
Abstract
The dysbindin-1 and neuregulin-1 (NRG-1) genes are related to schizophrenia. Expression studies in postmortem brains have revealed lower expression of dysbindin-1 and higher expression of NRG-1 in brain tissue from subjects with schizophrenia. In addition to the difficulty of sampling, the use of postmortem brain tissues is not ideal because these tissues are heterogeneous with respect to biochemical parameters, lifetime history of medications and physiological status at the time of death. In contrast, medication and environmental influences that could mask the genetic basis of differences in RNA expression are removed in immortalized lymphocytes by culturing. Only a few microarray analysis studies using immortalized lymphocytes in schizophrenia have been reported, and whether immortalized lymphocytes are an appropriate alternative to neuronal tissue remains controversial. In this study, we measured the mRNA expression levels of dysbindin-1, NRG-1 and two other genes (NPY1R and GNAO1) in immortalized lymphocytes from 45 patients with schizophrenia and 45 controls using real-time quantitative reverse transcriptase-PCR. No difference was observed between patients and controls with respect to the expression of dysbindin-1, NRG-1, NPY1R or GNAO1 gene. Our findings suggest that the gene expression profile of immortalized lymphocyte from schizophrenic patients is different from that in postmortem brain tissue at least with respect to the dysbindin-1 and NRG-1 genes.
Similar content being viewed by others


Introduction
Schizophrenia is a complex genetic disorder that is characterized by profound disturbances of cognition, emotion and social functioning. It affects ∼1% of the general population world wide. The dysbindin-1 and neuregulin-1 (NRG-1) genes are related to schizophrenia,1 and the dysbindin-1 gene is also associated with cognitive functions.2, 3, 4 Furthermore, the Sandy mouse, which expresses no dysbindin-1, has been reported to have behavioral abnormalities, cognitive deficits and a synaptic dysfunction that is related to the pathophysiology of schizophrenia.5, 6, 7 Identified risk variants of NRG-1 are associated with the reduced white matter volume that is observed in schizophrenic brains.8 The NRG-1 gene spans 1.2 Mb9 and gives rise to many structurally and functionally distinct isoforms, through alternative promoter usage. These isoforms are divided into three classic groups:10 type I (previously known as acetylcholine receptor inducing activity, heregulin or neu differentiation factor), type II (glia growth factor) and type III (cysteine-rich domain containing), which are based on distinct amino termini. Additional NRG-1 5′ exons have recently been identified, giving rise putatively to novel NRG-1 types IV–VI in the human brain.11 Transgenic mice that overexpress NRG-1 type I, the expression of which is reported to be increased in the schizophrenic brains,12 have a tremor, show impaired ability on the accelerating rotarod and have reduced prepulse inhibition.13 Expression studies in postmortem brains have also revealed lower expression of dysbindin-1 and higher expression of NRG-1 type I, in subjects with schizophrenia.12, 14, 15, 16
Postmortem brain tissues are necessary for determining the pathophysiology of schizophrenia. Many gene expression studies have been conducted using postmortem brain tissues. These studies have demonstrated increased expression of genes involved in presynaptic function17, 18 and the downregulation of myelination-related genes.19, 20 Although there is some agreement across these studies, there has been a lack of consistency because of the varying characteristics of postmortem brain tissues. Postmortem brain tissues are not easy to obtain. Moreover, postmortem brain tissues are quite heterogeneous with respect to biochemical parameters, lifetime history of medications and physiological status at the time of death and sampling.
In contrast, medication and environmental influences that could mask the genetic basis of differences in RNA expression may be removed in immortalized lymphocytes by culturing. Immortalized lymphocytes can be readily obtained, in contrast to postmortem brain tissues, thereby allowing larger case–control expression studies with optimal matching on key variables such as age and sex. The gene expression profile of whole blood has been shown to have moderate degree of similarity to that of the central nervous system among 79 human tissues.21 For these reasons, immortalized lymphocytes are good tools for determining the effect of genetic risks or drug treatment on gene expressions. Disrupted in schizophrenia 1 and a serotonin transporter polymorphism have been reported to have effect on their gene expressions in immortalized lymphocytes from bipolar disorder patients.22, 23 The effect of lithium on gene expression was also investigated in immortalized lymphocytes from bipolar disorder patients.24 However, only a few microarray analysis using immortalized lymphocytes from patients with schizophrenia have been reported.25, 26, 27 Whether immortalized lymphocytes are an appropriate alternative to neuronal tissue remains controversial.
