
Abstract
The aim of this study was to determine the neuropsychologic development in patients with congenital (primary) hypothyroidism (CH) detected by screening and treated from early age. Seven studies were evaluated, including 675 CH patients and 570 controls. Criteria for inclusion of the studies were:1) age of patients and controls ≥5 y; 2) control group well defined in the original article. A meta-analysis of the data on the intellectual development was performed. All analyzed studies show a trend toward lower intelligence quotient (IQ) and-as far as investigated-poorer motor skills in CH patients compared with controls. Pooling of data showed a significant deficit of the mean IQ of 6.3 (95% confidence interval: 4.7-7.8). The most important independent risk factor for the eventual outcome appears to be the severity of CH (defined by initial thyroxine at the moment of diagnosis and by skeletal maturation); treatment variables do not seem to have an important effect the cognitive development. We conclude that CH, despite early detection and treatment, results in an IQ deficit; the severity of CH seems to be the most important individual risk factor. Our second conclusion is that, although biomedical risk factors are well investigated, the individual weight of these factors is yet largely unknown. This may be due to the variability of definitions and test tools, especially for the investigation of motor skills, that have been used.
Similar content being viewed by others

Main
CH is a frequent disorder, leading to retardation of mental development and growth if not treated early. In the 1970s, neonatal mass screening programs were started all over the world to guarantee detection and treatment from the 1st wk of life. There is ample evidence that the long-term prognosis has improved since screening was introduced. The growth of early treated patients is essentially normal(1, 2) and mental development has much improved(3–6). However, only a few studies were published in which CH patients were compared with well defined control groups on mental as well as other aspects of neuropsychologic development. To avoid investigator bias and bias caused by the upward secular drift in IQ, cognitive development in CH patients cannot be investigated by comparing the IQ with reference data in the general population. In addition, it appears that in the assessment of neuropsychologic development of CH patients, apart from the evaluation of cognitive function, evaluation of motor skills is extremely important. Many different tools are used for the evaluation of motor development. Therefore, for both aspects of development, evaluation of case-control studies is necessary.
We report an analysis of literature data, to determine: 1) the intellectual development, motor skills, and behavior of early treated CH patients compared with those of controls and 2) which biomedical risk factors for retardation can be defined in these patients.
METHODS
A literature search was performed using MEDLINE data from 1988 up to September 1994 inclusively. Studies which fulfilled the following criteria were included: 1) age of patients and controls ≥5 y and2) control group well defined in the original article. If several studies on the same cohort at different ages were published, the study on the oldest children was included. An exception was made for those studies which described different aspects of development in the different age groups. Comparative studies between CH patients and a reference population not investigated by the authors of the original article, were excluded.
Details of the tests used for the assessment of motor and cognitive functions and of the statistical methods used in the different studies can be found in the original papers.
The following data were collected: number of cases and controls, matching variables, age (distribution), response rate, mean age of treatment, biomedical risk factors (etiology of CH, pretreatment T4, skeletal maturation, T4 dosage); IQ, motor skills, and behavior. Data on full scale, verbal, and performance IQ were pooled, and a weighted mean difference(IQ deficit of patients versus controls) was calculated. If the SD of the IQ distribution was not stated in the original paper, a value of 15 was assumed. Data on the risk factors and on the motor skills and behavior could not be pooled, because of the many different definitions and investigation tools used; therefore, only descriptive comparisons were made.
RESULTS
Studies Included
Seven studies (675 CH patients and 570 controls) fulfilled the inclusion criteria(3, 7–14). The study characteristics are summarized in Table 1. The studies are named after the screening area. The patient group described in the North Thames study is also part of the UK study.
Cognitive Functions
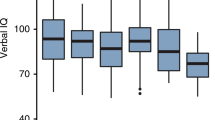
Table 2 summarizes the overall data on intellectual functions. In all studies the IQ, the global IQ as well as the verbal and performance IQ, is lower in the CH group than in the control group (deficit of the mean full scale IQ 4-11.8), although the difference does not reach significance in all studies. Meta-analysis of the pooled data showed a significant deficit of the IQ of patients compared with controls (full scale, 6.3; verbal, 6.4; performance, 6.1).
Motor Skills
Motor skills are reported in four of the seven studies; none of the groups used the same study tool. Motor functioning of CH patients differed significantly from the control group in all studies (Table 3). Motor impairment seemed to be more pronounced in balance and fine motor function than in gross motor function.
Behavior
The Norwegian study evaluated behavior by the Richmann behavior checklist. No statistically significant differences were found between CH patients and controls. The Achenbach Child Behavior Checklist was used in the New England study. This study, too, could not detect significant differences.
