
Abstract
Background:
Mechanisms underlying coffee's beneficial actions against cardiovascular disease and glucose metabolism are not well understood. Little information is available regarding association between coffee consumption and adipocytokines.
Objective:
We investigated potential associations between coffee consumption and adiponectin, leptin, markers for subclinical inflammation, glucose metabolism, lipids and liver enzymes. We then investigated whether adipocytokines played a role in the association between coffee consumption and these markers.
Design and subjects:
This is a cross-sectional study comprising 2554 male and 763 female Japanese workers. Potential relations between coffee consumption and adipocytokines or other markers were evaluated using a multiple linear regression model adjusted for confounding factors. We evaluated whether adiponectin and leptin partly explain the associations between coffee consumption and each marker by multiple mediation analysis.
Results:
Coffee consumption showed significant positive associations with adiponectin and total and low-density lipoprotein cholesterol, and inverse associations with leptin, high sensitivity C-reactive protein (hs-CRP), triglycerides and liver enzymes (all P<0.05). An adjustment for adiponectin and leptin significantly attenuated the associations between coffee consumption and hs-CRP or triglycerides, but not for liver enzymes. No associations were observed between coffee consumption and glucose metabolism-related markers.
Conclusion:
Coffee consumption was associated with high adiponectin and low leptin levels. We speculated that adipocytokines mainly explain the associations of coffee consumption with lipids and hs-CRP. Factors other than adipocytokines may explain the association between coffee consumption and liver function.
Similar content being viewed by others
Introduction
Coffee is one of the world's most commonly consumed beverages, and its effects on health have been attracting considerable attention.1, 2, 3 An inverse association of coffee consumption with triglycerides4, 5 and a positive association with high-density lipoprotein cholesterol levels were previously reported.6 Consumption of unfiltered coffee showed greater positive associations with total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) than filtered coffee.6 A meta-analysis of 15 large prospective studies has shown that four or more cups of coffee consumption per day was associated with a significantly lower risk of type 2 diabetes mellitus (DM).3 Although it has been speculated that weight loss,7 attenuation of subclinical inflammation,8 reduction of oxidative stress6 and ameliorating effects on liver function9, 10 might be potential mechanisms underlying the association, the precise mechanisms remain unknown. A few studies that assessed the association of coffee consumption with subclinical inflammation showed inconsistent results: positive11 and negative8 associations. A short-term clinical trial showed that C-reactive protein (CRP) levels did not change after coffee consumption.6
Adiponectin and leptin are well known to have important roles in the lipid and glucose metabolisms as well as inflammatory regulation.12, 13, 14, 15, 16, 17 The association between coffee consumption and adiponectin is still debated. Two cross-sectional studies showed positive association of coffee consumption with adiponectin,18, 19 whereas one study showed that coffee consumption was not significantly associated with adiponectin levels.20 In a clinical trial, adiponectin levels increased after eight cups of coffee per day compared with 0 cups per day.6 Few studies have examined the association of coffee consumption with leptin levels and it remains to be elucidated.21 There is a possibility that coffee consumption is associated with adipocytokines, markers of subclinical inflammation, lipids, glucose metabolism and liver function. Additionally, we hypothesized that these associations might be explained partly by adipocytokines.
In this study, we explored the potential association of coffee consumption with a number of biomarkers, and examined whether adipocytokines might explain these associations.
Materials and methods
Study sample
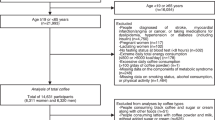
The Aichi Workers' cohort included 6651 civil servants in Aichi Prefecture, an urban and suburban area located in central Japan between 35 and 69 years of age at recruitment in 2002 (participation rate: 62%). Most of the cohorts were engaged in clerical work. Police officers, firefighters and public school teachers were not included. Baseline information was obtained through self-administered questionnaires and mandatory annual health check-ups provided by the worksite. Participants not consenting to the use of health check-up data or who did not provide blood sample were excluded from the present analysis (n=2570). We further excluded those without coffee consumption data (n=52), those with a history of cardiovascular diseases as well as those who had been on medication for hypertension, DM or dyslipidemia (n=732), because the treatment and associated behavioral change could confound the association between coffee consumption and blood markers, leaving 2554 men and 763 women eligible for the present analysis. The study protocol was approved by the Ethics Review Committee of the Nagoya University School of Medicine.