A recent study using microarray analysis has shown that the expression levels of dysbindin-1 isoform A and the NRG-1 type II GGF2 isoform in immortalized lymphocytes are lower in patients with schizophrenia than in controls. In contrast, the expression of the NRG-1 type II GGF isoform was not significantly different between patients with schizophrenia and controls.28 In this study, the expression profiles of dysbindin-1 and NRG-1 in immortalized lymphocytes were partly consistent with those in postmortem brains. However, a limited number of subjects were used, and a limited number of dysbindin-1 and NRG-1 isoforms was observed, therefore whether the expression profile of dysbindin-1 and NRG-1 in immortalized lymphocytes is consistent with that in the postmortem brain remains controversial.
In this study, we used approximately four times as many subjects as the previous study. We observed the total expression of dysbindin-1 and NRG-1 (that is, the combined expression of all isoforms), which had previously been observed in a postmortem brain,12, 14, 15, 16 to determine whether immortalized lymphocytes are a good tool to determine the effect of genetic risks of dysbindin-1 and NRG-1 on their expression and whether immortalized lymphocytes are an appropriate alternative to neuronal tissue.
Materials and methods
Subjects
In all, 45 Japanese patients with schizophrenia and 45 healthy Japanese control subjects participated in this study. Patients were recruited at Osaka University Hospital. Controls were recruited by local advertisements in Osaka.
Consensus diagnosis was made for each patient by at least two trained psychiatrists, according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria using the structured clinical interview for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (severe combined immunodeficiency). Controls were psychiatrically, medically and neurologically healthy volunteers who were not receiving psychiatric medication and had no first- or second-degree relatives with psychoses. Controls were screened for psychiatric disease with the non-patient edition of the modified structured clinical interview for the Diagnostic and Statistical Manual, Fourth Edition, Axis I disorders (severe combined immunodeficiency-I/non-patient). Symptoms of schizophrenia were assessed using the positive and negative syndrome scale. The clinical and demographic characteristics of all subjects are presented in Table 1. Patients and controls were matched for age and sex. All patients were treated with antipsychotics.
Immortalized lymphocytes and RNA extraction
The isolation of lymphocytes from the blood and immortalization using Epstein–Bar virus were performed by the Special Reference Laboratories (Tokyo, Japan). Immortalized lymphocytes from 45 patients with schizophrenia and from 45 controls were grown in culture media supplemented with 20% fetal bovine serum. Total RNA was extracted from cell pellets using the RNeasy mini kit (QIAGEN KK, Tokyo, Japan). The yield of total RNA was determined by measuring the absorbance at 260 nm, and the quality of the total RNA was analyzed using agarose gel electrophoresis.
DNase treatment and reverse transcription
Total RNA was treated with DNase to remove contaminating genomic DNA using the DNase Treatment & Removal Reagents (Ambion, Austin, TX, USA) according to the manufacturer's protocol. Total RNA (10 μg) treated with DNase was used in a 50 μl reverse transcriptase (RT) reaction to synthesize complementary DNA using the SuperScript first-strand synthesis system for reverse transcriptase-PCR (RT-PCR; Invitrogen, Carlsbad, CA, USA), according to the manufacturer's protocol. Briefly, total RNA (10 μg) was denatured in the presence of 1 mM deoxyribonucleotide triphosphates and 5 ng μl–1 random hexamers at 65 °C for 5 min. After the addition of RT buffer, MgCl2 (5 mM final concentration), dithiothreitol (10 mM final concentration), RNAseOUT recombinant ribonuclease inhibitor (100 U) and SuperScriptIII RT (125 U), the reaction mixture was incubated at 25 °C for 10 min, at 42 °C for 40 min and at 70 °C for 15 min. RNase H (5 U) was added to the reaction mixture, and then the mixture was incubated at 37 °C for 20 min to stop the reaction.
