
Abstract
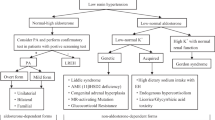
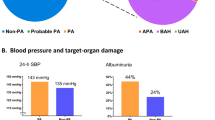
Metabolic syndrome (MS) is frequent clinical condition in patients with hypertension. Primary aldosteronism (PA) is a common form of secondary hypertension. This study was aimed at investigating the prevalence of the MS and its components in the two major forms of PA, in unilateral aldosterone-producing adenoma (APA) and bilateral aldosterone overproduction because of idiopathic hyperaldosteronism (IHA). The diagnosis of the particular form of PA was based on adrenal venous sampling and/or successful surgery confirmed by histopathological examination. We analyzed clinical and laboratory data from 100 patients with PA (50 patients with IHA and 50 patients with APA) and from 90 patients with essential hypertension (EH). Metabolic profiles of patients with bilateral form of PA (because of IHA) were similar to EH, but differed from those in patients with unilateral form of PA (APA). The prevalence of the MS (62% in IHA, 34% in APA and 56% in EH), the body mass index value (30±4 kg m–2 in IHA, 27±5 kg m–2 in APA and 29±5 kg m–2 in EH) and triglycerides levels (1.9±0.9 mmol l–1 in IHA,1.4±0.8 mmol l–1 in APA and 2.01±1.39 mmol l–1 in EH) were all significantly (P<0.05) higher in IHA compared with APA patients. Metabolic profile of patients with bilateral form of PA (because of IHA) is similar to EH in contrast to unilateral form of PA (APA).
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Redon J, Cifkova R, Laurent S, Nilsson P, Narkiewicz K, Erdine S et al. The metabolic syndrome in hypertension: European society of hypertension position statement. J Hypertens 2008; 26 (10): 1891–1900.
Eckel RH, Grundy SM, Zimmet PZ . The metabolic syndrome. Lancet 2005; 365: 1415.
Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G et al. 2007 Guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2007; 28: 1462–1536.
Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C et al. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol 2006; 48: 2293–2300.
Štrauch B, Zelinka T, Hampf M, Bernhardt R, Widimsky J . Prevalence of primary hyperaldosteronism in moderate to severe hypertension in the Central Europe region. J Hum Hypertens 2003; 17: 349–352.
Milliez P, Girerd X, Plouin PF, Blacher J, Safar ME, Mourad JJ . Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. J Am Coll Cardiol 2005; 45: 1243–1248.
Rossi GP, Sacchetto A, Visentin P, Canali C, Graniero GR, Palatini P et al. Changes in left ventricular anatomy and function in hypertension and primary aldosteronism. Hypertension 1996; 27: 1039–1045.
Sechi LA, Novello M, Lapenna R, Baroselli S, Nadalini E, Colussi GL et al. Long-term renal outcomes in patients with primary aldosteronism. JAMA 2006; 295: 2638–2645.
Holaj R, Zelinka T, Wichterle D, Petrák O, Strauch B, Widimský Jr J . Increased intima-media thickness of the common carotid artery in primary aldosteronism in comparison with essential hypertension. J Hypertens 2007; 25: 1451–1457.
Strauch B, Petrák O, Wichterle D, Zelinka T, Holaj R, Widimský Jr J . Increased arterial wall stiffness in primary aldosteronism in comparison with essential hypertension. Am J Hypertens 2006; 19: 909–914.
Krug AW, Ehrhart-Bornstein M . Aldosterone and metabolic syndrome: is increased aldosterone in metabolic syndrome patients an additional risk factor? Hypertension 2008; 51: 1252–1258.
Sowers JR, Whaley-Connell A, Epstein M . Narrative review: the emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann Intern Med 2009; 150: 776–783.
Fallo F, Veglio F, Bertello C, Sonino N, Della Mea P, Ermani M et al. Prevalence and characteristics of the metabolic syndrome in primary aldosteronism. J Clin Endocrinol Metab 2006; 91: 454–459.
Fallo F, Federspil G, Veglio F, Mulatero P . The metabolic syndrome in primary aldosteronism. Curr Hypertens Rep 2007; 9: 106–111.
Ronconi V, Turchi F, Rilli S, Di Mattia D, Agostinelli L, Boscaro M et al. Metabolic syndrome in primary aldosteronism and essential hypertension: relationship to adiponectin gene variants. Nutr Metab Cardiovasc Dis 2010; 20: 93–100.
