
Abstract
The objective of this systematic review was to assess tooth wear against ceramic crowns in posterior region in vitro and in vivo. An electronic PubMed search was conducted to identify studies on tooth wear against ceramic crowns in posterior region. The selected studies were analyzed in regard to type of crowns, natural antagonist, measuring protocol and outcome. From a yield of 1 000 titles, 43 articles were selected for full-text analysis; finally, no in vitro and only five in vivo studies met the inclusion criteria. As there is heterogeneity in design, used measuring method, ceramics and analysis-form, a meta-analysis was not possible. Results of these studies are very controversial which makes a scientifically valid comparison impossible. This review indicated that some all-ceramic crowns are as wear friendly as metal-ceramic crowns. Up to now, it has been impossible to associate tooth wear with any specific causal agent. The role of ceramic surface treatment that might be responsible for the changing in rate of tooth wear seems undetermined as yet through clinical trials. The literature reveals that studies on this topic are subject to a substantial amount of bias. Therefore, additional clinical studies, properly designed to diminish bias, are warranted.
Similar content being viewed by others

INTRODUCTION
Wear of tooth structure is a natural unavoidable process which occurs when tooth and tooth, or tooth and restoration are in contact and slide against each other. However, this natural process may be accelerated by the introduction of restorations whose properties of wear differ from those of the tooth structure that they slide against. It has been shown that enamel may be subject to accelerated wear when opposed by ceramic.1 Therefore and despite the truth that a constant wear of the entire dentition is possible independent of dental restorations,2 it is desirable that wear behavior of restorative materials is similar to natural enamel, because excessive wear could lead to clinical problems such as damage of teeth occluding surfaces, loss of vertical dimension of occlusion, poor masticatory function associated with temporomandibular joint remodeling, dentine hypersinsivity or death of the tooth and at least may lead to esthetic impairment.3,4,5
In the oral cavity, many factors contribute to the wear of enamel and dentin, such as the nature of the occlusal contacts with antagonist teeth (attrition), chewing of food items, tooth brushing with toothpaste, inhalation of dust (abrasion), acidic attack due to the consumption of certain fruits and beverages, inhalation of industrial acids or vomiting and regurgitation of gastric juice as in the case of bulimia and anorexia nervosa (corrosion).6
In order to observe and assess wear, it is necessary to understand tooth wear mechanisms and how it can be measured and evaluated, both clinically and in the laboratory. The terms abrasion, attrition and even corrosion were often used to identify the same thing which is the tooth wear caused mostly by alimentation and utilities use. Contrary, nowadays there is an agreement that the terms, abrasion, attrition and corrosion describe different mechanisms.
Attrition: tooth-to-tooth contact causes this form of wear, this occurs without the presence of food or foreign substances during deglutition and clenching; it is typically characterized by the facets on a tooth and the opposing tooth. It becomes more serious during bruxism.7
Abrasion: is the wear caused by friction between a tooth and an exogenous agent. The ‘masticatory abrasion’, usually occurs by friction from the food and abrasion, which is a result of bad oral habits such as nail biting or hard objects such as pens, pencils or pipes, opening hair pins with teeth. Occupational abrasion may occur among hairdressers because of opening hair pins with their teeth, tailors through cutting thread with their teeth, shoemakers who hold nails between their teeth and musicians who play wind instruments.
Tooth-cleaning, habits such as extreme tooth brushing, improper use of dental floss and toothpicks are the most common cause of abrasion. Even normal tooth-cleaning practices produce some abrasion of dentine over a lifetime. In Western populations, the major abrasive agent is toothpaste, which affects dentine much more than enamel.8 Tooth brushing without paste has no effect on enamel and clinically negligible effects on dentine.9
Corrosion: Is the loss of tooth surfaces caused by chemical dissolution without the involvement of plaque. Depending on the source of the acids causing the dissolution, there are two types of corrosion, intrinsic and extrinsic corrosion.10,11 The tooth corrosion caused by intrinsic sources such as bulimia and gastro esophageal reflux disease, shows enamel surfaces which appears to be translucent and thin; moreover bowel-shaped defects on the posterior occlusal surfaces and an enamel lost on the anterior palatal surfaces can be recognized. It has been reported that consuming drinks and food with a pH value of less than 5.5 can cause corrosion and demineralize teeth.10,11 Corrosive damage to anterior teeth may affect workers in industries where they are continuously exposed to acid droplets and fumes. Softened enamel exposed to saliva for an adequate time can regain mineral and thus re-acquire mechanical strength.12,13 On the other hand, it has been stated that fluoridated toothpaste had a protective effect on enamel corrosion progression.5,14,15,16,17,18,19,20
The observation of in vivo and in vitro studies show that individual wear mechanisms rarely act alone but interact with each other so that tooth wear is the result of three processes: abrasion, attrition and corrosion.
Measuring methods (wear quantification)
One of the most popular measuring methods of tooth wear is the direct measuring using clinical tooth wear indices;5,15,16,17,18,19,20 with this method, special equipment is not required, but the assessment is subjective and it takes a long time to get significant results.21 In addition, most tooth wear indices use unclear and complicated diagnostic criteria. Other limitations of these indices are no clear classification and quantification of tooth wear, besides the limited ability to determine the critical value of acceptable wear. Also, there are a lot of tooth wear index which make it difficult to achieve standardized and reliable tooth wear quantification and that leads to difficulties by comparing the results of various studies.
