
Abstract
Acylcarnitines in amniotic fluid samples were analyzed for the prenatal diagnosis of propionic acidemia, methylmalonic aciduria, isovaleric acidemia, and glutaric aciduria by electrospray tandem mass spectrometry. Although the levels of the specific acylcarnitine between affected and unaffected cases showed an overlap, the ratios of propionylcarnitine to 4-carbon acylcarnitine levels for propionic acidemia and methylmalonic aciduria, those of isovalerylcarnitine to propionylcarnitine for isovaleric acidemia, and those of glutarylcarnitine to propionylcarnitine for glutaric aciduria type I were shown to be reliable indicators in the prenatal diagnosis. In addition, it is suggested that the combination of the ratios of glutarylcarnitine, isovalerylcarnitine, and hexanoylcarnitine to propionylcarnitine may be useful for the prenatal diagnosis of glutaric aciduria type II.
Similar content being viewed by others

Main
Prenatal diagnosis in disorders of organic acid metabolism has been done by a variety of means, demonstrating the accumulation of the specified organic acids(1) or acylcarnitines(2–5) in amniotic fluid or in the maternal urine(6, 7), and the deficiency of the corresponding enzyme(8, 9) or cofactor(10). Each measurement has its own advantages and disadvantages with respect to technical difficulty and safety in sampling, sensitivity or selectivity, contamination of maternal cells, cost, and so on. Thus, a combination of some of these means is thought to be helpful for the reliable diagnosis of these disorders.
Among these methods, acylcarnitine determination in amniotic fluids by fast atom bombardment and tandem mass spectrometry has been reported to be simple and convenient(4, 5). Recently, acylcarnitines have been analyzed also by ESI-MS/MS(11–13). However, the accumulation of diagnostic acylcarnitines in amniotic fluids appears to be quantitatively less pronounced than that of selected organic acids measured for the purpose of prenatal diagnosis. In this study, we measured acylcarnitines in relatively large numbers of amniotic fluid samples from pregnancies at risk for organic acidemias by ESI-MS/MS and investigated the accuracy of this method.
METHODS
Amniotic fluids were collected from high risk pregnancies for propionic acidemia, methylmalonic acidemia, isovaleric acidemia, and glutaric acidurias(Table 1), and were tested also by gas chromatography/mass spectrometry(14). The diagnosis was confirmed by enzyme assays or by organic acid analysis after birth.
L-[methyl-2H3]Carnitine was obtained from Cambridge Isotope Laboratories (Woburn, MA).[methyl-2H3]3Carnitine was synthesized from 4-amino-3-hydroxybutyric acid (Nacalai Tesque, Kyoto, Japan) and[methyl-2H3]iodomethane (Campro Scientific, Veenendaal, The Netherlands). Acetylcarnitine, propionylcarnitine, butyrylcarnitine, isovalerylcarnitine, hexanoylcarnitine, octanoylcarnitine, glutarylcarnitine, acetyl-[methyl-2H3]carnitine, propionyl-[methyl-2H3]carnitine, butyryl-[methyl-2H3]carnitine, isovaleryl-[methyl-2H3]3carnitine, hexanoyl-[methyl-2H3]3carnitine, octanoyl-[methyl-2H3]3carnitine, and glutaryl-[methyl-2H3]3carnitine were synthesized according to previously reported methods(15, 16). Methanolic hydrogen chloride (3 mol/L) was purchased from Supelco (Bellefonte, PA).
A mixture of 200 μL of amniotic fluid, internal standards, and 1.0 mL of cold ethanol was centrifuged at 10,000 × g for 10 min. The concentrations (nanomoles/1 mL of amniotic fluid) of internal standards were as follows: 3 of acetyl-[methyl-2H3]carnitine, 2 (or 10 for samples with high propionylcarnitine concentrations) of propionyl-[methyl-2H3]carnitine, 1 of butyryl-[methyl-2H3]carnitine, 1 (or 10) of isovaleryl-[methyl-2H3]3carnitine, 0.5 of hexanoyl-[methyl-2H3]3carnitine, 0.5 of octanoyl-[methyl-2H3]carnitine, and 0.5 (or 2) of glutaryl-[methyl-2H3]3carnitine. The supernatant was dried under nitrogen stream, and the dry residue was derivatized with 100 μL of methanolic HCl (3 mol/L) at 65°C for 15 min. The sample was dried again under nitrogen stream and redissolved in 50 μL of methanol.