Matrozova J, Steichen O, Amar L, Zacharieva S, Jeunemaitre X, Plouin PF . Fasting plasma glucose and serum lipids in patients with primary aldosteronism: a controlled cross-sectional study. Hypertension 2009; 53: 605–610.
Funder JW, Carey RM, Fardella C, Gomez-Sanchez CE, Mantero F, Stowasser M et al. Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 2008; 93: 3266–3281.
Alberti KGMM, Zimmet P, Shaw J . Metabolic syndrome--a new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet Med 2006; 23: 469–480.
Alberti K, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA et al. Harmonizing the metabolic syndrome: a Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009; 120: 1640–1645.
McAreavey D, Murray G, Lever A, Robertson J . Similarity of idiopathic aldosteronism and essential hypertension. A statistical comparison. Hypertension 1983; 5: 116–121.
Bochud M, Nussberger J, Bovet P, Maillard MR, Elston RC, Paccaud F et al. Plasma aldosterone is independently associated with the metabolic syndrome. Hypertension 2006; 48: 239–245.
Kidambi S, Kotchen JM, Grim CE, Raff H, Mao J, Singh RJ et al. Association of adrenal steroids with hypertension and the metabolic syndrome in Blacks. Hypertension 2007; 49: 704–711.
Rossi GP, Belfiore A, Bernini G, Fabris B, Caridi G, Ferri C et al. Body mass index predicts plasma aldosterone concentrations in overweight-obese primary hypertensive patients. J Clin Endocrinol Metab 2008; 93: 2566–2571.
Lastra-Lastra G, Sowers JR, Restrepo-Erazo K, Manrique-Acevedo C, Lastra-González G . Role of aldosterone and angiotensin II in insulin resistance: an update. Clin Endocrinol 2009; 71: 1–6.
Zennaro M, Caprio M, Fève B . Mineralocorticoid receptors in the metabolic syndrome. Trends Endocrinol Metab 2009; 20: 444–451.
Henquin JC . Triggering and amplifying pathways of regulation of insulin secretion by glucose. Diabetes 2000; 49: 1751–1760.
Fallo F, Della Mea P, Sonino N, Bertello C, Ermani M, Vettor R et al. Adiponectin and insulin sensitivity in primary aldosteronism. Am J Hypertens 2007; 20: 855–861.
Sindelka G, Widimský J, Haas T, Prázný M, Hilgertová J, Skrha J . Insulin action in primary hyperaldosteronism before and after surgical or pharmacological treatment. Exp Clin Endocrinol Diabetes 2000; 108: 21–25.
Widimský J, Strauch B, Sindelka G, Skrha J . Can primary hyperaldosteronism be considered as a specific form of diabetes mellitus? Physiol Res 2001; 50: 603–607.
Fallo F, Federspil G, Veglio F, Mulatero P . The metabolic syndrome in primary aldosteronism. Curr Diab Rep 2008; 8: 42–47.
Catena C, Lapenna R, Baroselli S, Nadalini E, Colussi G, Novello M et al. Insulin sensitivity in patients with primary aldosteronism: a follow-up study. J Clin Endocrinol Metab 2006; 91: 3457–3463.
Giacchetti G, Turchi F, Boscaro M, Ronconi V . Management of primary aldosteronism: its complications and their outcomes after treatment. Curr Vasc Pharmacol 2009; 7: 244–249.
Acknowledgements
This work was supported by Research projects from Czech Ministry of Education, Youth and Sports No: 21620807 and 21620817.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Šomlóová, Z., Widimský, J., Rosa, J. et al. The prevalence of metabolic syndrome and its components in two main types of primary aldosteronism. J Hum Hypertens 24, 625–630 (2010). https://doi.org/10.1038/jhh.2010.65
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhh.2010.65
Keywords
This article is cited by
-
Visceral fat: a bad companion for mineralocorticoid receptor overactivation
Hypertension Research (2023)
-
Fat mass: the most sensitive predictor of persistent hypertension in unilateral primary aldosteronism
Hypertension Research (2023)
-
New-onset diabetes mellitus risk associated with concurrent autonomous cortisol secretion in patients with primary aldosteronism
Hypertension Research (2023)
-
Is adrenal venous sampling always necessary to differentiate between unilateral and bilateral primary aldosteronism? Lesson from the SPAIN-ALDO register
Endocrine (2023)
-
The differences of serum lipid profiles between primary aldosteronism and essential hypertension: a meta-analysis and systematic review
BMC Endocrine Disorders (2022)