Biomedical Risk Factors for Disturbance in Cognitive Function(Table 4)
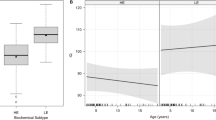
Initial low T4. Four studies found a significant correlation between the IQ and the pretreatment T4. However, the UK study found that this relation was discontinuous with a threshold at 42.8 nmol/L.
Skeletal maturation. The Toronto study compared the intrauterine hypothyroid group (defined as a skeletal development at time of diagnosis ≤36 wk of gestation) with the postnatal hypothyroid group; the intrauterine hypothyroid group had a significantly lower IQ. The Quebec study(at the age of 5 y) shows a significantly lower IQ in those CH patients with an area-of-the-knee epiphysis <0.05 cm2 compared with a control group.
Etiology. Four studies assigned CH patients to subgroups defined by etiology (agenesis, dyshormonogenesis and hypoplasia/ectopia). The Toronto study and the Dutch study compared these subgroups with the control group. Both studies found in the agenesis group a significantly lower IQ. The Quebec study found at the age of 5 y no significant difference between the CH subgroups. The Norwegian study found a significantly lower performance IQ in the agenesis group compared with the ectopic group.
Initial T4 and skeletal maturation. The Quebec study (at the age of 12 y) defined a subgroup with a severe form of CH based on initial T4 and skeletal maturation. Patients with a severe form of CH had a significantly lower IQ than the control group.
Age at start of treatment. In the North Thames study, IQ tended to be lower in the group treated after the age of 30 d in comparison to the group treated from earlier age. Neither the UK study nor the Dutch study found a significant correlation between IQ and age at start of treatment.
T4 dose. In the UK study, no correlation between T4 dose and IQ could be demonstrated. The Norwegian study showed a significant correlation between T4 dose at the age at 1 y and the verbal IQ at the age of 6.
Multivariate analyses. The Toronto study investigated the percentage of variance accounted for by the following variables: age, sex, parental IQ, social status, etiology, bone age, treatment age and age of normalization of T4. The overall p level was <0.05 for all fields of development (language, visuomotor, motor, memory, spatial ability, and auditory discrimination). Parental IQ, bone age, and treatment age accounted for a significant proportion of the variance in language.
The UK study could not detect a relationship between IQ and age at start of treatment, T4 dose, and plasma T4 during the first year of life. The North Thames study (at the age of 5 y) investigated in a multivariate model the independent contribution of initial T4, age at start of treatment and social class to IQ. T4 and social class were independently and significantly associated with IQ.
The Norwegian study assigned CH patient to subgroups defined by mean T4 level in the age group of the 1st y, 1-2 y, 2-4 y, and 4-6 y. The T4 during the 1st y as well as during the age period of 1-2 y was significantly correlated with the 6 y verbal IQ in an analysis of covariance(with sex, social class and initial T4 as covariates). The low T4 group (<129 nmol/L) had a lower verbal IQ. No other significant correlations were found.
Biomedical Risk Factors for Disturbance in Motor Skills
Initial low T4. The Dutch study compared subgroups assigned by initial T4 with the control group; the initial low T4 group performed significantly more poorly. The North Thames study(at the age of 5 y) found a trend toward better motor skills with higher initial T4.
Skeletal maturation. In the Toronto study children in the intrauterine hypothyroid group (definition see above) had significantly poorer motor skills than the postnatal group.
Etiology. The Toronto study showed that the athyroid group rated significantly more poorly, compared with the other etiology groups. The Dutch study compared the three etiology groups with the motor skills of the control group. The agenesis group scored significantly more poorly.
Age at start of treatment. The Dutch study found no significant correlation between motor skills and age at start of treatment. In the North Thames study, the motor skills tended to be lower in the group treated after the age of 30 d.
Multivariate analyses. The Toronto study investigated the percentage of variance accounted for by the following variables: age, sex, parental IQ, social status, etiology, bone age, treatment age and age of normalization of T4. Etiology and bone age accounted for a significant proportion of the variance in motor skills.
The North Thames study investigated in a multivariate model the independent contribution to motor skills of initial T4, age at start of treatment and social class. Only initial T4 was independently and significantly associated with the eventual motor skills.
DISCUSSION
Each year millions of neonates all over the world are screened for congenital hypothyroidism. Early detection and treatment have much improved the prognosis for these children, although individual risk factors may lead to a low IQ and poorer motor skills.
We report an analysis of literature data of seven studies in which CH patients (n = 675) are compared with well defined concurrent control groups (n = 570) investigated by the authors. We excluded other studies for two reasons. 1) Cases as well as controls have been studied by the same investigator, thus avoiding bias. 2) Use of population data as reference may lead to bias as a result of the upward secular shift in the outcome of IQ tests. We have chosen for the most recent published studies, to evaluate a follow up as long as possible. During long term follow up, various aspects of development can improve(11, 15), although noncompliance can influence the results(16).
