
Abstract
Prolongation of the QT interval in the ECG can be induced in d 17 chick embryos by ablating the nodose placode on the right side on d 1 of development. The nodose placode contains the precursor cells which from the neurons of the nodose (inferior vagal) ganglion. Neurons in this ganglion provide sensory innervation to the heart and other viscera. In this study, we measured ganglion volume and neuron size and number in the right and left nodose ganglia in d 17 experimental and control embryos from whom electrocardiograms had been obtained. A significant reduction in the number of neurons present in the right nodose ganglion, relative to the left ganglion, was evident in all embryos with abnormally prolonged QT intervals. Embryos with prolonged QT, as well as lesioned embryos who demonstrated normal QT on d 17, also had abnormally small neurons in both right and left nodose ganglia, indicating an additional nonspecific, perhaps permissive, effect of the lesion. These results suggest that abnormal development of the sensory innervation of the heart may be an important link in the chain of events leading to the developmental long QT syndrome expressed by these embryos.
Similar content being viewed by others

Main
The long QT syndrome is a life-threatening heart condition, often associated with severe bouts of ventricular tachycardia and presumed to be the cause in some cases of otherwise unexplained sudden death. In more benign manifestations, patients come to medical attention because of spells of dizziness or fainting, or when routine electrocardiographic screening reveals an abnormally prolonged interval between the onset of the Q wave and the end of the T wave in the ECG. Although the syndrome can be diagnosed by this phenomenologic criterion, what the altered ECG signifies in terms of the abnormality in the heart remains a subject of debate. Some analyses suggest that the T wave duration is increased, due to a prolongation of the repolarization phase of the cardiac cycle(1, 2). Others have proposed that the subsequent U wave is abnormally large and early in the ECG, due to increased after-depolarizations in cardiac muscle fibers(3–7).
In addition to the lack of resolution about the significance of the ECG alteration for cardiac function, there is also a lack of consensus about the underlying cause of the syndrome(5, 8). One body of clinical and basic research has highlighted a central role for an abnormality in the sympathetic component of cardiac innervation, particularly a sympathetic hyperactivity(5, 9–12). Not only are many symptomatic episodes (e.g. dizziness, fainting, arrhythmias), and sometimes sudden death, often associated with behavioral indicators of an increase in sympathetic activation, but patients are frequently(10, 13, 14) helped by interventions to decrease sympathetic activity. These interventions are not always successful(15–17), however, and other studies have produced results undermining the idea that sympathetic hyperactivation is the definitive abnormality in this syndrome. Results of one recent study indicate that decreased, not increased, sympathetic activity is associated with ventricular tachycardia(18). Furthermore, experimental manipulations, which decrease, rather than increase, cardiac sympathetic innervation during development, produce neonatal rats with prolonged QT intervals(19).
An alternative view of the involvement of the sympathetic system in the etiology of long QT syndrome has been proposed, in response to other physiologic investigations. In these studies, sympathetic activation has been proposed as a “triggering” mechanism, which unmasks an underlying error in cardiac muscle function(20–22). Reports of potential intracardiac abnormalities correlated with prolonged QT intervals have ranged from findings of increased numbers of undifferentiated myoblasts in affected hearts(23), to indications of specific genetic defects affecting the numbers and/or functional characteristics of K+ and Na+ channels in cardiac myocyte membranes(24, 25). In addition, the possibility that other aspects of cardiac innervation may be involved in this syndrome is raised by one study which reported that patients with low parasympathetic, but presumably normal sympathetic, activity have an increased risk of sudden death(26).
A unifying hypothesis which might resolve these contradictions suggests that abnormal development of cardiac sympathetic innervation has both a direct effect itself and also initiates a cascade of biochemical and molecular abnormalities during development of the heart which has a permanent impact on its function(27). To evaluate such a hypothesis adequately, a model system, in which analysis at these various levels is feasible, is necessary. Our laboratory has recently described a chick embryo model of human long QT syndrome(28, 29). In our studies, ablation of the nodose placode unilaterally on the right side early in development (d 1) resulted in embryos with prolonged QT intervals, measured as the embryo approached hatching (d 17). The nodose placodes are ectodermal thickenings lateral to the developing neural tube which contain the precursors for the neurons which normally populate the nodose ganglia. The nodose ganglion, which is the inferior vagal ganglion, provides sensory innervation to the heart and other viscera(30). In initial histologic evaluation of our model, we documented that, although the right nodose placode ablation is apparently often lethal, experimental embryos which survive to d 12 develop a right nodose ganglion that is populated with neurons, but the ganglion and the neurons are abnormal(31). In the present study, we asked whether a morphologically abnormal right nodose ganglion is specifically associated with prolongation of the QT interval. To this end, we recorded four-lead ECG and measured QT and RR intervals for experimental and sham-operated control chick embryos at d 17, by which time all components of the adult pattern of cardiac peripheral innervation are normally established and functional(32–36). We used morphometric methods to determine the volume of right and left nodose ganglia, and the number and size of nodose ganglion cells, in these embryos.