Oligonucleotide and primer design
The TaqMan Pre-Developed Assay Reagent kit (Applied Biosystems, Foster City, CA, USA) was used for the analysis of two housekeeping genes, β-actin and glyceraldehyde 3-phosphate dehydrogenase (GAPDH), and for dysbindin-1 (Hs00225229 m1), NPY1R (Hs00702150_s1) and GNAO1 (Hs00221365_m1).
The primer and probes for NRG-1 types I to IV were as described previously.12, 16 The real-time PCR (TaqMan) detection of NRG-1 isoforms used the following oligonucleotides: type I, forward primer 5′-GCCAATATCACCATCGTGGAA-3′, reverse primer 5′-CCTTCAGTTGAGGCTGGCATA-3′, probe 5′-FAM-CAAACGAGATCATCACTGMGB-3′; type II, forward primer 5′-GAATCAAACGCTACATCTACATCCA-3′, reverse primer 5′-CCTTCTCCGCACATTTTACAAGA-3′, probe 5′-FAM-CACTGGGACAAGCC-MGB-3′; type III, forward primer 5′-CAGCCACAAACAACAGAAACTAATC-3′, reverse primer 5′-CCCAGTGGTGGATGTAGATGTAGA-3′, probe 5′-FAMCCAAACTGCTCCTAAAC-MGB-3′ and type IV, forward primer 5′-GCTCCGGCAGCAGCAT-3′, reverse primer 5′-GAACCTGCAGCCGATTCCT-3′, probe 5′-FAM-ACCACAGCCTTGCCT-MGB-3′ (purchased from Applied Biosystems). These primers were designed to amplify specific transcripts based on the unique exon structure of each isoform. Thus, for example, because isoform II lacks exons 5–7, primers complementary to sections of exons 4 and 8, which are contiguous in the isoform II transcript, will only amplify this isoform.
Real-time quantitative RT-PCR
Dysbindin-1 and NRG-1 mRNA expression levels were measured by real-time quantitative RT-PCR, using each combination of oligonucleotides and an ABI Prism 7900 sequence detection system with a 384-well format (Applied Biosystems). Each 20 μl PCR reaction contained 6 μl of complementary DNA, 900 nM of each primer, 250 nM of probe and 10 μl of TaqMan Universal PCR Master Mix (Applied Biosystems) containing AmpliTaq Gold DNA polymerase, AmpErase UNG, deoxyribonucleotide triphosphates with deoxyuridine triphosphate, a passive reference and optimized buffer components. The PCR cycling conditions were 50 °C for 2 min, 95 °C for 10 min, 40 cycles of 95 °C for 15 s and 59 °C or 60 °C for 1 min. PCR data were obtained using the Sequence Detector Software (version 2.1, Applied Biosystems) and were quantified by a standard curve method. This software plotted the real-time fluorescence intensity and selected the threshold within the linear phase of the amplicon profile. The software plotted a standard curve of the cycle at the threshold (Ct; where the fluorescence generated within a reaction and threshold cross) versus the quantity of RNA. All samples were measured in one plate for one target gene or isoform, and their Ct-values were in the linear range of the standard curve. Experiments were typically performed three times with triplicate determinations and the expression level of each gene was determined by the average of the three independent experiments. Predicted Ct-values and sample quantities were used for statistical analysis.
Statistical analysis
The individual Mann–Whitney U-test and the χ2-test were used to compare means and categorical proportions, respectively. The groups did not differ with respect to age or gender (Table 1). The differences in the mRNA levels of dysbindin-1, NRG-1 type II, NPY1R and GNAO1 between patients and controls were also analyzed by analysis of covariance, with diagnosis as the independent factor and sex and age as covariates. Spearman rank order correlation test was performed to assess the possible correlation between gene expressions and clinical characteristics.