All studies we analyzed show a trend toward lower IQ and-as far as studied by the authors-poorer motor skills in CH patients compared with controls; meta-analysis showed the deficit to be significant. The most important independent risk factor for the eventual outcome is the severity of CH(defined by initial T4 at the moment of diagnosis and skeletal maturation). Several studies which did not fulfill our inclusion criteria found similar risk factors(17–20). Treatment variables such as age at start of treatment, T4 dose and plasma T4 during treatment do not seem to be an important additional risk factor for the eventual cognitive development in CH found in neonatal screening. The optimal dose of T4 was discussed by various authors(10, 21–23); from the so far published data as well as from the studies analyzed in this article(8, 9) no conclusive information is available. This aspects remains subject for further study.
The results suggest that at least part of the brain damage in patients with CH is caused in utero and cannot be prevented by early treatment. Tillotson et al.(8) estimate that without a screening program 40% of patients with severe hypothyroidism will show impairment of a degree likely to require special education, whereas in early treated CH this percentage is 10.
To assess the amount of prenatal damage to the brain, one would need to have insight in the fetal T4 level. Fetal T4 level is dependent on the production of T4 by the fetus itself as well as on the amount of maternal T4 transferred to the fetus. At approximately 14 d after birth, all maternal T4 transferred has been used by the fetus(21). After that time, the measured T4 will have been produced by the infant itself. Therefore, T4 at diagnosis, which usually takes place after 14 d of age, will be a good indicator of fetal production.
At present there is no good indicator for the amount of maternal T4 that is being transferred to the fetus. It is likely that this amount may vary greatly, because in patients with severe CH it has been shown that cord serum concentrations range from 35 to 70 nmol/L(24). Skeletal maturation is greatly dependent on T4 levels and can therefore be seen as a combined measure of fetal T4 production and maternal T4 transferred to the fetus. The results of Glorieux et al.(3, 14) suggest that a combination of diagnostic T4 and skeletal maturation may be the best predictor, currently available, for later development.
Two study groups designed a predictive model based on individual risk factors. Glorieux et al.(25) predicted in 10 out of 13 patients correctly an IQ < 90 in severe CH, defined as a low initial T4, and retardation of skeletal development (seeTable 4). According to a prediction based on the logistic model of the UK study(8), children with an initial T4 > 47 nmol/L are unlikely to suffer impairment of more the five IQ points. A meta-analysis of data derived from the various studies could probably be the basis for a further refinement of such predictive models for a poor outcome in the individual patient. However, the variability of the definitions used (initial T4, skeletal maturation, treatment parameters) and the diversity of tests for evaluation of the motor development makes such an analysis impossible at this moment.
We conclude that CH, despite early detection and treatment, results in a significant IQ deficit of approximately 6 points. The severity of CH(agenesis, low initial T4, retardation of skeletal malformation), rather than treatment variables, appear to be the most important individual risk factor. Although several biomedical risk factors have been well investigated in many studies, the individual weight is not precisely known. New recommendations of the American Academy of Pediatrics, the American Thyroid Association, and the European Society for Pediatric Endocrinology should help future investigators to design their follow up study in such a way that studies can be compared with each other.
Abbreviations
- CH:
-
congenital hypothyroidism
- CI:
-
confidence interval
- IQ:
-
intelligence quotient
- T4:
-
thyroxine
References
Aronson R, Ehrlich RM, Bailey JD, Rovet JF 1990 Growth in children with congenital hypothyroidism detected by neonatal screening. J Pediatr 116: 33–37.
Grant DB 1994 Growth in early treated congenital hypothyroidism. Arch Dis Child 70: 464–468.
Glorieux J, Dussault JH, Morisette J, Desjardins M, Letarte J, Guyda H 1985 Follow-up at ages 5 and 7 years on mental development with hypothyroidism detected by Quebec Screening Program. J Pediatr 107: 913–915.
New England Congenital Hypothyroidism Collaborative 1985 Neonatal hypothyroidism screening: status of patients at 6 years of age. J Pediatr 107: 915–919.
Illig R, Largo RH, Qin Q, Torresani T, Rochiccioli R, Larsson A 1987 Mental development in congenital hypothyroidism after neonatal screening. Arch Dis Child 62: 1050–1055.
Rovet JF, Ehrlich RM, Sorbara DL 1987 Intellectual outcome in children with fetal hypothyroidism. J Pediatr 110: 700–704.
Rovet JF, Ehrlich RM, Sorbara DL 1992 Neurodevelopment in infants and preschool children with congenital hypothyroidism: etiological and treatment factors affecting outcome J Pediatr P. sychol 17: 187–213.