Flow injection analysis was done, using a methanol flow (25 mL/min) with a model LC-10AD liquid chromatograph (Shimadzu, Kyoto, Japan), which was introduced through a fused silica capillary column into the ESI interface of a model TSQ-7000 tandem quadrupole mass spectrometer (Finnigan MAT Instrument Inc., Tokyo, Japan), and 5 mL of sample were injected manually using a 7725 injector (Rheodyne, Cotati, CA). The ESI voltage was 4.5 kV, and the capillary temperature was kept at 200°C. Argon was used as the collision gas in the second quadrupole at a pressure of 0.5 milliTorr and 30 eV collision energy. MS/MS measurement was done with unit mass resolution. The scan range and speed of the first quadrupole were m/z 200 to 400 per 3 s. The data in the precursor-ion scanning with product ion m/z 99, which is common to acylcarnitine methyl esters and used to improve the specificity and sensitivity of the measurement(17), were acquired in the continuum mode. The heights of the ions corresponding to the selected acylcarnitines during the appearance of the sample (about 20 scans) were averaged. Quantitative analysis of each acylcarnitine was done using the ratio of the averaged ion intensity of each acylcarnitine to that of the corresponding internal standard. The intra- and inter-day variations were determined using two sets of seven aliquots of a control amniotic fluid sample spiked with known (different in each set) amounts of synthesized acylcarnitines, which were stored in each vial at -80°C and processed after adding a fixed amount of internal standards.
RESULTS
Typical ESI-MS/MS spectra of amniotic fluid samples were shown in Figure 1. Correlation coefficients of calibration curves for selected acylcarnitines and coefficients of variation in the measurements were listed in Table 2.

Typical electrospray tandem mass spectra (precursor-ion scanning using product ion m/z 99) of methylated amniotic fluid samples of a control (A), a case with glutaric aciduria type I (B), and with glutaric aciduria type II (C). Peak identifications are as follows: C2, acetylcarnitine; C3, propionylcarnitine;C4, C4 acylcarnitines, C5, C5 acylcarnitines;C6, C6 acylcarnitines; C8, C8 acylcarnitines;Gl, 5-carbon dioylcarnitine. Peaks indicated by * are deuterium-labeled internal standards for the corresponding acylcarnitines; see text.
Figure 2 shows the relationship between the amniotic fluid levels of propionylcarnitine and those of C4 acylcarnitines in controls and pregnancies at risk for propionic acidemia and methylmalonic aciduria. The affected cases was discriminated from the unaffected cases and controls by the ratios of propionylcarnitine level to C4 acylcarnitine level, not by propionylcarnitine levels or by the ratios of propionylcarnitine level to acetylcarnitine level (data not shown). The levels of propionylcarnitine were correlated with those of methylcitric acid in pregnancies at risk for propionic acidemia (r2 = 0.62), and with those of methylmalonic acid for methylmalonic aciduria (r2 = 0.83). The levels of C4 acylcarnitines were not correlated significantly with the gestational weeks, the sample storage periods or the protein concentrations of amniotic fluids in these groups.

The relationship between the amniotic fluid levels of propionylcarnitine and those of C4 acylcarnitines in controls (▵) and pregnancies at risk for propionic acidemia (•, affected; ○, unaffected) and methylmalonic aciduria (▪, affected; □, unaffected).
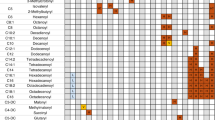
Figure 3 shows the ratios of propionylcarnitine to C4 acylcarnitine, those of C5 acylcarnitine to propionylcarnitine, and those of C5 dioylcarnitine to propionylcarnitine as indices for prenatal diagnosis of propionic acidemia, methylmalonic aciduria, isovaleric acidemia, and glutaric aciduria, respectively. The means and SD or ranges of the ratios in propionic acidemia (propionylcarnitine/C4 acylcarnitine) were 12.5 ± 2.5(affected), 2.00 ± 0.79 (unaffected), 1.60 ± 0.34 (control), those in methylmalonic aciduria (propionylcarnitine/C4 acylcarnitine), 10.6± 1.8 (affected), 1.64 ± 0.51 (unaffected), those in isovaleric acidemia (C5 acylcarnitine/propionylcarnitine), 6.4 ± 3.0 (affected), 0.52 ± 0.11 (unaffected), 0.38 ± 0.14 (control), those in glutaric aciduria type II (C5 acylcarnitine/propionylcarnitine), 1.53-5.57(affected), 0.32-0.51 (unaffected), those in glutaric aciduria type I (C5 dioylcarnitine/propionylcarnitine), 2.11-2.86 (affected), 0.03-0.18(unaffected), 0.06 ± 0.03 (control), those in glutaric aciduria type II, 0.23-0.42 (affected), 0.05-0.10 (unaffected). Z scores for the lowest ratios in the affected and the highest ones in the unaffected pregnancies were as follows; 17.1 and 4.6 for propionylcarnitine/C4 acylcarnitine in propionic acidemia, 26.9 and 1.7 in methylmalonic aciduria, 26.9 and 1.7 for C5 acylcarnitine/propionylcarnitine in isovaleric acidemia, 8.3 and 0.91 in glutaric aciduria type II, 81 and 4.5 for C5 dioylcarnitine/propionylcarnitine in glutaric aciduria type I, 6.5 and 1.5 in glutaric aciduria type II, 4.7 and-0.2 for C6 acylcarnitine/propionylcarnitine in glutaric aciduria type II.