METHODS
Microsurgery. Fertilized Arbor Acre chicken eggs were obtained fresh from the hatchery (Seaboard Hatcheries, Athens, GA). The eggs were incubated in force-draft incubators maintained at 37°C and 95% humidity. At about 30-36 h of incubation, eggs were opened with a horizontal sander, a neutral red-impregnated piece of agar was placed over the embryo to stain it lightly, and the vitelline membrane was torn to allow access to the embryo(37). In embryos at Hamburger-Hamilton stages 8-10, the right nodose placode was removed by microcautery. Details of the surgical procedure and histologic verification of its effectiveness in removing the selected tissue have been described elsewhere(28, 31, 38). Briefly, the ectoderm covering somites 1-3 and extending laterally from the neural tube for approximately 1 mm, and rostrally to the mid-otic placode level, was cauterized on the right side to ablate the placode unilaterally.Figure 1 illustrates the location of the nodose placodes in embryos at this age(30). All placode lesions were restricted as much as possible to ectodermal tissue, which lies lateral to the neural tube and to the premigratory neural crest precursors. With one exception, hearts were evaluated for any structural defects indicative of unintentional damage more medially, in the region of the cardiac neural crest(39–41), after the embryo was killed at the end of the experimental procedures. (The heart of one embryo in the sham group was not available for analysis, due to an error in tissue handling during histologic processing.)

Diagram of the embryonic origins of cardiac innervation in the chick. On the left, coded graphically to match their embryonic sites of origin, are shown the adult derivatives of the embryonic structures shown on the right. The nodose placode provides the neuronal precursors to the nodose ganglion, which provides sensory innervation to the heart via the vagus nerve(30). (In the adult chicken, these fibers terminate centrally in the nucleus of the solitary tract.) The cardiac ganglia of the heart, containing the postganglionic parasympathetic neurons, are derived from precursors in the cardiac neural crest(50). The preganglionic parasympathetic fibers of the vagus nerve originate in neuronal somata in the medulla (dorsal motor nucleus of the vagus, in the adult). The sympathetic postganglionic innervation is primarily via the T1 sympathetic ganglion(51–53), whose neurons are derived from the cardiac sympathetic neural crest(32, 50). [This region of neural crest also contributes to many other sympathetic ganglia(54).] Neurons in the T1 dorsal root ganglion (DRG), also derived from neural crest precursors(55), probably provide a small“sympathetic afferent” innervation to the heart(56, 57). Fibers from these latter two ganglia reach the heart via the cardiac nerves(58). Fibers of the vagus nerve reach the heart between 3.5 and 4.5 d of incubation(32, 36). The parasympathetic innervation is functional by about d 12(34). The sympathetic innervation develops considerably later, about d 10 or 11(35, 59), but is functional by embryonic d 16(32, 33). The avian heart generally has a comparatively rich parasympathetic innervation, especially of the ventricle(60). The chick sympathetic innervation, on the other hand, seems to be rather restricted, even compared with other avian species(61).
After the surgical manipulation, the eggs were sealed with cellophane tape and returned to the incubator. Sham-operated control embryos were treated identically, except that the egg was resealed and returned to the incubator immediately after the vitelline membrane was opened.
In initial experiments, unilateral left placode ablations and bilateral placode ablations were also performed. Left and bilateral placode ablations were discontinued, however, as embryo mortality was virtually 100% after these two procedures. Embryos having only right placode ablations survived to d 17 in sufficient numbers for experimental analysis.
Electrocardiography. At embryonic d 17, three-lead ECG were recorded from surviving embryos. For the majority of embryos, the methods used were identical to those used in a previous study(28). In these cases, the eggs were maintained at 37.0 ± 1.0°C in a humidified incubator during the course of the recording. Three stainless steel wire recording electrodes and a ground reference electrode were inserted through small holes in the egg shell. Signals were amplified and recorded on a 2-channel chart recorder (RS 3200 with Universal amplifiers model 13-4615-58, Gould, Inc., Cleveland, OH), using a switchbox to select which of the three possible pairs of leads was recorded. Chart records were collected until 3-5 intervals of 10 consecutive beats were recorded without baseline shifts or artifacts from movement of the embryo, from each of the three pairs of electrodes sequentially. Intervals between the peaks of the R waves in consecutive QRS complexes and intervals between the onset of the Q wave and the offset (return to baseline) of the T wave were measured directly from the chart records using calipers. The RR and QT intervals were averaged for the best set of 10 consecutive beats recorded from each pair of leads. The measured QT intervals were corrected for heart rate using the formula QTc = QT/(RR)1/2(28, 42).
More recently, ECG were recorded using a computerized method which both improved the accuracy of measuring the RR and QT intervals by reducing the signal-to-noise ratio and performed the averaging function automatically. Using the window made in the egg shell during microsurgery, the legs and wings of the embryos were withdrawn one at a time. A topical anesthetic (Cetacaine; Cetylite Industries, Inc., Pennsauken, NJ) was applied to the skin and fine silver wire (0.12 mm outside diameter, insulated with Teflon except for the tip) recording electrodes were inserted under the skin and sutured in place. The limb was then reinserted into the shell. The embryo's temperature was monitored on a Bat-12 unit equipped with a small thermistor on a flexible lead(Bailey Instruments, Inc., Saddlebrook, NJ) which was directly inserted into the egg through the window. Analog output of the unit was fed to a servo-controlled DC heater set at 37°C which was part of the egg holder. When all leads were inserted, the window in the egg shell was resealed with cellophane tape, and the door to the electrically shielded recording chamber was shut. The ECG responses from each of three pairs of leads were amplified at 2.5K via 3 Grass P-511 amplifiers (series K, Grass Instruments, Quincy, MA) and recorded simultaneously directly on to computer disk, using RC Electronics, Inc. (Santa Barbara, CA) Enhanced Graphics Acquisition and Analysis software. Approximately 60 s of data were recorded initially, usually followed by a 10-20-min interval and a second 60-s recording period. ECG were subsequently analyzed off-line, using the signal averaging component of the software. Short intervals of about 10-20 heart beats drawn from the beginning, middle, and end of the recording period were averaged initially and compared, to ensure that no changes had occurred in the ECG over the recording session. ECG cycles from the entire recording period where then averaged, those cycles during which movement or other artifacts had occurred being excluded from the average by the artifact rejection features of the software. Measurements of QT and RR intervals were made with cursors directly on the computer screen on raw or signal-averaged wave forms. Figure 2 illustrates a portion of a raw ECG record and the signal-averaged ECG result produced by this computerized method.