Tillotson SL, Fuggle PW, Smith I, Ades AE, Grant DB 1994 Relation between biochemical severity and intelligence in early treated congenital hypothyroidism: a threshold effect. BMJ 309: 440–445.
Heyerdahl S, Kase BF, Lie SO 1991 Intellectual development in children with congenital hypothyroidism in relation to recommended thyroxine treatment. J Pediatr 118: 850–857.
New England Congenital Hypothyroidism Collaborative 1990 Elementary school performance of children with congenital hypothyroidism. J Pediatr 116: 27–32.
Kooistra L, Laane C, Vulsma T, Schellekens JM, van der Meere JJ, Kalverboer AF 1994 Motor and cognitive development in children with congenital hypothyroidism: a long-term evaluation of the effects of neonatal treatment. J Pediatr 124: 903–909.
Fuggle PW, Grant DB, Smith I, Murphy G 1991 Intelligence, motor skills and behavior at 5 years in early-treated congenital hypothyroidism. Eur J Pediatr 150: 570–574.
Simons, WF, PW Fuggle, DB Grant, I Smith 1994 Intellectual development at 10 years in early treated congenital hypothyroidism. Arch Dis Child 71: 232–234.
Glorieux J, Dussault J, Van Vliet G 1992 Intellectual development at age 12 years of children with congenital hypothyroidism diagnosed by neonatal screening. J Pediatr 121: 581–584.
Money J, Clarke FC, Beck J 1978 Congenital hypothyroidism and IQ increase: a quarter century follow-up. J Pediatr 93: 432–434.
New England Congenital Hypothyroidism Collaborative 1994 Correlation of cognitive test scores and adequacy of treatment in adolescents with congenital hypothyroidism. J Pediatr 124: 383–387.
Toublanc JE, Rives S, Acosta A, Chicaud J 1990 Le developpement psychomoteur et intellectuel chez 52 enfants atteints d'hypothyroidie congenitale depistee a la naissance. Elements susceptibles d'influer sur le pronostic. Arch Fr Pediatr 47: 191–195.
Ilicki A, Larsson A 1991 Psychological development at 7 years of age in children with congenital hypothyroidism. Timing and dosage of initial treatment. Acta Paediatr Scand 80: 199–204.
Rochiccioli P, Roge B, Alexandre F, Tauber MT 1992 School achievement in children with hypothyroidism detected at birth and search for predictive factors. Horn Res 38: 236–240.
Gottschalk B, Richman RA, Lewandowski L 1994 Subtle speech and motor deficits of children with congenital hypothyroid treated early. Dev Med Child Neurol 36: 216–220.
Fisher DA, Foley BL 1989 Early treatment of congenital hypothyroidism. Pediatrics 83: 785–789.
Dussault JH 1990 Early treatment of congenital hypothyroidism [Letter]. Pediatrics 85: 237–238.
Fisher DA 1990 Early treatment of congenital hypothyroidism [letter]. Pediatrics 85: 238–239.
Vulsma T, Gons MH, Vijlder de JJde JJM 1989 Maternal-fetal transfer of thyroxine in congenital hypothyroidism due to a total organification defect or thyroid agenesis. N Engl J Med 321: 13–16.
Glorieux J, M Desjardins, J Letarte, J Morisette, JH Dussault 1988 Useful parameters to predict the eventual mental outcome of hypothyroid children. Pediatr Res 24: 6–8.
Author information
Authors and Affiliations
Additional information
Manuscript dedicated to Professor H.K.A. Visser in honor of his retirement.
Rights and permissions
About this article
Cite this article
Derksen-Lubsen, G., Verkerk, P. Neuropsychologic Development in Early Treated Congenital Hypothyroidism: Analysis of Literature Data. Pediatr Res 39, 561–566 (1996). https://doi.org/10.1203/00006450-199603000-00028
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199603000-00028
This article is cited by
-
Simulations of radioiodine exposure and protective thyroid blocking in a new biokinetic model of the mother–fetus unit at different pregnancy ages
Archives of Toxicology (2022)
-
A comparison of thyroidal protection by stable iodine or perchlorate in the case of acute or prolonged radioiodine exposure
Archives of Toxicology (2020)
-
Intelligence Quotient at the Age of Six years of Iranian Children with Congenital Hypothyroidism
Indian Pediatrics (2018)
-
Neurodevelopmental outcome of children with congenital hypothyroidism diagnosed in a national screening program in Turkey
Indian Pediatrics (2017)
-
Health- related quality of life and self-worth in 10-year old children with congenital hypothyroidism diagnosed by neonatal screening
Child and Adolescent Psychiatry and Mental Health (2012)