Main exposure variables
Coffee consumption frequency was assessed by a question item in the brief dietary history questionnaire that required recall of dietary habits over 1 month. The possible responses included eight frequency categories: never, less than one cup per week, one cup per week, two to three cups per week, four to six cups per week, one cup per day, two to three cups per day and four or more cups per day. For the descriptive analysis, the lower five categories were incorporated into a separate category of less than one cup per day, because of the small number of the subjects in these categories. In the multiple linear regression analysis, coffee consumption frequency was treated as a continuous variable. For each category of coffee consumption frequency, the following numbers were assigned: 0, 0.05, 0.1, 0.4, 0.7, 1, 2.5 and 4 cups per day, respectively. We also assessed whether they used sugar in their coffee, categorized as used, not used and no answer.
Analysis of blood samples
Blood serum samples were drawn from the subjects overnight or after fasting for at least 8 h, and were stored at −80 °C until biochemical assay. All the assays were carried out at a commercial laboratory using the standard procedures. Adiponectin was determined using an enzyme-linked immunosorbent assay kit (Otsuka Pharmaceutical Co., Ltd, Tokyo, Japan). The detection limit of the adiponectin assay was 0.40 μg ml−1. Leptin was measured by a radioimmunoassay kit (HUMAN LEPTIN RIA KIT, Linco Research, Inc., St Charles, IL, USA). The detection limit of the leptin assay was 0.5 ng ml−1, specificity of the human leptin was 100%.
High sensitivity C-reactive protein (hs-CRP) was measured by latex nephelometry (Siemens Healthcare Diagnostics Inc., Tarrytown, NY, USA), which was sensitive enough to detect 0.02 mg l−1. Tumor necrosis factor-α (TNF-α) was measured by enzyme immunoassay with a minimum detectable level of 6 pg ml−1 (R&D Systems Inc., Minneapolis, MN, USA). High-sensitivity interleukin 6 (IL-6) was also measured by enzyme immunoassay (R&D Systems Inc.).
Fasting blood glucose was enzymatically determined by the hexokinase method (GLU-HK; Shino-test Corp., Tokyo, Japan). Fasting immunoreactive insulin was measured by a solid-phase radioimmunoassay (RIABEAD2; Dinabot Co., Ltd, Chiba, Japan), while a homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as FBS (mg dl−1) × fasting immunoreactive insulin (μU ml−1)/405.
TC and triglycerides were determined enzymatically. High-density lipoprotein cholesterol was measured by the phosphotungstate method. LDL-C was measured by an enzymatic method (Cholestest; Sekisui Medical Co., Ltd, Tokyo, Japan).
Aspartate aminotransaminase, alanine aminotransaminase and gamma-glutamyl transpeptidase were measured by the consensus method of the Japan Society of Clinical Chemistry. Intra-assay coefficients of variation of each variable were as follows: adiponectin, <8.6%; leptin, <1.79%; hs-CRP, <4.0%; TNF-α, <9.6%; IL-6, <7.5%; Aspartate aminotransaminase, <4.9%; alanine aminotransaminase, <7.5%; and gamma-glutamyl transpeptidase, <2.0%. TNF-α and IL-6 were only available for a portion of the studied sample (n=691).