Digitized raw and averaged ECG recordings from a 17-d chick embryo, illustrating display and analysis procedures using the RC Electronics EGAA software. The middle trace shows a segment of the digitized raw ECG recording (RAW ECG), with the triggering threshold for the window discriminator software also indicated (TRIG LEVEL). The top trace shows the trigger pulses generated by the software (TRIG PULSE), which are synchronized to the rising phase of the R wave. The averaging window extended for 120 ms before the trigger pulse and 400 ms after the trigger pulse, encompassing two complete cardiac cycles. The averaged record for 200 consecutive cardiac cycles is shown in the bottom trace(AVG ECG). The length of this averaged QT interval is measured automatically by moving cursors (vertical lines) to the onset of the Q wave and to the end of the T wave, as illustrated (numerical readout not shown). In this illustration, the QT interval (double-headed arrow) measured 146 ms, the RR interval was 244 ms, and QTc = 0.146/(0.244)1/2 = 0.296.
Identifying long QT embryos. To define the normal QT interval in embryonic chicks of this age in our recording conditions, ECG were recorded from a group of 15 unoperated 17-d embryos whose shells were windowed for the first time immediately preceding the recording. The QT intervals were analyzed by computer and corrected as described above, and the RR intervals were converted to heart rate (beats/min) by dividing the RR interval, measured in milliseconds, by 60,000 (ms/min). These measures were compared with those of a group of 15 sham-operated control embryos, surgically prepared on embryonic d 1. As there was no difference in either measure between these two groups (see Results; Table 1), we defined a QTc interval greater than the longest interval measured in the normal group as a prolonged QT interval.
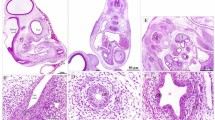
Histologic procedures. At the conclusion of the ECG measurements, the chick embryos were overdosed with Nembutal and perfused through a small needle inserted into the left ventricle with saline followed by 4% paraformaldehyde in 0.1 M phosphate buffer (pH 7.4). The embryos were immersed in the same fixative overnight, and their right and left nodose ganglia were removed, postfixed in 1% aqueous osmium tetroxide, and embedded in a water-soluble plastic (Historesin; Leica Instruments GmbH, Heidelberg, Germany). Serial sections through each ganglion were cut at 4 μm, mounted on glass slides, and stained with toluidine blue.
Morphometric measurements. The sections were viewed with a light microscope equipped with a televison camera. The images were captured on a television monitor and analyzed using JAVA morphometric software (Jandel, Inc., San Rafael, CA). The outline of the ganglion was traced on the monitor screen and entered into the computer for every section through the ganglion. The area of each section was automatically calculated by the pixel addition-based algorithm of the software. Section areas were summed for the whole ganglion, and the total area was multiplied by section thickness (4μm) to determine ganglion volume.
Sections equal to 10% of the total volume of the ganglion were selected for measurement of individual ganglion cells. The selection was done in a systematically random fashion, so that the sections were equally spaced through the ganglion to avoid a bias due to regional differences in ganglion cell sizes. The areas of all ganglion cell profiles containing a nucleolus were measured in each of these sections. Measuring only ganglion cells with a nucleolus was done to optimize the likelihood of measuring cells at the site of maximum diameter.
The number of cells for which areal measurements were made for each ganglion was summed and multiplied by 10 (because 1/10 of the ganglion volume had been sampled for cells) to generate an uncorrected count of neurons per ganglion. This count was corrected for split nucleoli using the formulaN = {t/[t + 2(r2 -(k/2)2)1/2]} × Ni wheret is section thickness, r is the average diameter of the nucleolus, k is the smallest detectable nucleolar fragment, andNi is the uncorrected cell number(43). In these sections, the average value of r was 3.44 μm and ofk was 0.25 μm. Given a section thickness of 4 μm, this formula produced a correction factor of 0.37 which was applied to the uncorrected counts for each of the ganglia examined.
RESULTS
Table 1 summarizes the means and standard deviations of QTc and RR measurements for the group of embryos used to define the normal range for these measures in d 17 chick embryos and the group of sham-operated embryos with which they were compared. There was no statistically significant difference on either measure between the group of embryos opened for the first time on d 17 (normal), and the sham group(t test). QTc measurements ranged from 0.294 to 0.327 ms for the normal group, and from 0.278 to 0.326 in the sham group. Therefore, a QTc interval greater than 0.327 ms was defined as a prolonged QT interval.
Approximately 200 dozen eggs were incubated and opened at embryonic d 1 during the course of this study. A total of 363 survived to embryonic d 17 and had an ECG recorded and analyzed. Of these, 25% were excluded from evaluation due to either technical problems with the recording, apparent gross anatomical abnormalities (such as ancephalocele and ectopia cordis, among others), or electrocardiographic abnormalities other than prolonged QT intervals(i.e. premature atrial contractions; fewer than 10 embryos were in this latter category). Another 25% (96) were sham-operated embryos. Prolonged QT intervals (QTc > 0.327 ms) were found in 80 of the experimental embryos included in the study, whereas 95 had normal QT intervals.