Indirect techniques for evaluation of tooth wear suggest measuring the loss of tooth surface using cast replicas.22,23,24,25 For more accurate quantification, image analysis, scanning electron microscopy,5,22,23,24,25,26,27 computer graphics,28 three dimensional (3D) scanner15,29,30 and profilometry5,31,32,33,34,35,36,37,38,39,40,41 were developed. Disadvantages can be inaccurate replicas and repositioning problems, due to the fact that reproducing of tooth surfaces with impressions before scanning always adds a source of error.23
Various clinical studies applied these 3D measuring techniques,5,22,24,25,30,42 which allow 3D scanning of the entire tooth surface without affecting the tooth surfaces. These techniques are highly accurate, quantitative, applicable to both the clinic and the laboratory, and provides storable 3D databases that enable comparison to other 3D databases.30,32
3D images can be obtained using contact profilers, non-contact white light, micro/cone computerized tomography (CT) scanners, laser scanners and computer-aided design/computer-aided manufacturing (CAD/CAM) systems such as Cerec and Cercon systems.15 However, 3D canning requires a specialized hardware and software and has the disadvantage of time-consuming, high cost and the limited availability to clinical investigators.24,43 Measurement accuracy of the cone-beam CT scanners approximates few hundred microns, and thus they have limited ability to determine tooth wear on the occlusal surfaces.44
Direct intraoral 3D scanning of teeth, e.g., intraoral digital camera of Cerec, is accurate and requires less number of steps when compared to the indirect scanning of models,43 but the need for spraying teeth with white powder might decrease the accuracy of measurement.
Clinical studies which evaluate dental wear are very time-consuming, expensive and have the disadvantage that a lot of factors such as chewing forces cannot be controlled.40 Thus, laboratory mastication simulation has been used by a lot of investigators to study single parameters of the wear processes.28,31,45,46,47,48,49 But even the in vitro wear simulations show considerable variability and do not simulate the clinical condition, because the loads, speeds and abrasives used are often more severe than the masticatory standards.50
Ceramic crowns opposing tooth structure
As mentioned before, wear of teeth differs according to the different restorative materials used as antagonist. Ceramic reconstructions have become increasingly popular as a result of rising patient demands for more aesthetics. But the main disadvantage of ceramics is their high abrasiveness to opposing enamel.51,52 Various types of ceramic crowns can be used as fixed dental prosthesis; some entirely made of the same ceramic material through out and others consist of high-strength ceramic substructure veneered with porcelain; in addition metal-ceramic crowns veneered with porcelain are still used.53 Recently, the high-strength zirconia ceramic (yttrium-oxide tetragonal zirconia polycrystal) was introduced for dental application; it has a high bending strength and fracture toughness.54 The clinical use of this ceramic is increasing because of its chemical and dimensional stability, its higher fracture toughness, hardness and frictional resistance in comparison to conventional dental porcelain.54,55,56 But the weak point of a zirconia restoration is at this time veneer chipping or cracking,57 whereas other all-ceramic restorations show a percentage of framework fracture.58,59
Using CAD/CAM techniques, it has become possible to produce full-zirconia restorations with occlusal design that do not need to be veneered (Zirluna; ACF GmbH, Amberg, Germany; Zirkonzahn Prettau; Zirkonzahn GmbH, Bruneck, Italy; BruxiZir; Glidewell Laboratories, Newport Beach, CA, USA); and must have the advantage that no chipping of the veneering porcelain will occur because of the absence of this veneering layer. Mono-block restorations could be also fabricated from glass ceramics; however, they are less stable in comparison to zirconia-based restorations and their indication range is clearly limited to single crowns and small fixed dental prostheses.53
Factors affecting enamel wear when opposed by ceramic
At this point of research, some of the features of ceramic which affect enamel wear were evaluated:
Hardness of ceramics was always associated with the greater abrasiveness against teeth,34,60 but some studies showed that the hardness of ceramics will not substantially lead to wear of the opposing teeth.61,62 On the other hand, the degree of wear is more affected by the surface structure and the roughness of the restoration or environmental factors.61,62 Various in vitro investigations on the effect of ceramic hardness on the dental wear have supported this fact by their finding that soft ceramics caused more abrasion against enamel (enamel abrasion) in comparison with harder ceramics.36,46
Similarly, more wear was expected from zirconia, because zirconia has strong surface hardness,56,63 but certain investigations reported that less wear of antagonistic teeth was measured with zirconia than with the feldspathic dental porcelain.64,65 Rosentritt has no wear traces for enamel against zirconia using a chewing simulation.65 It was also reported that the wear rate of zirconia is bad in water and even under dry sliding conditions,66 that suggests that the hardness of ceramics alone is not a reliable predictor of the wear of opposing teeth.
Resistance to friction: Many factors may affect the frictional resistance of the both teeth and ceramic restorations when coming together in contact, e.g., morphology, properties and structure of tooth and restoration, as well as mastication movements. With increased coefficient of friction, more wear of the tooth structure would be expected. It has been shown that high loads, rough surfaces and high sliding speed caused an increase in the coefficient of friction which leads to greater wear.67 Therefore, meticulously polished ceramic surfaces would lead to an decrease in the rates of wear of the opposing tooth surfaces.
Porosity: Undesirable characteristic of ceramic like decreased strength, reduced aesthetics and increased plaque accumulation can be impart by porosity.68 Furthermore, during the wear process, a subsurface porosity of ceramic may be exposed, then the sharp edge of the defect will cause increased wear in the opposing teeth;32,69,70 therefore, porosity of dental porcelain needs to be minimized.