Other variables
Height and weight were measured in a standing position at the annual health check-up, with body mass index (BMI) being calculated as weight in kilograms divided by the square of the height in meters. Smoking status was self-reported, and classified into current, ex- or never smokers. The number of cigarettes smoked per day was also obtained for current and ex-smokers. Physically active subjects were defined as those who engaged in moderate or vigorous exercise for more than 60 min per week.22 Brief dietary history questionnaire was also used to assess other dietary habits. Total energy intake, and the intakes of magnesium and alcohol were calculated using the ad hoc computer algorithm based on the Standard Table of Food Composition in Japan, fifth revised edition.23 Consumption frequency of green tea was assessed using the same categories as coffee consumption. In the present analysis, they were incorporated into two categories: one cup or less per day and two or more cups per day. The estimated glomerular filtration rate (eGFR) was calculated as 194 × serum creatinine−1.094 × Age−0.287 × 0.739 (if female) (ml min−1 per 1.73 m2).24
Statistical analysis
Adipocytokines, inflammatory and glucose metabolism-related markers, lipids, liver enzymes and eGFR were natural logarithmically transformed to approximately normalize the distribution and used in the analysis, then transformed back for data presentation, and shown as geometric means and 95% confidence intervals. A comparison of continuous variables among coffee consumption groups was conducted by one-way analysis of variance or covariance adjusted for covariates described below. The linear trend across coffee consumption categories was evaluated by using the polynomial procedure of SPSS. Multiple linear regression analysis, taking adipocytokines, inflammatory markers, lipids, glucose metabolism-related markers and liver enzymes as dependent variables, was also performed to evaluate the direction and magnitude of associations with coffee consumption. Independent variables included in the model were age, BMI, smoking status, cigarettes smoked per day for current smokers, physical activity, total energy intake, intakes of alcohol, magnesium and green tea, sugar use in coffee, and eGFR.
Then, we performed the multiple mediation analyses based on the structure equation modeling using SPSS macros provided by Preacher and Hayes25 to examine how much of the association between coffee consumption and inflammatory or glucose metabolism-related markers, lipids or liver enzymes was attributable to the adipocytokines. Figure 1 shows the multiple mediation model, with path a(s) representing the relations of coffee consumption (X) to adipocytokines (M(s)), path b(s) representing the relations of M(s) to each marker (Y(s)) adjusted for X, path c(s) representing the relations of X to Y(s) and path c(s) representing the relations of X to Y(s) adjusted for M(s). All of these paths would typically be quantified with regression coefficients calculated by multiple linear regression analyses. The mediation analyses were carried out for variables in which only when all the paths a(s), b(s) and c(s) to be statistically significant,25 that is, Model 1 P-values, and Model 2 P-values for ln-leptin and ln-adiponectin in Table 2 <0.05. In the mediation analysis, the indirect effect of X on Y through M(s) is defined as the product of path a and path b, that is, a1b1 and a2b2. And, the total effect of X on Y is the sum of the direct effect and all of indirect effects: c=c' + a1b1 + a2b2. We computed bootstrapped bias-corrected 95% confidence intervals (5000 samples) for the size of the specific mediation effects. All multiple mediation analyses were performed with adjustments for the covariates used in the multiple regression analysis. We presented standardized regression coefficients (β) and respective 95% confidence intervals so that comparison of the strength of the associations investigated would be possible. All statistical analyses were conducted using the SPSS statistical package for Windows version 19.0 (SPSS Inc., Chicago, IL, USA).

Multiple mediation model with two mediators (M1, ln-adiponectin; M2, ln-leptin) in the context of this study. (1) Total effect of coffee consumption (X) on each marker (Y(s)) – path c. (2) Coffee consumption is hypothesized to exert indirect effects on each marker through ln-adiponectin (M1) and ln-leptin (M2), and to exert a direct effect on each marker (path c'(s)). The specific indirect effect of X on Y through M1 is defined by the product of the two paths linking X on Y through that mediator, that is, a1b1; similarly, the specific indirect effect of X on Y through M2 is defined by a2b2. The total indirect effect of X on Y is the sum of the two specific indirect effects, that is, a1b1 + a2b2. The total effect of X on Y is thus the sum of the direct effect and all of the indirect effects: c = c' + a1b1 + a2b2.
Results
The mean±s.d. age was 47.6±7.1 years, and the mean BMI was 22.8±2.7 kg m−2 (range 15.0–35.8). Current and ex-smokers accounted for 29.6% and 21.1% of the sample, respectively. The geometric means of insulin, adiponectin and leptin were 4.59 μU ml−1, 6.78 μg ml−1 and 6.58 ng ml−1, respectively. Greater coffee consumption was associated with younger age, a higher proportion of current smoking and higher total energy and magnesium intakes (all P<0.001) (Table 1). Coffee consumption was also associated positively with eGFR (P=0.033), but was not related to BMI or physical activity. Coffee consumption was inversely associated with the intakes of green tea (P=0.003).