The ratios of the selected acylcarnitines to the propionyl- or C4-acylcarnitine for prenatal diagnosis in propionic acidemia(PA), methylmalonic aciduria (MMA), isovaleric acidemia(IVA), glutaric aciduria type I (GA-I), and glutaric aciduria type II (GA-II). Control ranges indicated with bar show mean ± 3 SD. (+), affected; (-), unaffected.
DISCUSSION
For quantitative assay of acylcarnitines in amniotic fluids by tandem mass spectrometry, fast atom bombardment as an ionization method has been used(4, 5). However, the latest applications of ESI-MS/MS for acylcarnitine profiling in blood spots indicated that this method is specific and accurate for the diagnosis of organic acidemias(13). In the present study, we showed that this method provides high sensitivity and accuracy similar to the former one, in the measurement of acylcarnitines in amniotic fluid samples, too.
The results obtained in our study clearly indicated that the concentrations of the specific acylcarnitine should be corrected by the other acylcarnitines for the reliable prenatal diagnosis of organic acidemias. In a previous study of prenatal diagnosis of propionic acidemia(5), a relatively high level of propionylcarnitine in the amniotic fluid of a possible heterozygote was reported. In the present study, unfortunately, we are also not sure whether the unaffected case with a high propionylcarnitine level, shown in Fig. 2, is a heterozygote for propionic acidemia. For practical purposes in prenatal diagnosis, however, it seems important to emphasize that the accumulation of the specific acylcarnitines in amniotic fluids seems to be less marked than that of the other metabolites in organic acidemias and that the concentrations of metabolites in amniotic fluids should be standardized as urinary levels of metabolites being corrected for by the creatinine concentration. Thus, it is thought to be convenient to use acylcarnitine levels measured simultaneously for the standardization.
Although the results in our earlier study(4) suggested that the ratio of the levels of the specific acylcarnitine to those of acetylcarnitine might be more useful than the former levels themselves, it was less reliable than the ratios proposed in the present study using larger numbers of samples, partly because acetylcarnitine levels tended to be lower in samples stored for long periods than those of the other acylcarnitines(18).
Based on the Z scores shown in this study, thus, we believe that the ratios of the index acylcarnitines to the other selected acylcarnitines permit reliable prenatal diagnosis in pregnancies at risk for propionic acidemia, methylmalonic acidemia, isovaleric acidemia, and probably glutaric aciduria type I in clinical settings, although we have tested few samples without prior knowledge of the results obtained by other methods. Even in the first trimester of gestation, affected amniotic fluids contained significantly high values of the ratios mentioned above, the usefulness of which should be confirmed in further analysis. For glutaric aciduria type II, however, the lowest Z scores of the ratios of C5 acylcarnitine to propionylcarnitine and those of C5 dioylcarnitine to propionylcarnitine in affected cases may not be large enough for reliable diagnosis. Although the combination of these values of C5 dioylcarnitine, C5 acylcarnitine, and C6 acylcarnitine seems promising, further analysis in pregnancies at risk for this disorder will be necessary.
Abbreviations
- ESI:
-
electrospray ionization
- ESI-MS/MS:
-
electrospray tandem mass spectrometry
- C4, C5, C6, C8:
-
4-, 5, 6, and 8-carbon
- Z score:
-
multiples of the SD above the mean of controls
References
Jakobs C, Brink HJ, Stellaard F 1990 Prenatal diagnosis of inherited metabolic disorders by quantitation of characteristic metabolites in amniotic fluid: factors and future. Prenat Diagn 10: 265–271.
Penn D, Schmidt-Sommerfeld E, Jakobs C, Bieber LL 1987 Amniotic fluid propionylcarnitine in methylmalonic acidemia. J Inhert Metab Dis 10: 376–382.