Some parameters are associated with increased porosity of dental ceramics such as particle size,71 higher sintering temperature68 and longer sintering time.72 More porosity was showed in low-fusing porcelains with a fine grain size than in conventional feldspathic porcelain.36 It was also reported that aluminous porcelain has a higher viscosity than conventional feldspathic porcelain, which requires a higher firing temperature to increase the wetting of crystals and the glassy matrix73 and because of that, a higher porosity of aluminus porcelain is expected. Although a reduction of porosity is expected by longer sintering time,72 Piddock73 and Cheung68 reported an increase in porosity with increasing sintering time, because of the limited ability of air to escape during rapid firing. During the building of porcelain layers in order to simulate the teeth tissues, the influence of mechanical vibration on the reduction of porosity is limited.74
Full-zirconia restorations without veneering are free from the problems associated with porosity, because they have no veneer layer and their microstructure shows no open porosity.75
Effect of roughness of ceramic surfaces: The surface treatment of all ceramic crowns may be responsible for the changing in the rate of enamel wear. Glazing of ceramic restorations produces a smooth, aesthetic and hygienic surface and is considered as a step which reduces the amount of wear of opposing teeth and restorations, but this layer of glaze can be removed shortly after being in function or by a required occlusal adjustment76 that may lead to more abrasive wear of the opposing teeth because of the insufficiently polished exposed surface of the crown.
Jagger77 suggested in his study that the amounts of wear of enamel caused by glazed and unglazed porcelain are similar. Some investigators found that the glazed ceramic surfaces are smoother than the polished ones.78,79 However, other authors found no significant differences between glazed and polished ceramic surfaces.75,80,81 Contradictorily, some investigations confirmed the finding that the smoothness of polished ceramic surfaces is similar or better than the glazed surfaces.82,83,84,85 This conclusion was supported through various in vitro studies, which found that the glazed surfaces caused more teeth wear compared to polished surfaces.39,77,86 Functional finishing of ceramic surfaces during the wear process was documented by Monasky,87 who reported in his in vitro study that the initially high rate of wear decreased over time, suggesting that the effect of surface roughness on wear may be self-limiting.
However, it must be considered that the factors described above are results of in vitro studies depending on wear or chewing simulation device and these results are contradictory.
The aim of this manuscript was to provide a literature review about the tooth wear against ceramic crowns in posterior region both in vitro and in vivo. This systematic review was prepared following the preferred reporting items for systematic reviews and meta-analyses statement guidelines (http://www.prisma-statement.org/). This article focuses as well on measuring methods of tooth wear available in dental literature and on factors related to ceramic materials and may influence the wear of opposing tooth structure.
MATERIAL AND METHODS
Search strategy and study selection
An electronic PubMed search for in vitro and in vivo trials on tooth wear by ceramic crowns in posterior region was supplemented manually to obtain peer-reviewed articles published in English language till April 2013. The main keywords used for the search and the numbers of articles produced were:
-
tooth wear and in vitro 634;
-
tooth wear and in vivo 160;
-
tooth wear and ceramic crowns 138;
-
tooth wear and metal-ceramic crowns 48;
-
tooth wear and ceramic crowns and in vitro 9;
-
tooth wear and ceramic crowns and in vivo 4;
-
tooth wear and metal-ceramic crowns and in vitro 3;
-
tooth wear and metal-ceramic crowns and in vivo 4.
Titles and abstracts were initially screened by two reviewers for possible inclusion in the review. To decide about inclusion of the studies, full text of all studies of possible relevance was then obtained for assessment by the reviewers. To complement the search, a manual hand search of the bibliographies of all full-text articles and related reviews selected from the electronic search was also performed to identify any possible investigations on wear of natural teeth, which may have not been listed on PubMed.
The articles found (43 studies) were read to identify ones which satisfied the following inclusion and exclusion criteria.
Inclusion criteria
This systematic review is based on in vitro and in vivo (prospective or retrospective) cohort studies. Inclusion criteria for study selection were:
-
human in vivo and in vitro;
-
conducted on tooth wear by ceramic crowns;
-
study has a set inclusion and exclusion criteria;
-
study has a materials and methods;
-
publications appearing in English and in the Dental literature;
-
a mean follow-up time of 6 months or more for in vivo trials.
Exclusion criteria
-
case reports;
-
animal studies;
-
conducted on other ceramic restorations except of crowns;
-
use of flat specimens in vitro;
-
clinical trials with follow-up time of less than 6 months;
-
patients with bruxism.
The selected studies that met the inclusion criteria were analyzed with regard to type of crowns antagonist, wear measuring method, wear measuring device and outcome.
RESULTS
Because of the heterogeneity in design, used measuring method, used materials, forms of analysis and associated factors, a meta-analysis was not possible.
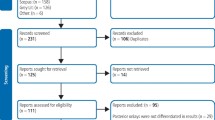
From a yield of 1 000 titles, 43 articles were selected for full-text analysis; finally, no in vitro and only five in vivo studies met the inclusion criteria.
From the 43 full-text articles retrieved, all of the 30 in vitro studies were excluded from the final analysis. The main reason for exclusion was the use of flat specimens against the natural teeth in vitro.
From this extensive search, it was obvious that there were no in vitro studies available measuring the tooth wear against ceramic crowns in posterior region. Following this, one final search was done by inspecting the bibliographies of the 43 reviewed articles for any additional studies; however, none were found. From the eligible investigations, five studies satisfied the inclusion criteria and were included in the systematic review. The characteristics of the selected studies are shown in Table 1.
These studies were published from 2008 to 2013. Full-text analysis of the five studies showed that the three studies performed by Silva 2011, Esquivel-Upshaw 2012 and Esquivel-Upshaw 2013 evaluated tooth wear by the same patient population and published the same obtained results in three different journals; therefore, we decided to consider the results of these three trials as the results of one investigation.
