
Abstract
We compared values of body mass index (BMI) and cardiorespiratory fitness (20 m shuttle-run test) of n=157 boys and n=150 girls aged 10–11 measured in 2014 with measures from 2008 and 1998. Boys’ fitness was lower (d=0.68) in 2014 than 2008, despite a small (d=0.37) decline in BMI. Girl’s BMI changed trivially (d=0.08) but cardiorespiratory fitness was lower (d=0.47) in 2014 than 2008. This study suggests fitness is declining at 0.95% per year, which exceeds the 0.8% rate of decline we reported between 1998 and 2008 and is double the global average of 0.43%. Declines in fitness were independent of changes in BMI suggesting continued reductions in English children’s habitual physical activity levels.
Similar content being viewed by others
Introduction
Cardiorespiratory fitness is an important marker of childhood1 and adult2 health, but is declining globally at 4.3% a decade.3 Increases in body mass index (BMI) may explain some of the decrease in fitness4, 5 but we reported an 8% fall between 1998 and 2008 which was largely independent of changes in BMI.6 The prevalence of overweight and obesity is static or may even be declining in some English children.7 There are, however, no comparable data regarding English children’s cardiorespiratory fitness, despite a call for its surveillance by the Chief Medical Officer in 2009.8 We sought to determine whether cardiorespiratory fitness has changed since 2008 via a further secular comparison of data from 10–11-year olds from Chelmsford, England.
Materials and Methods
Study design
To update the Chelmsford Children’s Fitness and Activity Survey data, we approached all (n=5) schools surveyed in 2008. Four schools volunteered to participate again, including one from a more-deprived area we recruited purposefully in 2008 from within this relative affluent borough. As one school was unable to participate, we approached a neighbouring school (surveyed in 1998) which agreed to participate. Area-level deprivation was initially assessed using the English Indices of Deprivation9 obtained from school postcodes. In participating schools we assessed deprivation by the same method using pupils’ home postcodes.
We tested children in the summer term of 2014 to reduce potential seasonal bias. As before, testing was completed in school gymnasia and playgrounds. Ethical approval was granted by the Writtle College Ethics Committee and we obtained school and parental consent, as well as pupil assent prior to assessments.
Sample size calculation
The primary outcome measure was cardiorespiratory fitness assessed by performance on the 20 m shuttle-run test. Using extant means (±s.d.) we assumed a drop of 0.5 km h−1 over the 6-year period in boys and 0.4 km h−1 in girls. We calculated that n=140 boys and n=120 girls were needed to produce statistical significance at α=0.05 and β=0.80 assuming this predicted difference in test performance.
We repeated all measures using identical protocols to those reported previously.10 Stature (to the nearest 0.1 cm) and mass (to 0.1 kg) were measured with participants dressed in standard physical education clothing, without shoes. BMI was calculated (kg m−2) and converted to z-scores using UK reference data11 to correct for age, sex and skewness. Cardiorespiratory fitness (fitness) was assessed using the 20 m shuttle-run test. After listening to recorded instructions, pupils ran back and forth between cones (20 m apart) on flat, non-slip surfaces. Pupils ran in time with an audible signal, the initial running speed of 8 km h−1 increased by 1 km h−1 at the end of the first minute, then by 0.5 km h−1 after each consequent minute. Pupils were instructed to 'run as long as possible' and the test was terminated if individuals volitionally withdrew or when they could no-longer reach the cones in time on two consecutive occasions. Researchers recorded the number of shuttles completed which we converted to maximal running speed (km h−1) and z-scores based on global reference data.3
Data analysis
We analysed data from boys and girls separately using ANOVA to examine differences in BMI and fitness (z-scores). When analysing running speed, we checked data were normally distributed and then controlled for decimal age using analysis of covariance (ANCOVA) with Bonferroni post hoc tests. We calculated the intraclass correlation coefficient (ICC=between-school variance/(between-school variance+within-school variance)) to assess whether outcomes clustered within schools (low ICC (close to 0)=no/little clustering; high ICC (close to 1)=most/all variance is explained by clustering). We calculated standardised effect sizes (Cohen’s d) to describe the magnitude of differences between values obtained in 2008 and 2014; assuming a minimum important effect size of d=0.2.12 All analyses were performed in SPSS version 20 (SPSS, An IBM Company, Chicago, IL, USA).
Results
Table 1 shows BMI and fitness values from: 1998, 2008 and 2014. As differences between 1998 and 2008 have been reported previously, the following results focus on differences between 2008 and 2014.