Results
To measure the expression levels of dysbindin-1 and NRG-1 in immortalized lymphocytes, standard curves were obtained using serial dilutions (1:4) of pooled complementary DNA prepared from 300 ng total RNA derived from immortalized lymphocytes. For NRG-1 types I, II, III and IV, the same amount of RNA from a postmortem brain (a kind gift from the Stanley Foundation) was also used as a positive control. The standard curves of two housekeeping genes, β-actin and GAPDH, and of dysbindin-1 showed that these genes were expressed in immortalized lymphocytes (Figures 1a–c). Although the expression of NRG-1 type II was observed in immortalized lymphocytes, the expression levels of NRG-1 types I, III and IV were below the detection limit of the real-time quantitative RT-PCR assay (Figures 1d–g). The expressions of NRG-1 types I, II, III and IV in the postmortem brain were confirmed by the real-time quantitative RT-PCR method, as previously reported (Figures 1d–g).12, 16 In each experiment for β-actin, GAPDH, dysbindin-1 and NRG-1 type II the R2-value of the standard curve was >0.99, and no-template control assays resulted in no detectable signal.

Standard curves for the housekeeping genes, dysbindin-1 and the four NRG-1 isoforms. (a, b) Standard curves for the house keeping genes, β-actin (a) and GAPDH (b). (c) Standard curve for dysbindin-1. The expression of the dysbindin-1 gene was observed in immortalized lymphocytes. (d–g) Standard curves for NRG1 types I (d), II (e), III (f) and IV (g). The expression of NRG-1 types I, II, III and IV was observed in the postmortem brain, as previously reported. The expression of NRG-1 type II was observed in immortalized lymphocytes. The expression levels of NRG-1 types I, III and IV in immortalized lymphocytes were below the detection limit of the real-time quantitative RT-PCR assay.
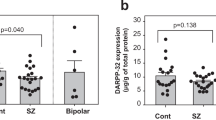
The expression levels of β-actin and GAPDH were not significantly different between the 45 patients with schizophrenia and the 45 age- and sex-matched controls (Figure 2a). No significant difference was observed between the 45 patients with schizophrenia and the 45 controls with respect to the expression of dysbindin-1 and NRG-1 type II normalized to the expression of β-actin or GAPDH (Figures 2b and c; Mann–Whitney U-test: dysbindin-1/β-actin; U=916, P=0.436, dysbindin-1/GAPDH; U=952, P=0.625, NRG-1 type II/β-actin; U=961, P=0.678, NRG-1 type II/GAPDH; U=977, P=0.775). Analysis of covariance with sex and age as covariates did not alter the results (dysbindin-1/β-actin; F=0.267, P=0.607, dysbindin-1/GAPDH; F=0.06, P=0.808, NRG-1 type II/β-actin; F=2.412, P=0.124, NRG-1 type II/GAPDH; F=1.693, P=0.197).

Control gene, dysbindin-1 and NRG-1 type II expression levels. (a) The expression levels of the house keeping genes β-actin and GAPDH. The expression levels of the two standard housekeeping genes were not significantly different between patients with schizophrenia and controls. (b) The expression levels of dysbindin-1 normalized by β-actin and GAPDH expression. (c) The expression levels of NRG-1 type II normalized by β-actin and GAPDH expression. No significant difference was observed between the 45 patients with schizophrenia and the 45 controls with respect to the expression of dysbindin-1 and NRG-1 type II normalized by β-actin and GAPDH and expression. The bars show the means.
A correlation test was performed to observe the influence of clinical characteristics on the expression levels of dysbindin-1 and NRG-1 type II in immortalized lymphocytes from patients with schizophrenia. None of the measurements of dysbindin-1 and NRG-1 type II expression normalized by β-actin and GAPDH expression correlated significantly with age, age of onset, duration of illness, chlorpromazine equivalents, positive and negative syndrome scale positive, negative or general psychopathology scores (Spearman rank order correlation test: all P>0.1).