The studies included 79 patients between the age of 18 and 62 years. A total dropout of two patients were reported and excluded from the evaluation. The studies were mainly conducted in an institutional environment in universities. The operators were dental students, postgraduate students, private dentists and specialists.
The reviewed studies involved patients with teeth that needed full-coverage crowns in posterior region; only in one study,22 first premolars were included; otherwise, the other investigator included only second premolars, first and second molars. Patients showed no temporomandibular disorders or parafunctional habits (e.g., bruxism or clenching).
In all studies, crowns had to be opposed by natural dentition in the maxillary or mandibular arch, but in each study, this point was described in different way:
-
i)
Etman 2008: crowns had to be opposed by a natural tooth which the majority of the occlusal surface was enamel.
-
ii)
Suputtamongkol 2008: reported that treated teeth must be opposed by natural dentition in the maxillary and mandibular arch.
-
iii)
Silva 2011: the crown had to be opposed by antagonist tooth with intact enamel surfaces.
-
iv)
Esquivel-Upshaw 2012: the crown must be opposed by a natural antagonist.
-
v)
Esquivel-Upshaw 2013: crown must have an opposing non-restored or minimally restored natural teeth (i.e., not larger than a Class II amalgam restoration).
The studies included a total of 156 crowns. Forty-two metal-ceramic crowns and 114 all-ceramic crowns were tested. The evaluated crown systems and the measuring methods used are summarized in Table 2.
Metal-ceramic crowns
Etman 2008 measured tooth wear against 30 metal-ceramic crowns made using Simidur S 2 alloy (Panadent, Colton, CA, USA) as a coping material that was veneered using IPS Classic feldspathic porcelain (Ivoclar Vivadent, Schaan, Lichtenstein). The three studies Silva 2011, Esquivel-Upshaw 2012 and Esquivel-Upshaw 2013, used 12 metal-ceramic crown system: crowns were made from Pd–Au–Ag–Sn–In alloy (Argedent 62; Argen Corporation, San Diego, CA, USA) and glass-ceramic as veneer (IPS d.SIGN veneer; Ivoclar Vivadent, Schaan, Liechtenstein).
All-ceramic crowns
Suputtamongkel investigated 30 crowns made of lithium disilicate-based all-ceramic system (Ivoclar Vivadent, Schaan, Liechtenstein). The veneering material that opposed the enamel was glass-based, but the author did not mention which material was used.
In his trial, Etman 2008 tested two types of all-ceramic crowns:
-
i)
30 IPS e.max Press crowns/lithium disilicate crystals (Ivoclar Vivadent);
-
ii)
The other 30 crowns were made using ProceraAllCeram coping (Nobel Biocare, Zürich, Switzerland) veneered with feldspathic porcelain (Ducera, Berlin, Germany).
The three studies Silva 2011, Esquivel-Upshaw 2012 and Esquivel-Upshaw 2013, used two all-ceramic crown systems:
-
i)
Non-veneered (glazed) crowns made from a lithium disilicate glass-ceramic (IPS e.max Press core and e.max Ceram glaze; Ivoclar Vivadent, Schaan, Liechtenstein).
-
ii)
Core ceramic/veneer ceramic crowns made from lithium disilicate glass-ceramic and a glass ceramic veneer (IPS Empress 2 core and IPS Eris; Ivoclar Vivadent, Schaan, Liechtenstein).
The follow-up time ranged from 6 months to 3 years. Baseline impressions were made 1 week after crowns cementation.
The tooth wear results obtained in the reviewed investigations are listed in Table 3. The highest tooth wear was reported after 24 months for the patients who received Procera AllCeram crowns and the lowest tooth wear was against metal-ceramic crowns veneered with IPs classic.
DISCUSSION
This review was performed to evaluate available information in the dental literature on tooth wear against ceramic crowns in posterior region both in vitro and in vivo. The first idea was to see whether there were any clinical prospective studies supporting the findings of in vitro studies that showed how wear friendly the ceramic materials are. Surprisingly, we observed that there are no in vitro studies measured tooth wear against ceramic crowns in posterior region. Further intensive search yielded no in vitro investigation focusing on the evaluation of the effect of anatomical occlusal surfaces on tooth wear process. Available in vitro investigations mostly measured tooth wear against flat-shaped ceramic specimens33,36,46,65 and that made a comparison of in vitro results with those of in vivo trials impossible. Therefore and based on the available literature, we decided to present an overview of the current thinking on the relationship of clinical tooth wear and the ceramic crowns in posterior region.
Only five in vivo studies dealt with establishing a causal relationship between insertion of ceramic crowns and increased tooth wear in posterior region. Detailed full-text analysis of these five studies revealed that in three of them (Silva 2011, Esquivel-Upshaw 2012, Esquivel-Upshaw 2013), the authors made the same investigation and evaluated the same patient population. Due to that, we had to consider the results of these three studies as results of one investigation and to compare it with the other two studies of Etman 2008, Suputtamongkol 2008.