Coffee consumption was positively and significantly associated with adiponectin levels (Tables 1 and 2) independent of potential confounding variables (P<0.001). In contrast, it was negatively associated with leptin (P<0.001), hs-CRP (P=0.026), triglycerides (P=0.026) and liver enzymes (all P<0.001). The inverse association of coffee consumption with hs-CRP or triglycerides was attenuated by additional adjustment for adipocytokines and became statistically insignificant, that is, completely explained. Although the associations of coffee consumption with liver enzymes were also attenuated by adipocytokines, they were nevertheless significant. Coffee consumption was positively associated with TC and LDL-C; interestingly, these associations were strengthened by the inclusion of adipocytokines in the model. Statistically significant associations were not observed between coffee consumption and high-density lipoprotein cholesterol or glucose metabolism-related markers.
The mediation effects by adiponectin and/or leptin on the association of coffee consumption were evaluated for hs-CRP, triglycerides or liver enzymes (Table 3). Adipocytokines explained 43.1% and 61.2% of the associations of coffee consumption with hs-CRP and triglycerides, respectively. Total mediation effects by adipocytokines on the associations of coffee consumption with liver enzymes ranged from 19% for aspartate aminotransaminase to 33.3% for alanine aminotransaminase.
Discussion
In the present study, we found that the amount of coffee consumption was associated positively with adiponectin and inversely with leptin levels. Although coffee consumption was not related to BMI, our finding was independent of BMI and potential confounding variables. These associations of coffee with adipocytokines explained most of its association with triglycerides and some of those with hs-CRP and liver enzymes. A positive association of coffee consumption with adiponectin levels is consistent with previous reports from smaller studies.18, 19 As adiponectin is secreted from adipocytes,12 coffee may have effects on adipocytes. Indeed, one of the major substances that coffee contains among several hundred other substances, caffeine, in an experimental study led to the upregulation of peroxisome proliferator-activated receptor γ expression,26 which is an essential regulator of adipocyte differentiation and maintenance.27 As no association between decaffeinated coffee consumption and adiponectin was reported,19 caffeine contained in the coffee may have acted to increase adiponectin levels.
We observed a statistically significant inverse association between coffee consumption and leptin concentration in the present study. This was consistent with a previous study that found a statistically insignificant inverse association.21 Although the pathophysiological significance of blood leptin levels is not fully understood, it is positively correlated with obesity and inflammatory markers.28 In addition, increased circulating leptin has been implicated as a marker of leptin resistance.29, 30 As increased leptin levels may have effects on tissues and organs that remain sensitive to high leptin concentrations,31 the decrease of leptin due to coffee consumption may attenuate such effects. However, it remains to be elucidated how coffee consumption might do so.
The level of hs-CRP is a marker of systemic low-grade inflammation. An inverse association of coffee consumption with hs-CRP was mainly explained by adiponectin and leptin, a finding consistent with previous studies reporting the role of leptin and adiponectin-determining serum CRP levels.32, 33 Our data also showed that mediation effects of adiponectin and leptin on hs-CRP were almost equal.
Coffee consumption was inversely associated with triglycerides, also consistent with previous reports.4, 5, 6 However, in this study we were the first to reveal that the association was explained mainly by adiponectin. Coffee may have a potential to improve hypertriglyceridemia through its effects on adiponectin. In contrast, LDL-C and TC were positively associated with coffee consumption. That finding is also consistent with others even though consumption of unfiltered coffee would be very little in the present sample.6, 34 Our data showed that adipocytokines negatively mediated the associations of coffee consumption with TC and LDL-C. In other words, adipocytokines were suggested to have suppressed35 coffee's cholesterol-increasing effect.36
In line with previous studies,9, 10 coffee consumption was inversely associated with blood concentration of the liver enzymes. The associations were partly explained by adipocytokines (from 18.9% in aspartate aminotransaminase to 33.5% in alanine aminotransaminase). Thus, other factors would likely explain the associations of coffee consumption with liver enzymes.