The expression levels of NPY1R and GNAO1, which were reported to be differentially expressed in schizophrenic immortalized lymphocytes,25 were also measured to further assess the usefulness of immortalized lymphocytes from patients with schizophrenia. No significant difference was observed between the 45 patients with schizophrenia and the 45 controls with respect to the expression of NPY1R and GNAO1 normalized to the expression of β-actin or GAPDH (Figures 3a and b) (Mann–Whitney U-test: NPY1R/β-actin; U=949, P=0.606, NPY1R/GAPDH; U=949, P=0.608, GNAO1/β-actin; U=932, P=0.516, GNAO1/GAPDH; U=965, P=0.701). An analysis of covariance with sex and age as covariates did not alter the results (NPY1R/β-actin; F=2.940, P=0.090, NPY1R/GAPDH; F=1.756, P=0.189, GNAO1/β-actin; F=0.004, P=0.950, GNAO1/GAPDH; F=0.007, P=0.935).

NPY1R and GNAO1 expression levels. (a) The expression levels of NPY1R normalized by β-actin and GAPDH expression. (b) The expression levels of GNAO1 normalized by β-actin and GAPDH expression. No significant difference was observed between the 45 patients with schizophrenia and the 45 controls with respect to the expression of NPY1R and GNAO1 normalized by β-actin and GAPDH expression. The bars show the means.
Discussion
We confirmed the expression of dysbindin-1 and NRG-1 types I, II, III and IV in postmortem brain.16 However, the expression levels of NRG-1 types I, III and IV were below the detection limit of the real-time quantitative RT-PCR assay, and only dysbindin-1 and NRG-1 type II expression was observed in immortalized lymphocytes. In the postmortem brain, the expression of dysbindin-1 has been reported to be lower in patients with schizophrenia than in controls.14, 15 NRG-1 type I in the postmortem brain has been reported to be higher in patients with schizophrenia than in controls, and the expression of NRG-1 types II, III and IV in the postmortem brain has been reported to show no significant difference between patients with schizophrenia and controls.12, 16 In immortalized lymphocytes, we found no difference between patients with schizophrenia and controls with respect to the expression of dysbindin-1 and NRG-1 type II. The expression profile of NRG-1 type II in immortalized lymphocytes was consistent with that in the postmortem brain, but the expression profile of dysbindin-1 was not consistent with that in the postmortem brain. Our findings suggest that, in subjects with schizophrenia, the immortalized lymphocyte gene expression profile is different from that in postmortem brain tissue at least with respect to dysbindin-1 and NRG-1 genes. This difference in gene expression profile might be attributed to the differences of the tissue-specific regulation of gene expression and alternative splicing. Not only the tissue-specific regulation of gene expression but also the transformation process using Epstein–Bar virus and culturing might have effect on this difference in gene expression profiles. The expression profile in postmortem brain might be affected by medication and environmental influences that could be removed in immortalized lymphocytes by this transformation and culturing process.
We failed to replicate the abnormal expression of dysbindin-1 and NRG-1 in immortalized lymphocytes in our cohort, which consist of a much larger sample than that used in the previous study. The previous study showed that dysbindin-1 isoform A and NRG-1 type II isoform GGF2 in immortalized lymphocytes from patients with schizophrenia were decreased relative to that in controls.28 This discrepancy might be attributed to the differences in the isoforms observed, the sample size, the ethnicity of the subjects and the sample preparation. In this study, we used approximately four times more subjects than the previous study, and we observed the total expression of the genes (that is, the combined expression of all isoforms) in a Japanese sample population. To clarify this discrepancy, we should observe the expression levels of all of the isoforms of the genes individually (that is, dysbindin-1 isoform A and NRG-1 type II isoform GGF).