To measure the amount of worn dental tissues after cementing the crowns, impressions were made of each of the maxillary and mandibular arches at 1 week (baseline) and after 6 months,22,88,89,90 1 year,22,25,88,89,90 2 years22,88,89,90 and 3 years.88,89,90 Resulting gypsum casts were produced by a dental technician with type IV gypsum (GC Fujirock, Leuven, Belgium) and scanned using the same 3D laser scanner (es1 Scanner; Etkon, Gräfelfing, Germany).25,88,89,90 In one study,22 the quantitative measurement of wear was performed by digitizing the impressions of the restored teeth and their antagonist using a non-contacting laser profilometer (Keyence LC-2400 series laser displacement meter). The use of different methods in obtaining wear data may account for such a broad range (Table 3) between the results of this study22 and the results of the other studies.25,88,89,90
Etman 2008 reported in his investigation that the metal-crowns produced the least tooth wear and the Procera AllCeram veneered with feldspathic porcelain (Ducera) was the most abrasive ceramic which caused more tooth wear than the metal-ceramic (Simidur alloy veneered with IPS Classic) and the other experimental glass-ceramic (IPS Empress/lost wax technique); it also suffered the greatest loss of test material. Contrary Silva 2011 results showed that the metal-ceramic crowns (Argendent alloy veneered with IPS.d.SIGN) caused the highest tooth wear volume compared to the other tested all-ceramic crowns (IPS Empress 2 veneered IPS Eris and the other all-ceramic system IPS e.max Press without veneering). The natural teeth opposing these crowns exhibited at year 3 wear as follows: (1.10±0.10) mm3 for metal-ceramic crowns/IPS d.SIGN; (1.02±0.20) mm3 for IPS Eris for E2 and (0.80±0.09) mm3 for IPS e.max Press. We can recognize that crowns made using the system IPS. e.max Press were the most wear friendly after 3 years.
The use of two different measuring methods in these two studies (Etman 2008 and Silva 2011) may explain these two different statements. Moreover, the results by Etman 2008 were obtained after 2 years and by Saliva 2011 after 3 years. And at least we must mention that the veneering ceramics used were different and each investigator compared metal-ceramic crowns with different all-ceramic systems.
Volume of tooth wear measured by Suputtamongkol 200825 against lithiadiasilicate-based all ceramic crowns and after 1 year, was less than that measured by Silva 201188 against lithiadisilicate all-ceramic crowns after three years (Table 3). This comparison may lead to the conclusion that tooth wear increased with time.
This article addressed some of the material factors related to the wear of opposing enamel by ceramic. It can be concluded that hardness of ceramics should not be blamed for the accelerated loss of enamel as various studies have demonstrated that there is no strong correlation between the ceramic hardness and the wear rate of human enamel;61,62 however, it was confirmed that wear process would be more affected by ceramic microstructure and ceramic roughness and therefore, surface treatment of ceramics played a significant role on wear of opposing tooth structure.36,46,48 Etman 2008 confirmed that in his clinical trial, low-fusing porcelain used to veneer Procera AllCeram copings caused the highest tooth wear. Various in vitro investigations on the effect of ceramic hardness on the dental wear have supported this fact by their finding that soft ceramics caused more abrasion against enamel in comparison with harder.36,48
Roughened and pitted surfaces of the feldspathic porcelain were detected by clinical and by scanning electron microscope examination;90 as a result, exposure of the crystalline structure happened and thus. will accelerate the rates of tooth wear in the future.
There was no significant relationship between bite force and tooth wear through the first year25,89 and the second year;90 however, there was a significant effect of bite force on wear at year 3 when enamel contralateral antagonist was analyzed alone.90 That confirms the truth that a constant wear of the entire dentition is possible independent of dental restorations.2
As clinical recommendations demand perfectly polished surfaces of all ceramic restorations after any occlusal adjustments, the maintenance of a smooth ceramic surface during clinical use is the key for avoiding initiation or progression of microcracks and for minimizing abrasion of the opposing teeth. Nevertheless, it would be difficult to find an answer about the optimal ceramic treatment that is not responsible for accelerated enamel wear. That is because of the inconsistent results of various studies that were performed to identify the best techniques to achieve a smooth ceramic surface. It can be assumed that when enamel is opposed by unglazed and unpolished ceramic surface, the wear rate of enamel is higher than when opposed by glazed or polished one.36,85
It can be suggested that dentists should consider the type of ceramic restorative material used. Further, the ceramic restorations should be sufficiently polished after any chairside adjustment of occlusal surface so that it minimizes the undesired effect of roughened ceramic materials on wear of antagonistic tooth. Wear requires the sliding of one surface against the other; therefore, when a ceramic restoration is placed, sliding contact in centric and eccentric movements should be minimized.
The literature reveals that studies on this topic are subject to a substantial amount of bias, such as evaluation bias (use of non-blinded examiners) and confounding bias (no control of other aethiological factors). Up to now, it has been impossible to associate tooth wear with any specific causal agent, and the role of surface treatment of ceramic crowns that may be responsible for the changing in the rate of enamel wear seems as yet undetermined. Therefore, additional studies, properly designed to diminish bias, are warranted.
Based on the applied literature, it can be concluded that for ceramic material, their proper handling and control of the patient’s intrinsic risk factors related to wear are all critically important to the reduction of enamel wear by dental ceramics.
References
Wiley MG . Effects of porcelain on occluding surfaces of restored teeth. J Prosthet Dent 1989; 61( 2): 133–137.
Sulong MZ, Aziz RA . Wear of materials used in dentistry: a review of the literature. J Prosthet Dent 1990; 63( 3): 342–349.
Bani D, Bani T, Bergamini M . Morphologic and biochemical changes of the masseter muscles induced by occlusal wear: studies in a rat model. J Dent Res 1999; 78( 11): 1735–1744.
Oh WS, Delong R, Anusavice KJ . Factors affecting enamel and ceramic wear: a literature review. J Prosthet Dent 2002; 87( 4): 451–459.
Ohlmann B, Trame JP, Dreyhaupt J et al. Wear of posterior metal-free polymer crowns after 2 years. J Oral Rehabil 2008; 35( 10): 782–788.