Sugiyama N, Kidouchi K, Kobayashi M, Wada Y 1990 Carnitine deficiency in inherited organic acid disorders and Reye syndrome. Acta Paediatr Jpn 32: 410–416.
Shigematsu Y, Kikawa Y, Sudo M, Kanaoka H, Fujioka M, Ma D 1991 Prenatal diagnosis of isovaleric acidemia by fast atom bombardment and tandem mass spectrometry. Clin Chim Acta 203: 369–374.
Van Hove JLK, Chace DH, Kahler SG, Millington DS 1993 Acylcarnitines in amniotic fluid: application to the prenatal diagnosis of propionic acidemia. J Inhert Metab Dis 16: 361–367.
Aramaki S, Lehotay D, Nyhan WL, MacLeod PM, Sweetman L 1989 Methylcitrate in maternal urine during a pregnancy with a fetus affected with propionic acidaemia. J Inhert Metab Dis 112: 86–88.
Sakuma T, Sugiyama N, Ichiki T, Kobayashi M, Wada Y, Nohara D 1991 Analysis of acylcarnitines in maternal urine for prenatal diagnosis of glutaric aciduria type 2. Prenat Diagn 11: 77–82.
Gompertz D, Goodey PA, Thom H, Russell G, Johnston AW, Mellor DH, MacLean MW, Ferguson-Smith ME, Ferguson-Smith MA 1975 Prenatal diagnosis and family studies in a case of propionic acidemia. Clin Genet 8: 244–250.
Fowler B, Giles L, Sardharwalla IB, Donnai P, Clayton JK 1988 First trimester diagnosis of methylmalonic aciduria. Prenat Diagn 8: 207–213.
Yamaguchi S, Shimizu N, Orii T, Fukao T, Suzuki Y, Maeda K, Hashimoto T, Previs SF, Rinaldo P 1991 Prenatal diagnosis and neonatal monitoring of a fetus with glutaric aciduria type II due to electron transfer flavoprotein (-subunit) deficiency. Pediatr Res 30: 439–443.
Kelly BM, Rose ME, Wycherley D 1992 Electrospray mass spectra of medium-chain and long-chain acylcarnitine. Org Mass Spectrom 27: 924–926.
Rashed MS, Ozand PT, Harrison ME, Watkins PJF, Evans S 1994 Electrospray tandem mass spectrometry in the diagnosis of organic acidemias. Rapid Commun Mass Spectrom 8: 129–133.
Rashed MS, Ozand PT, Bucknall MP, Little D 1995 Diagnosis of inborn errors of metabolism from blood spots by acylcarnitines and amino acids profiling using automated electrospray tandem mass spectrometry. Pediatr Res 38: 324–331.
Jakobs C 1989 Prenatal diagnosis of inherited metabolic disorders by stable isotope dilution GC-MS analysis of metabolites in amniotic fluid: review of four years experience. J Inhert Metab Dis 2( suppl): 267:27270.
Bohmer T, Bremer J 1968 Propionylcarnitine. Physiological variations in vivo. Biochim Biophys Acta 152: 559–567.
Pourfarzam M, Bartlett K 1991 Synthesis, characterisation and high-performance liquid chromatography of C6-C16 dicarboxylyl-mono-coenzyme A and -monocarnitine esters. J Chromatogr Biomed Appl 570: 253–276.
Millington DS, Norwood DL, Kodo N, Roe CR, Inoue F 1989 Application of fast atom bombardment with tandem mass spectrometry and liquid chromatography/mass spectrometry to analysis of acylcarnitines in human urine, blood, and tissue. Anal Biochem 180: 331–339.
Schmidt-Sommerfeld E, Penn D, Duran M, Bennett MJ, Santer R, Stanley CA 1993 Detection of inborn errors of fatty acid oxidation from acylcarnitine analysis of plasma and blood spots with the radioisotopic exchange-high-performance liquid chromatographic method. J Pediatr 122: 708–714.
Author information
Authors and Affiliations
Additional information
Supported in part by Morinaga Hoshikai.
Rights and permissions
About this article
Cite this article
Shigematsu, Y., Hata, I., Nakai, A. et al. Prenatal Diagnosis of Organic Acidemias Based on Amniotic Fluid Levels of Acylcarnitines. Pediatr Res 39, 680–684 (1996). https://doi.org/10.1203/00006450-199604000-00020
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199604000-00020
This article is cited by
-
Antenatal manifestations of inborn errors of metabolism: biological diagnosis
Journal of Inherited Metabolic Disease (2016)
-
Spectrométrie de masse en biologie médicale: principes et applications
Bio tribune magazine (2011)