We have also measured the mRNA expression levels of NPY1R and GNAO1, which were reported to be differentially expressed in schizophrenic immortalized lymphocytes,25 using our cohort which consist of larger sample to further assess the usefulness of immortalized lymphocytes from patients with schizophrenia. We also failed to replicate the abnormal expression of NPY1R and GNAO1 in immortalized lymphocytes in our cohort, which consist of a much larger sample than that used in the previous study. This discrepancy might be attributed to the differences of the sample size, the ethnicity of the subjects or the sample preparation.
Although the dysbindin-1 and NRG-1 gene expression profiles in immortalized lymphocytes were different from those in postmortem brain tissue, it remains possible that immortalized lymphocytes could be good tools to determine the effect of genetic risks of the dysbindin-1 and NRG-1 genes on their expression, for example, the allele effects that have been reported to be associated with schizophrenia on their genes expressions. In immortalized lymphocytes, it might be difficult to observe the effect of dysbindin-1 and NRG-1 gene expression on their neuron-specific functions, for example, the effect of dysbindin-1 on glutamate and dopamine release,5, 6, 29 and on the formation of synaptic vesicles30 and the effect of NRG-1 on N-methyl D-aspartate receptor hypofunction.31 However, we might be able to determine the effect of dysbindin-1 and NRG-1 genes expression on their functions which are common in multiple tissues using immortalized lymphocytes, for example, the effect of dysbindin-1 on phosphatidylinositol 3 kinase–Akt signaling29 and the effect of NRG-1 on ErbB–Akt signaling. In fact, it has been reported that NRG-1-induced cell migration resulting from ErbB–Akt signaling is impaired in immortalized lymphocyte from patients with schizophrenia.32
Further studies are required to assess whether immortalized lymphocytes are a good tool to determine the effect of genetic risks on their gene expression and whether immortalized lymphocytes are an appropriate alternative to neuronal tissue.
References
Gill, M., Donohoe, G. & Corvin, A. What have the genomics ever done for the psychoses? Psychol. Med. 40, 529–540 (2010).
Hashimoto, R., Noguchi, H., Hori, H., Ohi, K., Yasuda, Y., Takeda, M. et al. Association between the dysbindin gene (DTNBP1) and cognitive functions in Japanese subjects. Psychiatry Clin. Neurosci. 63, 550–556 (2009).
Hashimoto, R., Noguchi, H., Hori, H., Nakabayashi, T., Suzuki, T., Iwata, N. et al. A genetic variation in the dysbindin gene (DTNBP1) is associated with memory performance in healthy controls. World J. Biol. Psychiatry 11, 431–438 (2010).
Burdick, K. E., Lencz, T., Funke, B., Finn, C. T., Szeszko, P. R., Kane, J. M. et al. Genetic variation in DTNBP1 influences general cognitive ability. Hum. Mol. Genet. 15, 1563–1568 (2006).
Murotani, T., Ishizuka, T., Hattori, S., Hashimoto, R., Matsuzaki, S. & Yamatodani, A. High dopamine turnover in the brains of Sandy mice. Neurosci. Lett. 421, 47–51 (2007).
Hattori, S., Murotani, T., Matsuzaki, S., Ishizuka, T., Kumamoto, N., Takeda, M. et al. Behavioral abnormalities and dopamine reductions in sdy mutant mice with a deletion in Dtnbp1, a susceptibility gene for schizophrenia. Biochem. Biophys. Res. Commun. 373, 298–302 (2008).
Takao, K., Toyama, K., Nakanishi, K., Hattori, S., Takamura, H., Takeda, M. et al. Impaired long-term memory retention and working memory in sdy mutant mice with a deletion in Dtnbp1, a susceptibility gene for schizophrenia. Mol. Brain 1, 11 (2008).
McIntosh, A. M., Moorhead, T. W., Job, D., Lymer, G. K., Munoz Maniega, S., McKirdy, J. et al. The effects of a neuregulin 1 variant on white matter density and integrity. Mol. Psychiatry 13, 1054–1059 (2008).
Stefansson, H., Sigurdsson, E., Steinthorsdottir, V., Bjornsdottir, S., Sigmundsson, T., Ghosh, S. et al. Neuregulin 1 and susceptibility to schizophrenia. Am. J. Hum. Genet. 71, 877–892 (2002).