The right and left nodose ganglia were dissected and examined in all embryos. However, in three experimental embryos with prolonged QT intervals no right nodose ganglion could be found. The left nodose ganglion appeared to be normally developed in these three embryos. In one of these embryos, a very small swelling in the vagus nerve resembling a ganglion-like structure was found on the right side, but on serial sectioning through this structure and the adjacent vagus nerve, no neuronal cell bodies were seen. The remaining two embryos had no grossly definable right ganglion structure at all. Sections through a considerable length of the right vagus nerve failed to reveal any neurons in either embryo. Right and left nodose ganglia were easily identified in all sham-operated and experimental embryos with normal QT intervals at d 17.
Morphometry was carried out on right and left nodose ganglia of four sham-operated embryos (sham group), three embryos which had nodose placode lesions but had normal QT intervals (NormQT-RTNP group), and three embryos with right placode lesions which had developed right ganglia and had prolonged QT intervals (LQT-RTNP group). The nodose ganglia of the first sham-operated embryo, for which complete data were collected and for which no reasons for exclusion were found, were analyzed morphometrically. Subsequently, one embryo was randomly selected for morphologic analysis from each group (sham, NormQT-RTNP, and LQT-RTNP) from the pool of embryos collected in the intervening weeks. When morphologic analysis was completed on these three embryos, the random selection was iterated twice more, each time from a new pool of embryos. This assured a random selection, although distributing the samples systematically over embryos from different layings at different seasons.
In Table 2, the heart rate and QTc of each embryo used for morphometric analysis are shown. Nodose placode lesions have previously been documented to result in structurally normal hearts(44, 45); nonetheless, we evaluated the hearts in this group of embryos for structural defects. As shown inTable 2, ventricular septal defects were found in two embryos, one in the NormQT-RTNP group and one in the sham group. No defects were found in hearts of LQT-RTNP embryos. The occurrence of the ventricular septal defect in the NormQT-RTNP embryo may be indicative of unintentional damage to the neural crest during placode ablation surgery in this embryo, as the incidence of this defect has been reported to be higher in embryos with neural crest lesions than in sham-operated embryos(40). However, ventricular septal defect is also the most common heart defect seen in sham-operated embryos(39), as our finding of one sham embryo with the same defect attests. In one experimental embryo not used for morphometric analysis (and hence not included in Table 2) because the right ganglion was completely absent, defects of the cardiac outflow consistent with tetralogy of Fallot were found. These defects indicate that the cardiac neural crest was damaged during surgery in this one embryo.
Table 3 summarizes the measurements of nodose ganglion volume, ganglion cell cross-sectional area, and ganglion cell number in these embryos. As is evident from inspection of the table, in embryos with prolonged QT intervals, both right and left ganglion volume and mean cell area were reduced by about 50% compared with the control sham group. The values for the NormQT-RTNP embryos, which had the lesion but not the cardiac abnormality, were intermediate between those of the other two groups. One-way analyses of variance on right and left nodose ganglion cell area indicated a significant effect of group (F = 7.913; df = 2, 7; p < 0.02): F = 8.393; df = 2,7; p < 0.02, for right and left areas, respectively), with post hoc multiple comparison tests indicating that both experimental groups were significantly different form the control group (Newman-Keuls test: p < 0.05), but not different from each other (Fig. 3A). There were no significant differences in mean cell area in right versus left ganglia within any of the groups (t test, p = 0.80, 0.40, 0.54, for sham, NormQT-RTNP, and LQT-RTNP groups, respectively).

Comparisons of right and left nodose ganglion cells in control and experimental chick embryos. (A) Ganglion cell size. The size of neuronal cell bodies in the nodose ganglion was estimated from area measurements of cell profiles in sections representing 10% of the ganglion volume. The mean areas of ganglion cell profiles in the two experimental groups were significantly lower than that of the sham (control) group, but were not significantly different from each other (p < 0.05, Newman-Keuhls post hoc test). There were no right vs left differences in ganglion cell size within any of the groups. (B) Ganglion cell number. The number of cells in each ganglion was estimated by counting all profiles containing a nucleolus in the same set of sections through the ganglion used for cell size measurements. Raw counts were multiplied by 10 (as 10% of ganglion volume was sampled) and then corrected for split nucleoli(43). The number of neurons present in right nodose ganglia of both experimental groups was significantly reduced compared with controls. Only the experimental group with prolonged QT intervals showed a significant difference between right and left nodose ganglia in the estimated number of neurons. Asterisk (*) = significantly different from control (sham); + = significantly different from each other.
Measurements of ganglion volume were rather variable for some of the groups, and in a one-way analysis of variance, the main effect of group on nodose ganglion volume was not significant for right or left ganglia. Nonetheless, a t test indicated that the LQT-RTNP ganglia, both right and left, were significantly smaller than those of the sham-treated(p < 0.05 for both comparisons).