Smith BG, Bartlett DW, Robb ND . The prevalence, etiology and management of tooth wear in the United Kingdom. J Prosthet Dent 1997; 78( 4): 367–372.
Xhonga FA . Bruxism and its effect on the teeth. J Oral Rehabil 1977; 4( 1): 65–76.
Addy M, Hunter ML . Can tooth brushing damage your health? Effects on oral and dental tissues. Int Dent J 2003; 53( Suppl 3): 177–186.
Absi EG, Addy M, Adams D . Dentine hypersensitivity - the effect of toothbrushing and dietary compounds on dentine in vitro: an SEM study. J Oral Rehabil 1992; 19: 101–110.
Huysmans MC, Chew HP, Ellwood RP . Clinical studies of dental erosion and erosive wear. Caries Res 2011; 45( Suppl 1): 60–68.
Lussi A, Schlueter N, Rakhmatullina E et al. Dental erosion—an overview with emphasis on chemical and histopathological aspects. Caries Res 2011; 45( Suppl 1): 2–12.
Attin T, Buchalla W, Gollner M et al. Use of variable remineralization periods to improve the abrasion resistance of previously eroded enamel. Caries Res 2000; 34( 1): 48–52.
Eisenburger M, Addy M, Hughes JA et al. Effect of time on the remineralisation of enamel by synthetic saliva after citric acid erosion. Caries Res 2001; 35( 3): 211–215.
Ganss C, Klimek J, Schaffer U et al. Effectiveness of two fluoridation measures on erosion progression in human enamel and dentine in vitro. Caries Res 2001; 35( 5): 325–330.
Al-Omiri MK, Harb R, Abu Hammad OA et al. Quantification of tooth wear: conventional vs new method using toolmakers microscope and a three-dimensional measuring technique. J Dent 2010; 38( 7): 560–568.
Carlsson GE, Johansson A, Lundqvist S . Occlusal wear. A follow-up study of 18 subjects with extensively worn dentitions. Acta Odontol Scand 1985; 43( 2): 83–90.
Chadwick RG, McCabe JF, Walls AW et al. Comparison of a novel photogrammetric technique and modified USPHS criteria to monitor the wear of restorations. J Dent 1991; 19( 1): 39–45.
Fares J, Shirodaria S, Chiu K et al. A new index of tooth wear. Reproducibility and application to a sample of 18- to 30-year-old university students. Caries Res 2009; 43( 2): 119–125.
Hugoson A, Bergendal T, Ekfeldt A et al. Prevalence and severity of incisal and occlusal tooth wear in an adult Swedish population. Acta Odontol Scand 1988; 46( 5): 255–265.
Oilo G, Dahl BL, Hatle G et al. An index for evaluating wear of teeth. Acta Odontol Scand 1987; 45( 5): 361–365.
Taylor DF, Bayne SC, Sturdevant JR et al. Correlation of M–L, Leinfelder, and USPHS clinical evaluation techniques for wear. Dent Mater 1990; 6( 3): 151–153.
Etman MK, Woolford M, Dunne S . Quantitative measurement of tooth and ceramic wear: in vivo study. Int J Prosthodont 2008; 21( 3): 245–252.
Lambrechts P, Braem M, Vuylsteke-Wauters M et al. Quantitative in vivo wear of human enamel. J Dent Res 1989; 68( 12): 1752–1754.
Peters MC, Delong R, Pintado MR et al. Comparison of two measurement techniques for clinical wear. J Dent 1999; 27( 7): 479–485.
Suputtamongkol K, Anusavice KJ, Suchatlampong C et al. Clinical performance and wear characteristics of veneered lithia-disilicate-based ceramic crowns. Dent Mater 2008; 24( 5): 667–673.
Teaford MF, Tylenda CA . A new approach to the study of tooth wear. J Dent Res 1991; 70( 3): 204–207.
Willems G, Lambrechts P, Lesaffre E et al. Three-year follow-up of five posterior composites: SEM study of differential wear. J Dent 1993; 21( 2): 79–86.
DeLong R, Sasik C, Pintado MR et al. The wear of enamel when opposed by ceramic systems. Dent Mater 1989; 5( 4): 266–271.
Albashaireh ZS, Ghazal M, Kern M . Two-body wear of different ceramic materials opposed to zirconia ceramic. J Prosthet Dent 2010; 104( 2): 105–113.
Mehl A, Gloger W, Kunzelmann KH et al. A new optical 3-D device for the detection of wear. J Dent Res 1997; 76( 11): 1799–1807.
Alarcon JV, Engelmeier RL, Powers JM et al. Wear testing of composite, gold, porcelain, and enamel opposing a removable cobalt–chromium partial denture alloy. J Prosthodont 2009; 18( 5): 421–426.
Delong R, Pintado MR, Douglas WH . The wear of enamel opposing shaded ceramic restorative materials: an in vitro study. J Prosthet Dent 1992; 68( 1): 42–48.
Elmaria A, Goldstein G, Vijayaraghavan T et al. An evaluation of wear when enamel is opposed by various ceramic materials and gold. J Prosthet Dent 2006; 96( 5): 345–353.
Hudson JD, Goldstein GR, Georgescu M . Enamel wear caused by three different restorative materials. J Prosthet Dent 1995; 74( 6): 647–654.
Joshi N, Patil NP, Patil SB . The abrasive effect of a porcelain and a nickel–chromium alloy on the wear of human enamel and the influence of a carbonated beverage on the rate of wear. J Prosthodont 2010; 19( 3): 212–217.
Magne P, Oh WS, Pintado MR et al. Wear of enamel and veneering ceramics after laboratory and chairside finishing procedures. J Prosthet Dent 1999; 82( 6): 669–679.
