear. The purpose of the present study was to develop a model by whichin vivo copper overload of the rodent liver could be studied in an isolated hepatocyte preparation, to determine the role of oxidant stress in these in vivo copper-overloaded hepatocytes, and to compare the relative effects of copper chelation and antioxidant (vitamin E) treatment in this model.
METHODS
Animals. Weanling male Sprague-Dawley rats were obtained from Sasco Inc. (Omaha, NE) and housed in polyethylene cages with stainless steel wire tops on 12-h day-night light cycles. All rats received humane care under the guidelines of Animal Care Committee of the University of Colorado Health Sciences Center. To achieve two different states of copper nutritional status, rats were randomly assigned to receive an 8-wk course of one of two semisynthetic diets obtained from Dyets, Inc. (Bethlehem, PA): a high copper group received 1000 mg of copper (as cupric chloride) per kg of diet for the first 4 wk followed by 2000 mg/kg of diet for 4 wk, as previously described(14). This diet produces hepatic copper levels after 8 wk that are similar to those in humans with Wilson's disease, approximately 20-fold elevated compared with a control diet, and a portal triaditis with focal hepatocyte necrosis(14). A control diet had 6 mg of copper/kg of diet. Both diets contained 50 IU of α-tocopherol acetate/kg of diet (the recommended normal dietary content) and stripped corn oil as the dietary lipid source. Both diets were otherwise nutritionally complete and identical. Control rats were pair-fed to produce the same weight gain observed in the copper-overloaded rats.
Hepatocyte Isolation. After 8 wk of diet, rats were killed, and hepatocytes were isolated from each rat by a modification of the recirculatingin situ collagenase technique, as previously described(17). An important modification of this technique was the use of 9% O2/86% N2/5% CO2 as the gas bubbled through the isolation buffer and maintained in the atmosphere in flasks containing the isolated hepatocytes, to achieve the oxygen content normally present in the liver and thus avoid a hyperoxic stress. This modified technique results in over 92% viable hepatocytes based on trypan blue exclusion. After isolation, hepatocytes were maintained at 4°C until used for experiments within 2 h of isolation. Blood was obtained from the inferior vena cava before starting the liver perfusion and analyzed for serum aspartate aminotransferase, alanine amino-transferase, alkaline phosphatase, and bilirubin by an automated analyzer. An aliquot of freshly isolated hepatocytes was stored frozen at-20°C and analyzed for copper content by atomic absorbance spectroscopy(20) on a Perkin-Elmer 360 atomic absorption spectrophotometer and 2100-HGA controller and furnace (Perkin-Elmer Corp., Norwalk, CT). Hepatocyte copper content was expressed as micrograms/106 cells.
Experimental Design. Freshly isolated hepatocytes from both copper-overloaded and control rats were resuspended in Krebs-Henseleit buffer containing 2% BSA, 1% D-glucose, and a mixture of amino acids(18) at a concentration of 1.0 × 106 cells/mL. Aliquots of cells were incubated at 37°C in a shaking water bath with one of the following: D-α-tocopheryl succinate solubilized in ethanol (final concentration of 200 μM for α-tocopherol and 0.05% for ethanol); ethanol as a control (final concentration of 0.05%); or 2,3,2-tetramine, a potent copper chelator(19) (final concentration of 100 μM). All cells were incubated in sealed flasks under an atmosphere of 9% O2/86% N2/5% CO2 that was sparged every 15 min. Aliquots of hepatocytes, removed at baseline and each hour for 4 h, were analyzed for viability [trypan blue exclusion(17)] and lipid peroxidation by the TBARS method, as previously described(17). A standard curve for the TBARS assay was constructed daily using 1,1,3,3-tetraethoxypropane as the standard; results were expressed as nanomoles of TBARS/106 hepatocytes.
Statistical Analysis. Differences among experimental groups were tested for significance by the unpaired t test or the analysis of variance with the Scheffe F test. Correlations were examined by linear regression analysis (least squares technique). A p value of<0.05 was considered statistically significant. Data were expressed as mean± SEM.
RESULTS
Pair-fed rats maintained on the two dietary regimens were of equal weight at the time of sacrifice (Table 1). Serum aspartate aminotransferase and alanine aminotransferase concentrations were significantly increased in the copper-overloaded rats (Table 1), indicating chronic hepatocellular injury caused by excess dietary copper intake. Alkaline phosphatase and bilirubin did not vary between groups. Hepatocyte copper content (Table 1) reflected the dietary copper intake, with approximately a 15-fold copper increase in the copper-overloaded hepatocytes.