Falls, D. L. Neuregulins and the neuromuscular system: 10 years of answers and questions. J. Neurocytol. 32, 619–647 (2003).
Steinthorsdottir, V., Stefansson, H., Ghosh, S., Birgisdottir, B., Bjornsdottir, S., Fasquel, A. C. et al. Multiple novel transcription initiation sites for NRG1. Gene 342, 97–105 (2004).
Hashimoto, R., Straub, R. E., Weickert, C. S., Hyde, T. M., Kleinman, J. E. & Weinberger, D. R. Expression analysis of neuregulin-1 in the dorsolateral prefrontal cortex in schizophrenia. Mol. Psychiatry 9, 299–307 (2004).
Deakin, I. H., Law, A. J., Oliver, P. L., Schwab, M. H., Nave, K. A., Harrison, P. J. et al. Behavioural characterization of neuregulin 1 type I overexpressing transgenic mice. Neuroreport 20, 1523–1528 (2009).
Talbot, K., Eidem, W. L., Tinsley, C. L., Benson, M. A., Thompson, E. W., Smith, R. J. et al. Dysbindin-1 is reduced in intrinsic, glutamatergic terminals of the hippocampal formation in schizophrenia. J. Clin. Invest. 113, 1353–1363 (2004).
Weickert, C. S., Straub, R. E., McClintock, B. W., Matsumoto, M., Hashimoto, R., Hyde, T. M. et al. Human dysbindin (DTNBP1) gene expression in normal brain and in schizophrenic prefrontal cortex and midbrain. Arch. Gen. Psychiatry 61, 544–555 (2004).
Law, A. J., Lipska, B. K., Weickert, C. S., Hyde, T. M., Straub, R. E., Hashimoto, R. et al. Neuregulin 1 transcripts are differentially expressed in schizophrenia and regulated by 5′ SNPs associated with the disease. Proc. Natl Acad. Sci. USA 103, 6747–6752 (2006).
Vawter, M. P., Barrett, T., Cheadle, C., Sokolov, B. P., Wood, W. H. III, Donovan, D. M. et al. Application of cDNA microarrays to examine gene expression differences in schizophrenia. Brain Res. Bull. 55, 641–650 (2001).
Chung, C., Tallerico, T. & Seeman, P. Schizophrenia hippocampus has elevated expression of chondrex glycoprotein gene. Synapse 50, 29–34 (2003).
Hakak, Y., Walker, J. R., Li, C., Wong, W. H., Davis, K. L., Buxbaum, J. D. et al. Genome-wide expression analysis reveals dysregulation of myelination-related genes in chronic schizophrenia. Proc. Natl Acad. Sci. USA 98, 4746–4751 (2001).
Tkachev, D., Mimmack, M. L., Ryan, M. M., Wayland, M., Freeman, T., Jones, P. B. et al. Oligodendrocyte dysfunction in schizophrenia and bipolar disorder. Lancet 362, 798–805 (2003).
Sullivan, P. F., Fan, C. & Perou, C. M. Evaluating the comparability of gene expression in blood and brain. Am. J. Med. Genet. B Neuropsychiatr. Genet. 141B, 261–268 (2006).
Hranilovic, D., Stefulj, J., Schwab, S., Borrmann-Hassenbach, M., Albus, M., Jernej, B. et al. Serotonin transporter promoter and intron 2 polymorphisms: relationship between allelic variants and gene expression. Biol. Psychiatry 55, 1090–1094 (2004).
Maeda, K., Nwulia, E., Chang, J., Balkissoon, R., Ishizuka, K., Chen, H. et al. Differential expression of disrupted-in-schizophrenia (DISC1) in bipolar disorder. Biol. Psychiatry 60, 929–935 (2006).
Sun, X., Young, L. T., Wang, J. F., Grof, P., Turecki, G., Rouleau, G. A. et al. Identification of lithium-regulated genes in cultured lymphoblasts of lithium responsive subjects with bipolar disorder. Neuropsychopharmacology 29, 799–804 (2004).