Metzler KT, Woody RD, Miller AW 3 rd et al. In vitro investigation of the wear of human enamel by dental porcelain. J Prosthet Dent 1999; 81( 3): 356–364.
O’Kray HP, O’Brien WJ . In vitro human enamel wear by a hydrated high-alkali porcelain. Quintessence Int 2005; 36( 8): 617–622.
Palmer DS, Barco MT, Pelleu GB Jr et al. Wear of human enamel against a commercial castable ceramic restorative material. J Prosthet Dent 1991; 65( 2): 192–195.
Pintado MR, Anderson GC, DeLong R et al. Variation in tooth wear in young adults over a two-year period. J Prosthet Dent 1997; 77( 3): 313–320.
Yu H, Wegehaupt FJ, Wiegand A et al. Erosion and abrasion of tooth-colored restorative materials and human enamel. J Dent 2009; 37( 12): 913–922.
Esquivel-Upshaw JF, Young H, Jones J et al. In vivo wear of enamel by a lithia disilicate-based core ceramic used for posterior fixed partial dentures: first-year results. Int J Prosthodont 2006; 19( 4): 391–396.
DeLong R . Intra-oral restorative materials wear: rethinking the current approaches: how to measure wear. Dent Mater 2006; 22( 8): 702–711.
Kobayashi K, Shimoda S, Nakagawa Y et al. Accuracy in measurement of distance using limited cone-beam computerized tomography. Int J Oral Maxillofac Implants 2004; 19( 2): 228–231.
Sirona Dental Systems, Inc. Electronical material cerec omnicam and cerec bluecam. The first choice in every case. Sirona product information. Available at http://www.sirona.com/de/aktuelles/kampagnen/die-neue-cerec-omnicam/ (accessed 31 October 2012).
al-Hiyasat AS, Saunders WP, Sharkey SW et al. Investigation of human enamel wear against four dental ceramics and gold. J Dent 1998; 26( 5/6): 487–495.
al-Hiyasat AS, Saunders WP, Smith GM . Three-body wear associated with three ceramics and enamel. J Prosthet Dent 1999; 82( 4): 476–481.
Clelland NL, Agarwala V, Knobloch LA et al. Wear of enamel opposing low-fusing and conventional ceramic restorative materials. J Prosthodont 2001; 10( 1): 8–15.
Hacker CH, Wagner WC, Razzoog ME . An in vitro investigation of the wear of enamel on porcelain and gold in saliva. J Prosthet Dent 1996; 75( 1): 14–17.
Rosentritt M, Hmaidouch R, Behr M et al. Fracture resistance of zirconia FPDs with adhesive bonding versus conventional cementation. Int J Prosthodont 2011; 24( 2): 168–171.
Heintze SD . How to qualify and validate wear simulation devices and methods. Dent Mater 2006; 22( 8): 712–734.
Cattell MJ, Clarke RL, Lynch EJ . The biaxial flexural strength and reliability of four dental ceramics—Part II. J Dent 1997; 25( 5): 409–414.
Zarone F, Russo S, Sorrentino R . From porcelain-fused-to-metal to zirconia: clinical and experimental considerations. Dent Mater 2011; 27( 1): 83–96.
Scherrer SS, de Rijk WG, Belser UC . Fracture resistance of human enamel and three all-ceramic crown systems on extracted teeth. Int J Prosthodont 1996; 9( 6): 580–585.
Aboushelib MN, de Jager N, Kleverlaan CJ et al. Microtensile bond strength of different components of core veneered all-ceramic restorations. Dent Mater 2005; 21( 10): 984–991.
Sundh A, Sjogren G . Fracture resistance of all-ceramic zirconia bridges with differing phase stabilizers and quality of sintering. Dent Mater 2006; 22( 8): 778–784.
Raigrodski AJ, Chiche GJ, Potiket N et al. The efficacy of posterior three-unit zirconium-oxide-based ceramic fixed partial dental prostheses: a prospective clinical pilot study. J Prosthet Dent 2006; 96( 4): 237–244.
Esquivel-Upshaw JF, Anusavice KJ, Young H et al. Clinical performance of a lithia disilicate-based core ceramic for three-unit posterior FPDs. Int J Prosthodont 2004; 17( 4): 469–475.
Wolfart S, Bohlsen F, Wegner SM et al. A preliminary prospective evaluation of all-ceramic crown-retained and inlay-retained fixed partial dentures. Int J Prosthodont 2005; 18( 6): 497–505.
Fisher RM, Moore BK, Swartz ML et al. The effects of enamel wear on the metal-porcelain interface. J Prosthet Dent 1983; 50( 5): 627–631.
Dahl BL, Oilo G . In vivo wear ranking of some restorative materials. Quintessence Int 1994; 25( 8): 561–565.
Seghi RR, Rosenstiel SF, Bauer P . Abrasion of human enamel by different dental ceramics in vitro. J Dent Res 1991; 70( 3): 221–225.
Aboushelib MN, de Jager N, Kleverlaan CJ et al. Effect of loading method on the fracture mechanics of two layered all-ceramic restorative systems. Dent Mater 2007; 23( 8): 952–959.
Guazzato M, Albakry M, Ringer SP et al. Strength, fracture toughness and microstructure of a selection of all-ceramic materials. Part II. Zirconia-based dental ceramics. Dent Mater 2004; 20( 5): 449–456.
Jung YS, Lee JW, Choi YJ et al. A study on the in-vitro wear of the natural tooth structure by opposing zirconia or dental porcelain. J Adv Prosthodont 2010; 2( 3): 111–115.