Initial viability of hepatocytes isolated from copper-overloaded rats (95.9± 0.9%) did not differ from that of control rats (97.5 ± 0.4%). Likewise, initial TBARS values of hepatocytes isolated from copper-overloaded rats were undetectable in cells from all rats. Therefore, copper-loaded hepatocytes tolerated the isolation procedure without evidence of significant damage or oxidant injury occurring during the isolation.
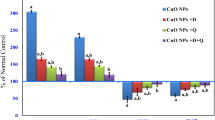
Incubation of freshly isolated control hepatocytes over 4 h resulted in a small decrease of viability to 83 ± 2% at 4 h (Fig. 1A). Incubation of copper-loaded hepatocytes resulted in a progressive decrease in viability over 4 h to 60 ± 5% that was significantly greater than that observed in control hepatocytes (Fig. 1A). Incubation of copper-overloaded hepatocytes with 2,3,2-tetramine resulted in a significant but partial improvement in cell viability(Fig. 1A). However, incubation of copper-overloaded hepatocytes with α-tocopheryl succinate improved cell viability to equal that of the control hepatocytes (Fig. 2A).α-Tocopheryl succinate and 2,3,2-tetramine incubation had no significant effects on viability of control hepatocytes (data not shown).

Trypan blue exclusion (A) and TBARS(B) of hepatocytes isolated from copper-overloaded (Cu) or control (Con) rats incubated in physiologic buffer and at physiologic oxygen tensions for 4 h. Hepatocytes isolated from copper-overloaded rats were also treated in vitro with 100 μM 2,3,2-tetramine (Cu + Tetra). *p < 0.05 vs control cells.

Effect of incubation of copper-overloaded hepatocytes with 200 μM α-tocopheryl succinate (Cu + Toc) on trypan blue exclusion (A) and TBARS levels (B). *p < 0.05 vs control (Con) and Cu + Toc.
TBARS values increased progressively over 4 h in the copper-loaded hepatocytes and were significantly higher (p < 0.05) than those from control hepatocytes at time points beyond 1 h of incubation(Fig. 1B). Similar to the effects observed on cell viability, 2,3,2-tetramine incubation partially and α-tocopheryl succinate incubation completely ameliorated the rise of TBARS in copper-overloaded cells (Figs. 1B and2B). There was no significant effect of either α-tocopheryl succinate or 2,3,2-tetramine on TBARS values in control hepatocytes (data not shown).
Combining data from hepatocytes of all incubations, there was a strong correlation (p < 0.001) between the loss of cell viability(trypan blue exclusion) and the degree of oxidant damage to the hepatocytes(TBARS) after 1, 2, 3, and 4 h of incubation (r = 0.91, 0.88, 0.86, and 0.74, respectively).
DISCUSSION
The cellular mechanisms involved in the pathogenesis of copper-induced liver injury are poorly characterized. Postulated mechanisms include inhibition of sulfhydryl-containing enzymes, polymerization of proteins, alteration of charge of the plasma membrane, inhibition of tubulin polymerization, and perturbations in lysosomal function(1). The role of oxidant damage to the liver during states of excess hepatic copper has received recent attention. Copper is a potent catalyst of the Fenton reaction by which O˙2 reacts with H2O2 yielding the extremely reactive hydroxyl free radical(OH·) (reactions 1–3). The resulting hydroxyl radical readily reacts with polyunsaturated fatty acids to initiate lipid peroxidation, thiol-containing proteins, and nucleic acids, resulting in cellular injury(21). Excess copper may also cause oxidant damage by the direct oxidation of susceptible proteins and lipids. Theoretically, during copper overload, if the copper chelation capacity of intracellular metallothionein in hepatocytes is exceeded, copper could become available for these reactions.
In this study we have validated the utility of using hepatocytes isolated from dietary copper-loaded rats to study the role of oxidant stress in copper hepatic toxicity. The results show that these in vivo copper-overloaded hepatocytes undergo a time-dependent loss in cell viability compared with control hepatocytes when incubated in a physiologic buffer and at physiologic oxygen concentrations. This decrease in viability was closely paralleled by increased lipid peroxidation compared with control values. Moreover, the lipid-soluble, membrane-localized antioxidant,α-tocopherol, which is taken up well by isolated hepatocytes in suspension when delivered as the succinate ester(17), completely ameliorated both hepatocyte injury and lipid peroxidation. Although hepatocyte α-to-copherol concentrations were not measured in this study, we have previously shown a 6-fold increase in hepatocyte α-tocopherol content after a 30-min incubation with 200 μM α-to-copherol under similar experimental conditions(22). Because these incubations were carried out at the relatively low physiologic oxygen concentrations found in liver (9% O2), oxygen toxicity to the hepatocytes does not explain these findings. The potent copper chelating agent, 2,3,2-tetramine(19), had only a partial protective effect in our model, most likely because insufficient time was available in our system for this chelator to be taken up well by hepatocytes and chelate the excess copper that was present in multiple intracellular compartments. It is also possible that a portion of the intracellular copper was sequestered and inaccessible to the 2,3,2-tetramine. Nevertheless, the 2,3,2-tetramine was shown to reduce injury and lipid peroxidation to a significant, albeit partial, extent, confirming that the excess copper played a role in the cell injury observed in this model. The protective effect ofα-tocopherol and partial protection of 2,3,2-tetramine are consistent with the postulated role of oxidant damage to the hepatocyte in the genesis of copper-induced hepatocyte injury.