Vawter, M. P., Ferran, E., Galke, B., Cooper, K., Bunney, W. E. & Byerley, W. Microarray screening of lymphocyte gene expression differences in a multiplex schizophrenia pedigree. Schizophr. Res. 67, 41–52 (2004).
Liu, Y. L., Fann, C. S., Liu, C. M., Chang, C. C., Yang, W. C., Hung, S. I. et al. More evidence supports the association of PPP3CC with schizophrenia. Mol. Psychiatry 12, 966–974 (2007).
Matigian, N. A., McCurdy, R. D., Feron, F., Perry, C., Smith, H., Filippich, C. et al. Fibroblast and lymphoblast gene expression profiles in schizophrenia: are non-neural cells informative? PLoS One 3, e2412 (2008).
Chagnon, Y. C., Roy, M. A., Bureau, A., Merette, C. & Maziade, M. Differential RNA expression between schizophrenic patients and controls of the dystrobrevin binding protein 1 and neuregulin 1 genes in immortalized lymphocytes. Schizophr. Res. 100, 281–290 (2008).
Numakawa, T., Yagasaki, Y., Ishimoto, T., Okada, T., Suzuki, T., Iwata, N. et al. Evidence of novel neuronal functions of dysbindin, a susceptibility gene for schizophrenia. Hum. Mol. Genet. 13, 2699–2708 (2004).
Hikita, T., Taya, S., Fujino, Y., Taneichi-Kuroda, S., Ohta, K., Tsuboi, D. et al. Proteomic analysis reveals novel binding partners of dysbindin, a schizophrenia-related protein. J. Neurochem. 110, 1567–1574 (2009).
Hahn, C. G., Wang, H. Y., Cho, D. S., Talbot, K., Gur, R. E., Berrettini, W. H. et al. Altered neuregulin 1-erbB4 signaling contributes to NMDA receptor hypofunction in schizophrenia. Nat. Med. 12, 824–828 (2006).
Sei, Y., Ren-Patterson, R., Li, Z., Tunbridge, E. M., Egan, M. F., Kolachana, B. S. et al. Neuregulin1-induced cell migration is impaired in schizophrenia: association with neuregulin1 and catechol-o-methyltransferase gene polymorphisms. Mol. Psychiatry 12, 946–957 (2007).
Acknowledgements
We thank all the individuals who participated in this study. This work was funded in part by Grants-in-Aid from the Japanese Ministry of Health, Labor and Welfare (H19-kokoro-002); the Japanese Ministry of Education, Culture, Sports, Science and Technology (18689030); CREST of JST; and the Japan Foundation for Neuroscience and Mental Health and by a Grant-aid for Scientific Research on Priority Areas -Research on Pathomechanisms of Brain Disorders- from the MEXT (18023045). Postmortem brains were kindly donated by the Stanley Foundation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yamamori, H., Hashimoto, R., Verrall, L. et al. Dysbindin-1 and NRG-1 gene expression in immortalized lymphocytes from patients with schizophrenia. J Hum Genet 56, 478–483 (2011). https://doi.org/10.1038/jhg.2011.40
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhg.2011.40
Keywords
This article is cited by
-
Antipsychotic drugs increase Neuregulin1β1 serum levels in first-episode drug-naïve patients and chronic schizophrenia with suggestions for improving the treatment of psychotic symptoms
BMC Psychiatry (2022)
-
Altered gene expression in lymphoblastoid cell lines after subculture
In Vitro Cellular & Developmental Biology - Animal (2018)
-
Elevated peripheral expression of neuregulin-1 (NRG1) mRNA isoforms in clozapine-treated schizophrenia patients
Translational Psychiatry (2017)
-
Emerging roles of ARHGAP33 in intracellular trafficking of TrkB and pathophysiology of neuropsychiatric disorders
Nature Communications (2016)
-
Increased dysbindin-1B isoform expression in schizophrenia and its propensity in aggresome formation
Cell Discovery (2015)