Rosentritt M, Preis V, Behr M et al. Two-body wear of dental porcelain and substructure oxide ceramics. Clin Oral Investig 2012; 16( 3): 935–943.
Koran A, Craig RG, Tillitson EW . Coefficient of friction of prosthetic tooth materials. J Prosthet Dent 1972; 27( 3): 269–274.
Cheung KC, Darvell BW . Sintering of dental porcelain: effect of time and temperature on appearance and porosity. Dent Mater 2002; 18( 2): 163–173.
DeLong R, Douglas WH, Sakaguchi RL et al. The wear of dental porcelain in an artificial mouth. Dent Mater 1986; 2( 5): 214–219.
Kelly JR, Campbell SD, Bowen HK . Fracture-surface analysis of dental ceramics. J Prosthet Dent 1989; 62( 5): 536–541.
Rasmussen ST, Ngaji-Okumu W, Boenke K et al. Optimum particle size distribution for reduced sintering shrinkage of a dental porcelain. Dent Mater 1997; 13( 1): 43–50.
Anusavice KJ, Lee RB . Effect of firing temperature and water exposure on crack propagation in unglazed porcelain. J Dent Res 1989; 68( 6): 1075–1081.
Piddock V . Effect of alumina concentration on the thermal diffusivity of dental porcelain. J Dent 1989; 17( 6): 290–294.
Evans DB, Barghi N, Malloy CM et al. The influence of condensation method on porosity and shade of body porcelain. J Prosthet Dent 1990; 63( 4): 380–389.
Centre AAC . Zirluna (translucent) data sheet. Amberg: Centre AAC, 2010.
Brewer JD, Garlapo DA, Chipps EA et al. Clinical discrimination between autoglazed and polished porcelain surfaces. J Prosthet Dent 1990; 64( 6): 631–634.
Jagger DC, Harrison A . An in vitro investigation into the wear effects of unglazed, glazed, and polished porcelain on human enamel. J Prosthet Dent 1994; 72( 3): 320–323.
Campbell SD . Evaluation of surface roughness and polishing techniques for new ceramic materials. J Prosthet Dent 1989; 61( 5): 563–568.
Patterson CJ, McLundie AC, Stirrups DR et al. Efficacy of a porcelain refinishing system in restoring surface finish after grinding with fine and extra-fine diamond burs. J Prosthet Dent 1992; 68( 3): 402–406.
Grieve AR, Jeffrey IW, Sharma SJ . An evaluation of three methods of polishing porcelain by comparison of surface topography with the original glaze. Restorative Dent 1991; 7( 2): 34–36.
Sulik WD, Plekavich EJ . Surface finishing of dental porcelain. J Prosthet Dent 1981; 46( 2): 217–221.
Haywood VB, Heymann HO, Kusy RP et al. Polishing porcelain veneers: an SEM and specular reflectance analysis. Dent Mater 1988; 4( 3): 116–121.
Haywood VB, Heymann HO, Scurria MS . Effects of water, speed, and experimental instrumentation on finishing and polishing porcelain intra-orally. Dent Mater 1989; 5( 3): 185–188.
Scurria MS, Powers JM . Surface roughness of two polished ceramic materials. J Prosthet Dent 1994; 71( 2): 174–177.
al-Hiyasat AS, Saunders WP, Sharkey SW et al. The abrasive effect of glazed, unglazed, and polished porcelain on the wear of human enamel, and the influence of carbonated soft drinks on the rate of wear. Int J Prosthodont 1997; 10( 3): 269–282.
Jacobi R, Shillingburg HT Jr, Duncanson MG Jr . A comparison of the abrasiveness of six ceramic surfaces and gold. J Prosthet Dent 1991; 66( 3): 303–309.
Monasky GE, Taylor DF . Studies on the wear of porcelain, enamel, and gold. J Prosthet Dent 1971; 25( 3): 299–306.
Silva NR, Thompson VP, Valverde GB et al. Comparative reliability analyses of zirconium oxide and lithium disilicate restorations in vitro and in vivo. J Am Dent Assoc 2011; 142( Suppl 2): 4S–9S.
Esquivel-Upshaw JF, Rose WF Jr, Barrett AA et al. Three years in vivo wear: core-ceramic, veneers, and enamel antagonists. Dent Mater 2012; 28( 6): 615–621.
Esquivel-Upshaw J, Rose W, Oliveira E et al. Randomized, controlled clinical trial of bilayer ceramic and metal-ceramic crown performance. J Prosthodont 2013; 22( 3): 166–173.
Acknowledgements
Publication of this manuscript is supported by Open Fund of State Key Laboratory of Oral Diseases, Sichuan University.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-No Derivative Works 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Hmaidouch, R., Weigl, P. Tooth wear against ceramic crowns in posterior region: a systematic literature review. Int J Oral Sci 5, 183–190 (2013). https://doi.org/10.1038/ijos.2013.73
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijos.2013.73
Keywords
This article is cited by
-
Erosive tooth wear among non-institutionalised older adults in Hong Kong: a cross-sectional study
BMC Oral Health (2024)
-
Digital technique to analyze the wear of screw-retained implant supported metal-ceramic dental prostheses and natural tooth as antagonist: a pilot study
BMC Oral Health (2024)
-
Clinical and radiographic performance of preformed zirconia crowns and stainless-steel crowns in permanent first molars: 18-month results of a prospective, randomized trial
BMC Oral Health (2023)
-
Quantitative analysis on the wear of monolithic zirconia crowns on antagonist teeth
BMC Oral Health (2021)
-
In-vivo-wear in composite and ceramic full mouth rehabilitations over 3 years
Scientific Reports (2021)