We found no associations between coffee consumption and the markers of glucose metabolism. The present finding seemingly contradicts coffee's reported inverse association with DM incidence.3 A recent report also showed that coffee consumption was inversely associated with 2-h postload glucose of oral glucose tolerance test.37 We also did not find associations of coffee consumption with DM prevalence or with markers of glucose metabolism even in a sample without excluding subjects on medication for DM (data not shown). Nevertheless, it would be possible that the association of coffee consumption with glucose or insulin could not be observed in apparently healthy young population with low inter-individual variability. Indeed, it has been shown that fasting glucose concentrations and insulin sensitivity show changes starting 3 to 5 years before a diagnosis of DM,38 and that the onset of DM is often rapid rather than gradual.39 It has also been reported that the prevalence of DM rapidly rises in people 60 years or older in Japan.40 Thus, it may be possible that examination of older subjects or a sample with greater inter-individual variability of glucose level might reveal associations of coffee consumption with markers of the glucose metabolism.
This study has some potential limitations to be considered. First, because it is a cross-sectional study, causality can only be inferred. However, as it is less likely that adipocytokines or other markers influence coffee consumption, we consider our inference plausible that coffee consumption may have primary effects on adipocytokines and other markers investigated in the present study. In addition, we have excluded subjects who had been medically treated for several conditions. Although there may be individuals with other conditions (e.g., these chronic conditions without medication, gastrointestinal disorders and so on), which could confound the association, we considered this would have minor effects. Second, there may be some misclassification of daily coffee consumption doses based on the self-administered questionnaire. However, such a misclassification would have been nondifferential. Third, we did not obtain anthropometric measurements other than BMI. The possibility that a residual confounding of body fat distribution exists cannot be excluded. Finally, as all subjects in the present study were Japanese, the present findings may not apply directly to other races.
In conclusion, we found that coffee consumption was positively associated with adiponectin, and inversely with leptin levels in middle-aged Japanese workers. Such associations explained most of the associations of coffee consumption with triglycerides, and some of those on hs-CRP and liver enzymes. Further studies are necessary to determine whether the mediation effects of adipocytokines on the associations of coffee consumption with metabolic markers are causal.
References
Hu G, Jousilahti P, Peltonen M, Bidel S, Tuomilehto J . Joint association of coffee consumption and other factors to the risk of type 2 diabetes: a prospective study in Finland. Int J Obes 2006; 30: 1742–1749.
Sofi F, Conti AA, Gori AM, Eliana Luisi ML, Casini A, Abbate R et al. Coffee consumption and risk of coronary heart disease: a meta-analysis. Nutr Metab Cardiovasc Dis 2007; 17: 209–223.
van Dam RM, Hu FB . Coffee consumption and risk of type 2 diabetes: a systematic review. JAMA 2005; 294: 97–104.
Lancaster T, Muir J, Silagy C . The effects of coffee on serum lipids and blood pressure in a UK population. J R Soc Med 1994; 87: 506–507.
Miyake Y, Kono S, Nishiwaki M, Hamada H, Nishikawa H, Koga H et al. Relationship of coffee consumption with serum lipids and lipoproteins in Japanese men. Ann Epidemiol 1999; 9: 121–126.
Kempf K, Herder C, Erlund I, Kolb H, Martin S, Carstensen M et al. Effects of coffee consumption on subclinical inflammation and other risk factors for type 2 diabetes: a clinical trial. Am J Clin Nutr 2010; 91: 950–957.
Greenberg JA, Boozer CN, Geliebter A . Coffee, diabetes, and weight control. Am J Clin Nutr 2006; 84: 682–693.
Lopez-Garcia E, van Dam RM, Qi L, Hu FB . Coffee consumption and markers of inflammation and endothelial dysfunction in healthy and diabetic women. Am J Clin Nutr 2006; 84: 888–893.
Kono S, Shinchi K, Imanishi K, Todoroki I, Hatsuse K . Coffee and serum gamma-glutamyltransferase: a study of self-defense officials in Japan. Am J Epidemiol 1994; 139: 723–727.
Nakanishi N, Nakamura K, Nakajima K, Suzuki K, Tatara K . Coffee consumption and decreased serum gamma-glutamyltransferase: a study of middle-aged Japanese men. Eur J Epidemiol 2000; 16: 419–423.