The results pertaining to nodose ganglion cell number had a distinctly different pattern than the other two measures (Table 2). In left nodose ganglia, there was no significant effect on cell number across the three groups (one-way analysis of variance, F = 2.211;df = 2, 7; p = 0.18). In the right ganglia, on the other hand, there was a significant difference between groups in ganglion cell number (F = 5.607; df = 2, 7; p < 0.05). The right nodose ganglia of embryos in both experimental groups had significantly fewer cells than those of sham-operated controls (p < 0.05 for both comparisons). More importantly, examination of differences in right and left nodose ganglion cell number indicated that embryos with prolonged QT intervals, unlike embryos in either of the other two groups, had fewer ganglion cells in the right ganglion than in the left one(Fig. 3B). Analysis of variance on differences between right and left cell number demonstrated a significant effect (F = 16.165; df = 2, 7; p < 0.005), and pairwise post hoc tests showed that the embryos with prolonged QT intervals were significantly different from controls and from experimental embryos with normal QT intervals (Newman-Keuls test; p < 0.05). Experimental embryos with normal QT intervals did not differ from control embryos on this measure.
Neuron number and profile area were also studied in the left nodose ganglia of the three experimental embryos which completely lacked right nodose ganglia and had prolonged QT intervals. Mean profile area (373 ± 113μm2) and number (3132 ± 103) in these ganglia were very similar to the values found in the nodose ganglia of the experimental embryos with normal QT intervals. There was thus no evidence that absence of the ganglion on the right side was accompanied by a compensatory enlargement of or increase in the number of neurons in the left ganglion.
In the course of our ECG recordings, we identified one sham-operated embryo with a prolonged QT interval (QTc = 0.338 ms) which we subsequently analyzed morphometrically. The right nodose ganglion volume was considerably smaller than left (0.125 mm3 versus 0.176 mm3), and both were in the range of the experimental embryos rather than the sham group(Table 2). The mean ganglion cell diameter was 361 and 379 μm2 for right and left ganglia, respectively, again falling very close to the mean of the NormQT-RTNP experimental group. Most significantly, the estimated number of ganglion cells in the right nodose ganglion of this embryo (ni = 2760) was considerably less than that in the left nodose ganglion (ni = 3674). Thus, in this case of spontaneously occurring prolonged QT interval, the embryo demonstrated a pattern of imbalance in the number of right and left nodose ganglion neurons that was very similar to the pattern seen in embryos with prolonged QT intervals produced by experimental manipulation.
DISCUSSION
The results of this study indicate that reduction in the number of neurons present in the right nodose ganglion relative to the number in the left ganglion is associated with prolonged QT intervals in the ECG of chick embryos. Presumably, removing the normal precursors of nodose ganglion neurons by ablating the placode produces this relative decrease in the number of neurons present in the ganglion on the lesioned side. The lesion is timed such that the precursor cells are removed before they migrate from the placode and coalesce in the region where the ganglion would normally form. Nonetheless, we have found in previous studies(31) that in many embryos the ablation does not prohibit development of the nodose ganglion: the majority of embryos surviving to d 12 have both right and left ganglia. It is therefore not surprising that the great majority of experimental embryos in this study also had developed right nodose ganglia. Three embryos in which no right ganglion was present did survive to d 17, and perhaps represent the extreme case of right-left imbalance in nodose ganglion cell number. All three embryos had prolonged QT intervals. These data support the hypothesis that a unilateral disruption in the development of sensory innervation of the heart can result in the abnormal cardiac physiology characteristic of long QT syndrome.
Our results also suggest that an overall reduction in the total number of ganglion cells, right plus left, innervating the heart is not in itself the critical factor in producing the prolonged QT interval. The experimental embryos, with prolonged QT intervals and which had right nodose ganglia, had more total nodose ganglion neurons than the experimental group with normal QT intervals (2689 + 4099 = 6788 versus 2810 + 3143 = 5953;Table 3). Thus, the NormQT-RTNP group in one sense provides a control for possible nutritional or other general consequences of disrupting visceral sensory innervation which could impact on cardiac function. All of the experimental groups had reduced ganglion cell numbers compared with the sham control group, however, and it remains a possibility that an overall reduction in total visceral sensory innervation may be a required precondition for development of the cardiac abnormality.
As a further test of the relationship of the right-left imbalance in ganglion cell number with prolongation of the QT interval, it would be useful to examine embryos with bilateral nodose placode ablations, as well as those with unilateral left placode ablations. Unfortunately, this has not been possible. The failure of embryos to survive the left nodose placode ablation remains an enigma. One could speculate that disruption of sensory innervation mediated via the left nodose ganglion may have a more profound effect on the heart and/or other viscera than a similar disruption on the right side, although why this might be the case is not immediately obvious. It has been suggested previously, in relation to the sympathetic innervation(27), that there is an asymmetry in neural regulation of the mammalian heart. Information is lacking for the chick, however, and we would need to know more about the processes occurring at earlier ages and the direct causes of embryo death after these lesions, to fully understand this result. The greater lethality of the bilateral ablation relative to the unilateral right placode ablation is more intuitively comprehensible, as a more extensive disruption of innervation to the heart and viscera would certainly be expected to result from this ablation.
It is also apparent from our results that there are bilateral nonspecific effects resulting from the unilateral ablation. There is a bilateral reduction in the average size of ganglion neurons, in both groups which had the placode removed, irrespective of QT interval. Alteration in the size of ganglion cells as a result of the ablation is therefore not directly related to the cardiac abnormality underlying QT prolongation. It remains possible, however, that it may be a necessary precondition for development of the dysfunction.