This isolated copper-loaded hepatocyte model confirms on a cellular basis the prior observations of oxidant injury in livers removed from mammalian models of copper-overload and from humans with Wilson's disease(14–16, 23). By using two independent techniques to measure lipid peroxidation (lipid-conjugated dienes and TBARS), we have reported markedly increased peroxidation of mitochondrial lipids from dietary copper-overloaded rats(14, 15); from the Long-Evans Cinnamon rat(23), a naturally occurring inbred model of Wilson's disease(24); from Bedlington terriers(25) with copper toxicosis(16); and from patients with Wilson's disease undergoing liver transplantation(16). Combined with the morphologic changes of hepatic mitochondria observed in rats(14) and humans with copper overload(1, 2), these data suggest that the hepatic mitochondrion is an important target organelle during copper toxicity. Indeed, abnormal respiratory function of hepatic mitochondria, as demonstrated by perturbations of state 3 mitochondrial respiration and low activity of the respiratory chain protein complex, cytochrome C oxidase, have been demonstrated in mitochondria isolated from copper-overloaded rats(15). Although in this current study we did not determine the intracellular site of increased lipid peroxidation, the demonstrated close relationship between the degree of oxidative damage and loss of cell viability supports the role of oxidant injury suggested by the mitochondrial studies.
The results of this study suggest that antioxidants might be hepatoprotective during copper overload states, such as Wilson's disease and Indian childhood cirrhosis. It should, however, be noted that the levels of hepatocyte α-tocopherol achieved by in vitro incubation(6-fold increase in α-tocopherol content) may not be duplicated by oral supplementation of vitamin E in the intact rat(14). The limited absorption of ingested vitamin E supplements(26) and the avid transfer by the liver of absorbed vitamin E into nascent very low density lipoproteins(27) appear to limit increases of hepaticα-tocopherol content in vivo. It still remains to be determined if the achievable hepatic levels of α-tocopherol, other antioxidants alone or combined antioxidant treatment would be of value in human copper overload disorders. Thus, the possible therapeutic use of antioxidants in copper-overload states merits investigation. Finally, this isolated rat hepatocyte model of copper overload appears to be an excellent system in which to investigate the cellular pathogenesis of copper-induced hepatotoxicity.



Abbreviations
- TBARS:
-
thiobarbituric acid-reducing substances
- O˙2:
-
superoxide
- OH·:
-
hydroxyl radical
References
Sokol RJ 1994 Wilson's disease and Indian childhood cirrhosis. In: Suchy FJ (ed) Liver Disease in Children. CV Mosby, St. Louis, pp 747–772
Scheinberg IH, Sternlieb I 1984 Wilson's Disease. WB Saunders, Philadelphia
Bull PC, Thomas GR, Mommens JM, Forbes JR, Cox D 1993 The Wilson disease gene is a putative copper transporting P-type ATPase similar to the Menkes gene. Nature Genet 5: 327–337
Petrukhin K, Fischer SG, Pirastu M, Tanzi RE, Chernov I, et al 1993 Mapping, cloning and genetic characterization of the region containing the Wilson disease gene. Nature Genet 5: 338–343
Popper H, Goldfischer S, Sternlieb I, Nayak NB, Madhaven TV 1979 Cytoplasmic copper and its toxic effects-studies in Indian childhood cirrhosis. Lancet 1: 1205–1208
Lefkowitch JH, Honig CL, King ME, Hagstrom JWC 1982 Hepatic copper overload and features of Indian childhood cirrhosis in an American sibship. N Engl J Med 307: 271–277
O'Neill NC, Tanner MS 1989 Uptake of copper from brass vessels by bovine milk and its relevance to Indian childhood cirrhosis. J Pediatr Gastroenterol Nutr 9: 167–172
Yuzbasiyan-Gurkan V, Grider A, Nostrant T, Cousins RJ, Brewer GJ 1992 Treatment of Wilson's disease with zinc. X. Intestinal metallothionein induction. J Lab Clin Med 120: 380–386