Zampelas A, Panagiotakos DB, Pitsavos C, Chrysohoou C, Stefanadis C . Associations between coffee consumption and inflammatory markers in healthy persons: the ATTICA study. Am J Clin Nutr 2004; 80: 862–867.
Kadowaki T, Yamauchi T, Kubota N, Hara K, Ueki K, Tobe K . Adiponectin and adiponectin receptors in insulin resistance, diabetes, and the metabolic syndrome. J Clin Invest 2006; 116: 1784–1792.
Kim SG, Kim HY, Seo JA, Lee KW, Oh JH, Kim NH et al. Relationship between serum adiponectin concentration, pulse wave velocity and nonalcoholic fatty liver disease. Eur J Endocrinol 2005; 152: 225–231.
Li S, Shin HJ, Ding EL, van Dam RM . Adiponectin levels and risk of type 2 diabetes: a systematic review and meta-analysis. JAMA 2009; 302: 179–188.
Morton GJ . Hypothalamic leptin regulation of energy homeostasis and glucose metabolism. J Physiol 2007; 583: 437–443.
Tschritter O, Fritsche A, Thamer C, Haap M, Shirkavand F, Rahe S et al. Plasma adiponectin concentrations predict insulin sensitivity of both glucose and lipid metabolism. Diabetes 2003; 52: 239–243.
Wannamethee SG, Tchernova J, Whincup P, Lowe GD, Kelly A, Rumley A et al. Plasma leptin: associations with metabolic, inflammatory and haemostatic risk factors for cardiovascular disease. Atherosclerosis 2007; 191: 418–426.
Imatoh T, Tanihara S, Miyazaki M, Momose Y, Uryu Y, Une H . Coffee consumption but not green tea consumption is associated with adiponectin levels in Japanese males. Eur J Nutr 2011; 50: 279–284.
Williams CJ, Fargnoli JL, Hwang JJ, van Dam RM, Blackburn GL, Hu FB et al. Coffee consumption is associated with higher plasma adiponectin concentrations in women with or without type 2 diabetes: a prospective cohort study. Diabetes Care 2008; 31: 504–507.
Kotani K, Fujiwara S, Hamada T, Tsuzaki K, Sakane N . Coffee consumption is associated with higher plasma adiponectin concentrations in women with or without type 2 diabetes: response to Williams et al. Diabetes Care 2008; 31: e46 author reply e47.
Lagiou P, Signorello LB, Mantzoros CS, Trichopoulos D, Hsieh CC, Trichopoulou A . Hormonal, lifestyle, and dietary factors in relation to leptin among elderly men. Ann Nutr Metab 1999; 43: 23–29.
Laaksonen DE, Lakka HM, Salonen JT, Niskanen LK, Rauramaa R, Lakka TA . Low levels of leisure-time physical activity and cardiorespiratory fitness predict development of the metabolic syndrome. Diabetes Care 2002; 25: 1612–1618.
Japan Science and Technology Agency. Standard Tables of Food Composition in Japan 5th revised edn. Printing Bureau of the Ministry of Finance: Tokyo, Japan, 2005 (In Japanese).
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis 2009; 53: 982–992.
Preacher KJ, Hayes AF . Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods 2008; 40: 879–891.
Gressner OA, Lahme B, Rehbein K, Siluschek M, Weiskirchen R, Gressner AM . Pharmacological application of caffeine inhibits TGF-beta-stimulated connective tissue growth factor expression in hepatocytes via PPARgamma and SMAD2/3-dependent pathways. J Hepatol 2008; 49: 758–767.
Anghel SI, Bedu E, Vivier CD, Descombes P, Desvergne B, Wahli W . Adipose tissue integrity as a prerequisite for systemic energy balance: a critical role for peroxisome proliferator-activated receptor gamma. J Biol Chem 2007; 282: 29946–29957.
Fransson EI, Batty GD, Tabak AG, Brunner EJ, Kumari M, Shipley MJ et al. Association between change in body composition and change in inflammatory markers: an 11-year follow-up in the Whitehall II Study. J Clin Endocrinol Metab 2010; 95: 5370–5374.