The absence of right-left differences in ganglion cell size was somewhat unexpected; in a previous study(31) we found that right nodose ganglion neurons were smaller than left at embryonic d 12 in embryos who had had right nodose placode lesions. We found that, although the left ganglion contained only placode-derived neurons, the ganglion cell population of the right ganglion also included neurons that were derived from neural crest cells, which typically are smaller in diameter than placode-derived neurons early in development(46). This size difference disappears later(46). Although the exact timing of this“catching up” process is not known, it could account for the absence of differences seen at d 12 in left and right cell sizes by embryonic d 17.
Ganglion volume also may be affected in a nonspecific manner by right nodose placode ablation. Although mean volume was lower bilaterally in both experimental groups compared with the control group, analysis of variance did not show a significant effect. Measurement of overall ganglion volume reflects not only decreases in cell number and size, but would also include decreases in other structural elements, such as connective tissue, supporting cells, and axons of the vagus nerve. These elements were not specifically measured in this study. However, they would most likely not be as directly affected by placode ablation as the neuronal population of the ganglion. Thus the ganglion volume measure is probably less sensitive than the other measures used, and its lack of a significant relationship to these other measures is perhaps not surprising.
The association of prolonged QT intervals in the ECG with a disruption in the normal sensory innervation to the heart suggests that the nervous system may play an important role in the genesis of underlying causes of the LQT syndrome. Interfering with the normal development of the nerves innervating the heart, as we have done by removal of the right nodose placode, could have several effects. Reducing the number of right nodose ganglion cells, thus reducing the number of vagal sensory nerves innervating the heart, could potentially disrupt the sensory feedback information available to the CNS for regulating cardiac function and/or induce an asymmetry in what is normally a bilaterally balanced control circuitry. Furthermore, removal of the nodose placode before the differentiation of CNS circuits might also interfere with the normal development of central neural circuits themselves. Little is known about the developmental time course of central control of cardiac function in the chick, and what is known in mammals suggests that this process is too species-specific to generate a relative time table from mammalian data that would be applicable to the chick(47). At the heart, parasympathetic transmission is functional at d 12, and sympathetic at d 16, in the chick embryo(32–34). The brain stem circuitry for autonomic control undoubtedly is developing throughout this time, and perhaps continues for some time after peripheral function is established. Thus, although the heart and cardiovascular system respond to circulating adrenaline and noradrenaline well before (i.e. embryonic d 5) neural transmission is established, these responses change during development and the adult pattern of response to these substances is not evident until considerably posthatching(48). The roles played by central versus peripheral mechanisms in the maturation of these responses remain unknown. Further studies will be necessary to determine the impact of placode ablation on central control circuits in these animals.
On the other hand, the primary effects of disrupting the development of the sensory component of cardiac innervation may be on the other peripheral components of cardiac innervation, rather than in the CNS. It has been shown that alteration in one component of cardiac innervation during development will induce compensatory changes in the other neural components. For example, Kirby et al.(49) have reported that decreasing the sympathetic innervation of the chick heart by removing their precursor cells in the cardiac sympathetic neural crest resulted not only in a decrease in the sympathetic innervation to the heart but also in a compensatory increase in the parasympathetic innervation. It seems likely that compensatory changes in the sympathetic and parasympathetic components of cardiac innervation might also be altered by disruption of the normal pattern of sensory innervation. If this is so, then our finding that disrupting sensory innervation results in a cardiac anomaly characteristic of the long QT syndrome may be easily reconciled with other experimental(19) and clinical(27) findings that support an important role for abnormalities of the sympathetic cardiac innervation in the etiology of long QT syndrome. We are presently assessing both the sympathetic and parasympathetic innervation of the heart to determine whether there are changes in the motor innervation of the heart in chick embryos with nodose placode ablation-induced prolonged QT intervals.
Whichever of these proves to be the major consequence of disrupting nodose ganglion development and the normal pattern of its sensory connections with the heart and the CNS, the central question concerning the mechanism which links these neural consequences to prolongation of the QT interval will remain to be answered. Analysis of the temporal relationship between the development of neural abnormalities and the development of the cardiac dysfunction, would provide a major step toward identifying the critical interaction in this link. The chick embryo model of long QT syndrome provides an excellent opportunity to carry out such an analysis, and to bring to light mechanisms which may be relevant to underlying causes of long QT syndrome in humans.