Sternlieb I, Scheinberg IH 1968 Prevention of Wilson's disease in asymptomatic patients. N Engl J Med 278: 352–354
Sternlieb I 1984 Wilson's disease: indications for liver transplantation. Hepatology 4: 15s–17s
Schilsky ML, Scheinberg IH, Sternlieb I 1994 Liver transplantation for Wilson's disease: indications and outcome. Hepatology 19: 583–587
Tanner MS, Bhave SA, Pradham AM, Pandit AN 1987 Clinical trials of penicillamine in Indian childhood cirrhosis. Arch Dis Child 62: 1118–1124
Sokol RJ, Francis PO, Gold SH, Ford DM, Lum GM, Ambruso DR 1985 Orthotopic liver transplantation for acute fulminant Wilson disease. J Pediatr 107: 549–552
Sokol RJ, Devereaux M, Mierau GW, Hambidge KM, Shikes RH 1990 Oxidant injury to hepatic mitochondrial lipids in rats with dietary copper overload. Modification by vitamin E deficiency. Gastroenterology 99: 1061–1071
Sokol RJ, Devereaux MW, O'Brien K, Khandwala RA, Loehr JP 1993 Abnormal hepatic mitochondrial respiration and cytochrome c oxidase activity in rats with long-term copper overload. Gastroenterology 105: 178–187
Sokol RJ, Twedt D, McKim Jr JM, Devereaux MW, Karrer FM, Kam I, Von Steigman G, Narkewicz MR, Bacon BR, Britton RS, Neuschwander-Tetri BA 1994 Oxidant injury to hepatic mitochondria in patients with Wilson's disease and Bedlington terriers with copper toxicosis. Gastroenterology 107: 1788–1798
Sokol RJ, Devereaux MW, Traber MG, Shikes RH 1989 Copper toxicity and lipid peroxidation in isolated rat hepatocytes: effect of vitamin E. Pediatr Res 25: 55–62
Hill KE, Burk RF 1982 Effect of selenium deficiency and vitamin E deficiency on glutathione metabolism in isolated rat hepatocytes. J Biol Chem 257: 10668–10672
Twedt DC, Hunzaker HA, Allen KGD 1988 2,3,2-Tetramine as a hepatic copper chelator in the treatment of copper hepatotoxicity in Bedlington terrier dogs. Am J Vet Res 192: 52–56
Evenson MA, Warren BL 1975 Determination of serum copper by atomic absorption, with the use of the graphite cuvette. Clin Chem 21: 619–625
Southorn PA, Powis G 1988 Free radicals in Medicine. I. Chemical nature and biologic reactions. Mayo Clin Proc 63: 381–389
Sokol RJ, Devereaux M, Khandwala R, O'Brien K 1993 Evidence for involvement of oxygen free radicals in bile acid toxicity to isolated rat hepatocytes. Hepatology 17: 869–881
McKim JM Jr, Devereaux MW, Petersen DR, Hambidge KM, Ruyle SZ, Schilsky ML, Sternlieb I, Sokol RJ 1994 Mitochondrial oxidant injury in Long-Evans Cinnamon (LEC) rat liver containing high copper. Gastroenterology 106:A941.
Sokol RJ 1994 At long last-an animal model for Wilson's disease. Hepatology 20: 533–535
Twedt DC, Sternlieb I, Gilbertson SR 1979 Clinical, morphologic, and chemical studies on copper toxicosis of Bedlington terriers. J Am Vet Med Assoc 175: 269–275
Blomstrand R, Forsgren L 1968 Labelled tocopherols in man. Int J Vitam Nutr Res 38: 328–344
Traber M, Rudel L, Burton G, Hughes L, Ingold K, Kayden H 1990 Nascent VLDL from liver perfusions of cynomolgus monkeys are preferentially enriched in RRR-compared with SRR- tocopherol. Studies using deuterated tocopherols. J Lipid Res 31: 687–694
Acknowledgements
The authors thank Kenneth Allen, Ph.D., for providing the 2,3,2-tetramine, K. Michael Hambidge, M.D., for the copper analyses, and Joanna Lantzy and Cindy Wyman for typing the manuscript.
Author information
Authors and Affiliations
Additional information
Supported in part by National Institutes of Health Grants (R01DK38446, 1P30AM34914, R01DK12432) and the Abby Bennett Liver Research Fund.
Rights and permissions
About this article
Cite this article
Sokol, R., Mckim, J. & Devereaux, M. α-Tocopherol Ameliorates Oxidant Injury in Isolated Copper-Overloaded Rat Hepatocytes. Pediatr Res 39, 259–263 (1996). https://doi.org/10.1203/00006450-199602000-00012
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199602000-00012
This article is cited by
-
Decreased serum antioxidant capacity in patients with Wilson disease is associated with neurological symptoms
Journal of Inherited Metabolic Disease (2012)