Considine RV, Sinha MK, Heiman ML, Kriauciunas A, Stephens TW, Nyce MR et al. Serum immunoreactive-leptin concentrations in normal-weight and obese humans. N Eng J Med 1996; 334: 292–295.
Heymsfield SB, Greenberg AS, Fujioka K, Dixon RM, Kushner R, Hunt T et al. Recombinant leptin for weight loss in obese and lean adults: a randomized, controlled, dose-escalation trial. JAMA 1999; 282: 1568–1575.
Martin SS, Qasim A, Reilly MP . Leptin resistance: a possible interface of inflammation and metabolism in obesity-related cardiovascular disease. J Am Coll Cardiol 2008; 52: 1201–1210.
Hukshorn CJ, Lindeman JH, Toet KH, Saris WH, Eilers PH, Westerterp-Plantenga MS et al. Leptin and the proinflammatory state associated with human obesity. J Clin Endocrinol Metab 2004; 89: 1773–1778.
Sun H, Zhang Y, Gao P, Li Q, Sun Y, Zhang J et al. Adiponectin reduces C-reactive protein expression and downregulates STAT3 phosphorylation induced by IL-6 in HepG2 cells. Mol Cell Biochem 2011; 347: 183–189.
Jee SH, He J, Appel LJ, Whelton PK, Suh I, Klag MJ . Coffee consumption and serum lipids: a meta-analysis of randomized controlled clinical trials. Am J Epidemiol 2001; 153: 353–362.
MacKinnon DP, Krull JL, Lockwood CM . Equivalence of the mediation, confounding and suppression effect. Prev Sci 2000; 1: 173–181.
Urgert R, Katan MB . The cholesterol-raising factor from coffee beans. Ann Rev Nutr 1997; 17: 305–324.
Loopstra-Masters RC, Liese AD, Haffner SM, Wagenknecht LE, Hanley AJ . Associations between the intake of caffeinated and decaffeinated coffee and measures of insulin sensitivity and beta cell function. Diabetologia 2011; 54: 320–328.
Tabak AG, Jokela M, Akbaraly TN, Brunner EJ, Kivimaki M, Witte DR . Trajectories of glycaemia, insulin sensitivity, and insulin secretion before diagnosis of type 2 diabetes: an analysis from the Whitehall II study. Lancet 2009; 373: 2215–2221.
Ferrannini E, Nannipieri M, Williams K, Gonzales C, Haffner SM, Stern MP . Mode of onset of type 2 diabetes from normal or impaired glucose tolerance. Diabetes 2004; 53: 160–165.
National Institute of Health and Nutrition. Estimated Numbers Related to Diabetes. Estimates of the National Health and Nutrition Survey in Japan, 2007 (Internet). Health Service Bureau, Ministry of Health Labour and Welfare: Japan, 2007. Available from http://www.nih.go.jp/eiken/english/research/project_nhns.html (Cited 18 March, 2011).
Acknowledgements
The authors wish to express their sincere appreciation to the participants, and to the healthcare personnel of the local government office.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-No Derivative Works 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Yamashita, K., Yatsuya, H., Muramatsu, T. et al. Association of coffee consumption with serum adiponectin, leptin, inflammation and metabolic markers in Japanese workers: a cross-sectional study. Nutr & Diabetes 2, e33 (2012). https://doi.org/10.1038/nutd.2012.6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nutd.2012.6
Keywords
This article is cited by
-
Dietary caffeine intake is associated with favorable metabolic profile among apparently healthy overweight and obese individuals
BMC Endocrine Disorders (2023)
-
Post-diagnostic coffee and tea consumption and breast cancer survival
British Journal of Cancer (2021)
-
Regularly consuming a green/roasted coffee blend reduces the risk of metabolic syndrome
European Journal of Nutrition (2018)
-
J-shaped relationship between habitual coffee consumption and 10-year (2002–2012) cardiovascular disease incidence: the ATTICA study
European Journal of Nutrition (2018)
-
Effects of combined extract of cocoa, coffee, green tea and garcinia on lipid profiles, glycaemic markers and inflammatory responses in hamsters
BMC Complementary and Alternative Medicine (2015)