Abbreviations
- QTc:
-
heart rate-corrected QT interval
References
Franz MR, Bargheer K, Refflenbeul W, Haverich A, Lichtlen PR 1987 Monophasic action potential mapping in human subjects with normal electrograms: direct evidence for the genesis of the T wave. Circulation 75: 379–386
Han J, Millet D, Chizzinitti B, Moe G 1966 Temporal dispersion of recovery of excitability in atrium and ventricle as a function of heart rate. Am Heart J 71: 481–487
Ben-David J, Gerbig NR, Zipes DP 1988 Differential response of early afterdepolarizations and ventricular tachycardia during right and left stellate stimulation in the dog treated with cesium. J Am Coll Cardiol 11: 254A
Bonatti V, Rolli A, Botti G 1983 Recording of monophaisc action potentials of the right ventricle in long QT syndromes complicated by severe ventricular arrhythmias. Eur Heart J 4: 168–179
Jackman WM, Friday KJ, Anderson JL, Aliot EM, Clark M, Lazzara R 1988 The long QT syndromes: a critical review, new clinical observations and a unifying hypothesis. Prog Cardiovasc Dis 31: 115–172
Levine JW, Spear JF, Guanieri T, Weisfeldt ML, de Langen CDJ, Becker LC, Moore EN 1985 Cesium chloride-induced long QT syndrome: demonstration of after-depolarizations and triggered activity in vivo. Circulation 72: 1092–1103
Schechter E, Freeman C, Lazzara R 1984 After-depolarizations as a mechanism for the long QT syndrome: electrophysiological studies of a case. J Am Coll Cardiol 3: 1556–1561
Hashiba K, Moss AJ, Schwartz PJ (Eds) 1992 QT Prolongation and Ventricular Arrhythmias. New York Academy of Science, New York, NY
Schwartz PJ, Malliani A 1975 Electrical alternation of the T wave: clinical and experimental evidence of its relationship with the sympathetic nervous system and with the long QT syndrome. Am Heart J 89: 45–50
Schwartz PJ, Locati E 1985 The idiopathic long QT syndrome: pathogenic mechanisms and therapy. Eur Heart J 6( suppl D): 103–114
Roy PR, Emanuel R, Ismail A, el Tayib MH 1976 Hereditary prolongation of the QT interval. Am J Cardiol 37: 237–243
Schwartz PJ 1985 Idiopathic long QT syndrome: progress and questions. Am Heart J 109: 399–411
Moss AJ, McDonald J 1971 Unilateral cervicothoracic sympathetic ganglionectomy for the treatment of long QT interval syndrome. N Engl J Med 258: 903–904
Moss AJ, Schwartz PJ, Crampton RS, Locati E, Carleen E 1985 The long QT syndrome: a prospective international study. Circulation 71: 17–21
Bhandari AK, Scheinmann MM, Morady F, Svinarich J, Mason J, Winkle R 1984 Effect of left cardiac sympathectomy in the treatment of patients with the long QT syndrome. Circulation 70: 1018–1023
Packer DL, Coltori F, Smith MS, Bardy GH, Benson DW, Edwards SB, German LD 1984 Sudden death after left stellectomy in the long QT syndrome. Am J Cardiol 54: 1365–1366
Till JA, Shinebourne EA, Pepper J, Camm AJ 1988 Complete denervation of the heart in a child with congenital long QT and deafness. Am J Cardiol 62: 1319–1321
Calkins H, Allman K, Bolling S, Kirsch M, Wieland D, Morady F, Schwaiger M 1993 Correlation between scintigraphic evidence of regional sympathetic neuronal dysfunction and ventricular refractoriness in the human heart. Circulation 88: 172–179
Malfatto G, Steinberg SF, Rosen TS, Danilo P Jr, Rosen MR 1992 Experimental QT interval prolongation. Ann NY Acad Sci 644: 74–83
Schwartz PJ 1988 Denervation of the heart in congenital long QT and deafness. Am J Cardiol 64: 424
Schwartz PJ, Locati E, Priori SG, Zaza A 1990 The idiopathic long QT syndrome. In: Zipes DP, Jalife J (eds) Cardiac Electrophysiology. From Cell to Bedside. WB Saunders, Philadelphia, pp 589–605
Ward DD, Camm AJ 1988 QT interval syndromes. Lancet 2: 47
Manoach M, Rein A, Hecht A, Varon D 1992 A cellular basis for the prolonged QT interval in mammals. Ann NY Acad Sci 644: 84–92
Curran ME, Splawski I, Timothy KW, Vincent GM, Green ED, Keating MT 1995 A molecular basis for cardiac arrhythmia: HERG mutations cause long QT syndrome. Cell 80: 795–804
Wang Q, Shen J, Splawski I, Atkinson D, Li Z, Robinson JL, Moss AJ, Towbin JA, Keating ML 1995 SCN5A mutations associated with an inherited cardiac arrhythmia, long QT syndrome. Cell 80: 805–811
Algra A, Tijssen JGP, Roelandt JRTC, Pool J, Lubsen J 1993 Heart rate variability from 24-hour electrocardiography and the 20 year risk for sudden death. Circulation 88: 180–185
Schwartz PJ, Bonazzi O, Locati E, Napolitano C, Sala S 1992 Pathogenesis and therapy of the idiopathic long QT syndrome. Ann NY Acad Sci 644: 112–141
Christiansen JL, Stadt HA, Mulroy MJ, Kirby ML 1989 Electrocardiographic QT prolongation after ablation of the nodose placode in the chick embryo: a developmental model of the idiopathic long QT syndrome. Pediatr Res 26: 11–15
Mulroy MJ, Hotelling HB, Harrison TA 1990 Long QT and long QT with deafness syndrome: Beginning a neural analysis in an embryonic chick model. Ann NY Acad Sci 588: 430–432
d'Amico-Martel A, Noden DM 1983 Contributions of placodal and neural crest cells to avian cranial peripheral ganglia. Am J Anat 166: 445–468
Harrison TA, Stadt HA, Kumiski D, Kirby ML 1995 Compensatory responses and development of the nodose ganglion following ablation of placodal precursors in the embryonic chick (Gallus domesticus). Cell Tissue Res 281: 379–385
Kirby ML, Stewart DE 1986 Development of the ANS innervation to the avian heart. In: Gootman P (ed) Developmental Neurobiology of the Autonomic Nervous System. Humana Press, Clifton, NJ, pp 135–158