Changes in BMI and fitness: boys
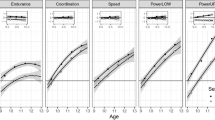
ANOVA showed no statistically significant main effect of time for boy’s BMI which was lower (z=−0.50, 95% CI, −1.2 to 0.24) in 2014 than in 2008 (d=0.38). ANCOVA showed a main effect for time on boys’ running speed and significant post hoc differences between all cohorts. There was a moderate (d=0.68) difference in boys’ running speed which was −0.87 (95% CI, −0.57 to −1.12) km h−1 slower in 2008 than 2014. There was a main effect of time for fitness (z-score) in boys, (Figure 1). Boy’s fitness was z=−0.67 (95% CI, −0.82 to −0.46) lower in 2008 than 2014 (d=0.64).

BMI and cardiorespiratory fitness (20 m shuttle-run test) of 10–11-year old schoolchildren: 1998, 2008 and 2014. All values are age- and sex-normalised z-scores. Z-scores calculated using the 1990 UK Growth Reference. Fitness—cardiorespiratory fitness assessed as maximal running speed achieved on the 20 m shuttle-run test and converted to z-scores using global reference data.5
Changes BMI and fitness: girls
There was no significant main effect for time on girls’ BMI (z-score) and a trivial (d=0.08) difference in mean values between 2008 and 2014. There was, however, a significant main effect for time on girls’ running speed, which declined by −0.34, (95% CI, −0.56 to −0.13) km h−1 from 2008 to 2014 (d=0.47). Girls’ fitness (z-score) was also (z=−0.51; 95% CI, −0.43 to −0.28) lower in 2014 than 2008 (d=0.57).
Subgroup analysis: changes BMI and fitness in children from more-deprived school
There was some evidence between-school clustering of fitness in 2008. Boys’ and girls’ fitness (z-scores) were lower in 2008, but between 2008 and 2014 the change in deprived boys; fitness was smaller (d=0.20) and there was a trivial increase (d=0.14) in deprived girls’ fitness.
Discussion
We reported annual declines of 0.7% and 0.9% in the cardiorespiratory fitness of boys and girls (respectively), in children from this area between 1998 and 2008.6 Chelmsford, like other affluent areas,13 did not witness overt increases in children’s BMI, despite reports of a ‘national’ obesity epidemic. As our primary aim was to provide an update from to our 2008 findings, this discussion is limited to the differences in measures of BMI and fitness from 2008 to 2014.
The lower mean value for BMI (z-scores) observed in boys measured in 2014 than in 2008 (d=0.37) indicates reduced adiposity; which is commonly associated with better performance on weight-bearing fitness tests like the 20 m shuttle-run.4 Despite potentially favourable changes in body composition, boys’ running speed was 8.3% lower in 2014 than in 2008; equivalent to a decline of 1.4% per year. This annual decline is double the figure reported between 1998 and 2008 (0.7%) which did coincide with a small increase in BMI.6 There was little change in girls’ BMI values, but their maximum running speed was 3.9% lower in 2014 than in 2008. This 0.65% annual rate of decline is lower than the 0.9% reported between 1998 and 2008.
The global rate of decline in fitness based on maximum running speed of both sexes is 0.43%, but we reported a much higher (0.8%) annual rate between 1998 and 2008. Combining data for both sexes suggests the rate of decline between 2008 and 2014 was 0.95% per year; greater still than over the previous 10-years and more than double the global average. Levels of fitness and changes in fitness differed greatly between sexes and to a lesser extent, between schools.
Inspection of mean values by school showed modest clustering of fitness (ICC=0.13) partly due to more-deprived children’s lower fitness values (Table 1). Such clustering was less obvious in 2014 (ICC=0.016). The change in more-deprived boys’ fitness was much smaller (d=0.20) than in the remaining population (d=0.96). The (albeit trivial, d=0.14) increase in fitness of more-deprived girls) was greatly at odds with the larger (d=0.69) decrease in fitness of the girls from less-deprived schools. Although intriguing, these findings should be interpreted with caution as this was an unplanned analysis in a small sample.
Historical declines in fitness may have been partly due to concomitant increases in body mass.4, 5, 14 Support for this hypothesis was elegantly provided in the SportsLinx project4 which reported declines in shuttle-run performance concurrent with increases in BMI. The current study is comparable to SportsLinx in design, but the findings differ greatly. Girls’ BMI (z-scores) changed little (d=0.08) but boys’ BMI was actually lower (d=0.37) in 2014 than 2008. Despite such potentially favourable changes in BMI, both boys and girls measured in 2014 performed less well on our weight-bearing fitness test compared with our age-matched sample from 2008.
The lower mean values for BMI are welcome and concur with national data showing a plateau6 or small decrease in the adiposity of children, from more-affluent areas at least.7 Our findings cannot explain the changes in BMI, but the lower fitness of children measured in 2014 than 2008 suggests continuing declines in their habitual physical activity. This theory is also supported by national survey data showing continued declines in calorie consumption.15
Childhood fitness is a predictor of adult health status independent of BMI,2 yet national-level health surveillance of English children is limited solely to measurement of BMI.8 Following our 2009 report10 on declining fitness, the Chief Medical Officer8 suggested the need for systematic evaluation of children’s fitness. No action has, as yet, been taken following this recommendation despite publication of expert guidance14 and examples of cost-effective, safe and successful localised fitness surveillance projects.4, 10
Study limitations
Given the lack of systematic surveillance of English children’s fitness, these data are necessarily opportunistic. Our sample of schools was, however, carefully matched in terms of area-level deprivation. There was some between-school clustering of fitness in 2008 but this was less obvious in 2014. Our subsample analysis of more-deprived children was limited by sample size but the somewhat intriguing findings warrant further investigation through studies including data from larger, more diverse samples and the use of multilevel modelling.
Conclusions
Cardiorespiratory fitness is a independent marker of children’s health status. Any evidence of a decline in fitness is worrying, regardless of any concurrent changes in BMI. Continued reliance on BMI as the lone population-level measurement of children’s health status is insufficient. There is urgent need for interventions to increase physical activity in English youth, the efficacy of which could be evidenced via systematic assessment of changes in physical fitness.
References
Ruiz JR, Ortega FB, Rizzo NS, Villa I, Hurtig-Wennlof A, Oja L et al. High cardiovascular fitness is associated with low metabolic risk score in children: the European Youth Heart Study. Pediatr Res 2007; 61: 350–355.
Ortega FB, Ruiz JR, Castillo MJ, Sjostrom M . Physical fitness in childhood and adolescence: a powerful marker of health. Int J Obesity 2008; 32: 1–11.
Tomkinson GR, Leger LA, Olds TS, Cazorla G . Secular trends in the performance of children and adolescents (1980-2000): an analysis of 55 studies of the 20 m shuttle run test in 11 countries. Sports Med 2003; 33: 285–300.
Stratton G, Canoy D, Boddy LM, Taylor SR, Hackett AF, Buchan IE . Cardiorespiratory fitness and body mass index of 9-11-year-old English children: a serial cross-sectional study from 1998 to 2004. Int J Obes 2007; 31: 1172–1178.
Olds TS, Ridley K, Tomkinson GR . Declines in aerobic fitness: are they only due to increasing fatness? Med Sport Sci 2007; 50: 226–240.
Sandercock G, Voss C, McConnell D, Rayner P . Ten year secular declines in the cardiorespiratory fitness of affluent English children are largely independent of changes in body mass index. Arch Dis Child 2010; 95: 46–47.
Conrad D, Capewell S . Associations between deprivation and rates of childhood overweight and obesity in England, 2007-2010: an ecological study. BMJ Open 2012; 2: e000463.
Chief Medical Officer The 2009 Annual Report of the Cheif Medical Officer. Department of Heatlh: London, UK. Available at http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_114012.pdf 2009 (Last accessed 20 May 2015).
Government DfCaL The English Indices of Deprivation 2007. Department for Communities and Local Government: London, UK, 2007.
Cohen D, Voss C, Sandercock GRH . 'Fitness Testing' for children: let's mount the Zebra!. J Phys Act Health; e-pub ahead of print 5 June 2014.
Cole TJ, Freeman JV, Preece MA . Body mass index reference curves for the UK, 1990. Arch Dis Child 1995; 73: 25–29.
Batterham AM, Atkinson G . How big does my sample need to be? A primer on the murky world of sample size estimation. Phys Ther Sport 2005; 6: 153–163.
Georgiades E, Reilly JJ, Stathopoulou E, Livingston AM, Pitsiladis YP . BMI distribution changes in adolescent British girls. Arch Dis Child 2003; 88: 978–979.
Barker A, Williams C, Tolfrey K, Fawkner S, Sandercock G . The BASES Expert Statement on Measurement and Interpretation of Aerobic Fitness in Young People. British Association of Sport and Exercise Sciences: Leeds, UK, 2013.
Griffith R, Lluberas R, Lührmann M . IFS Briefing Notes (BN142) Gluttony in England? Long-term change in diet. Institute for Fiscal Studies: London, UK, 2013.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Sandercock, G., Ogunleye, A. & Voss, C. Six-year changes in body mass index and cardiorespiratory fitness of English schoolchildren from an affluent area. Int J Obes 39, 1504–1507 (2015). https://doi.org/10.1038/ijo.2015.105
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijo.2015.105
This article is cited by
-
Associations Between Motor Competence and Physical Activity, Physical Fitness and Psychosocial Characteristics in Adolescents: A Systematic Review and Meta-analysis
Sports Medicine (2023)
-
An Update on Secular Trends in Physical Fitness of Children and Adolescents from 1972 to 2015: A Systematic Review
Sports Medicine (2021)
-
Performance and reproducibility on shuttle run test between obese and non-obese children: a cross-sectional study
BMC Pediatrics (2017)