Higgins D, Pappano AJ 1981 Development of transmitter secretory mechanisms by adrenergic neurons in the embryonic chick heart ventricle. Dev Biol 87: 148–162
Pappano AJ 1977 Ontogenetic development of autonomic neuroeffector transmission and transmitter reactivity in embryonic and fetal hearts. Pharmacol Rev 29: 3–33
Kirby ML, McKenzie JW, Weidman TA 1980 Developing innervation of the chick heart: A histofluorescence and light microscopic study of sympathetic innervation. Anat Rec 196: 333–340
Kuratani S, Tanaka S 1990 Peripheral development of the avian vagus nerve with special reference to the morphological innervation of the heart and lung. Anat Embryol 182: 435–445
Narayanan CH 1970 Apparatus and current techniques in the preparation of avian embryos for microsurgery and for observing embryonic behavior. Bioscience 20: 868–871
Mulroy MJ, Harrison TA 1994 Developmental study of the long QT with deafness syndrome in the chick embryo: Cochlear pathology. Int J Pediatr Otorhinolaryngol 29: 179–194
Kirby ML, Turnage KL, Hays BM 1985 Characterization of conotruncal malformation following ablation of “cardiac” neural crest. Anat Rec 213: 87–93
Besson WT, Kirby ML, Van Mierop LHS, Teabeaut JR 1986 Effects of the size of lesions of the cardiac neural crest at various embryonic ages on incidence and type of cardiac defects. Circulation 73: 360–364
Nishibatake M, Kirby ML, Van Mierop LHS 1987 Pathogenesis of persistent truncus arteriosus and dextroposed aorta in the chick embryo after neural crest ablation. Circulation 75: 255–264
Bazett HC 1920 An analysis of the time-relations of electrocardiograms. Heart 7: 353–370
Konigsmark B 1970 Methods for the counting of neurons. In: Nauta WJH, Ebbesson SOE (eds) Contemporary Research Methods in Neuroanatomy. Springer-Verlag, New York, pp 315–349
Kirby ML 1988 Nodose placode contributes autonomic neurons to the heart in the absence of cardiac neural crest. J Neurosci 8: 1089–1095
Kirby ML 1988 Nodose placode provides ectomesenchyme to the developing chick heart in the absence of cardiac neural crest. Cell Tissue Res 252: 17–22
d'Amico-Martel A 1982 Temporal patterns of neurogenesis in avian cranial sensory and autonomic ganglia. Am J Anat 163: 351–372
Gootman PM 1991 Developmental aspects of reflex control of the circulation. In: Zucker IH, Gilmore JP (eds) Reflex Control of the Circulation. CRC Press, Boca Raton, FL, pp 965–1053
Girard H 1973 Adrenergic sensitivity of circulation in the chick embryo. Am J Physiol 224: 461–469
Kirby ML, Conrad DC, Stewart DE 1987 Increase in the cholinergic plexus in sympathetically aneural chick hearts. Cell Tissue Res 247: 489–496
Kirby ML, Stewart DE 1983 Neural crest origin of cardiac ganglion cells in the chick embryo: identification and extirpation. Dev Biol 97: 433–443
Baumel JJ 1975 Aves nervous system. In: Getty R (ed) Anatomy of the Domestic Animals. WB Saunders, Philadelphia, pp 2019–2062
Tummons J, Sturkie PD 1968 Cardioaccelerator nerve stimulation in chickens. Life Sci 7: 377–380
Tummons J, Sturkie PD 1969 Nervous control of heart rate during excitement in the adult White Leghorn cock. Am J Physiol 216: 1437–1440
LeDouarin NM, Teillet MA, Fontaine-Perus J 1984 Chimeras in the study of the peripheral nervous system of birds. In: LeDouarin NM, McLaren A (eds) Chimeras in Develpmental Biology. Academic Press, New York, pp 318–352
LeDouarin NM, Teillet MA 1974 Experimental analysis of the migration and differentiation of neuroblasts of the autonomic nervous system and of neuroectodermal mesenchymal derivatives, using a biological cell marking technique. Dev Biol 41: 162–184
Cabot JB, Cohen DH 1977 Avian sympathetic cardiac fibers and their cells of origin: anatomical and electrophysiological characteristics. Brain Res 131: 73–87
Cabot JB, Cohen DH 1977b Anatomical and physiological characterization of avian sympathetic cardiac afferents. Brain Res 131: 89–101
Fedde MR, Burger RE, Kitchell RL 1963 Localization of vagal afferents involved in the maintenance of normal avian respiration. Poult Sci 42: 1224–1236
Higgins D, Pappano AJ 1979 A histochemical study of the ontogeny of catecholamine-containing axons in the chick embryo heart. J Mol Cell Cardiol 11: 661–668
Cabot JB, Cohen DH 1980 Neural control of the avian heart. In: Bourne GH (ed) Hearts and Heart-Like Organs. Academic Press, Orlando, FL, pp 190–258
Macdonald RL, Cohen DH 1970 Cells of origin of sympathetic pre- and postganglionic cardioacceleratory fibers in the pigeon. J Comp Neurol 140: 343–358
Acknowledgements
The authors thank Dr. M. L. Kirby and the Heart Development Group at the Medical College of Georgia for performing the nodose placode lesions, J. G. Hunter and H. B. Hotelling for technical assistance, and K. Waldo for graphic arts.
Author information
Authors and Affiliations
Additional information
Supported by National Institutes of Health Grant HL 36059.
Rights and permissions
About this article
Cite this article
Harrison, T., Mulroy, M. Abnormal Cardiac Sensory Innervation Associated with Experimentally Induced, Electrocardiographic Long QT Intervals in Chick Embryos. Pediatr Res 39, 90–97 (1996). https://doi.org/10.1203/00006450-199601000-00013
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199601000-00013
