
Abstract
Background:
Concern exists regarding gallstones as an adverse event of very-low-calorie diets (VLCDs; <800 kcal per day).
Objective:
To assess the risk of symptomatic gallstones requiring hospital care and/or cholecystectomy in a commercial weight loss program using VLCD or low-calorie diet (LCD).
Design:
A 1-year matched cohort study of consecutively enrolled adults in a commercial weight loss program conducted at 28 Swedish centers between 2006 and 2009. A 3-month weight loss phase of VLCD (500 kcal per day) or LCD (1200–1500 kcal per day) was followed by a 9-month weight maintenance phase. Matching (1:1) was performed by age, sex, body mass index, waist circumference and gallstone history (n=3320:3320). Gallstone and cholecystectomy data were retrieved from the Swedish National Patient Register.
Results:
One-year weight loss was greater in the VLCD than in the LCD group (−11.1 versus −8.1 kg; adjusted difference, −2.8 kg, 95% CI −3.1 to −2.4; P<0.001). During 6361 person–years, 48 and 14 gallstones requiring hospital care occurred in the VLCD and LCD groups, respectively, (152 versus 44/10 000 person–years; hazard ratio, 3.4, 95% CI 1.8–6.3; P<0.001; number-needed-to-harm, 92, 95% CI 63–168; P<0.001). Of the 62 gallstone events, 38 (61%) resulted in cholecystectomy (29 versus 9; hazard ratio, 3.2, 95% CI 1.5–6.8; P=0.003; number-needed-to-harm, 151, 95% CI 94–377; P<0.001). Adjusting for 3-month weight loss attenuated the hazard ratios, but the risk remained higher with VLCD than LCD for gallstones (2.5, 95% CI 1.3–5.1; P=0.009) and became borderline for cholecystectomy (2.2, 95% CI 0.9–5.2; P=0.08).
Conclusion:
The risk of symptomatic gallstones requiring hospitalization or cholecystectomy, albeit low, was 3-fold greater with VLCD than LCD during the 1-year commercial weight loss program.
Similar content being viewed by others
Introduction
Bariatric surgery is currently the most effective treatment for obesity,1 but all obese patients cannot undergo surgery because of guidelines, contraindications, capacity constraints and patient preferences. With the limited capacity of hospital-based obesity treatment, commercial weight loss programs including intensive treatment such as very-low-calorie diets (VLCDs; defined as <800 kcal per day) 2 are used by millions each year.2, 3, 4
The effects of commercial weight loss programs have shown to equal or even outweigh primary-care programs,5 with initial rapid weight loss using VLCD compared with low-calorie diet program (LCD; 1200–1500 kcal per day) inducing greater 1-year weight losses and lower dropout rates.6 However, the safety of commercial programs has rarely been studied, and using VLCD in commercial weight loss programs is a particular concern given the risk of adverse events as well as weight regain.7, 8, 9
A commonly described adverse event after rapid weight loss (including VLCD) is gallstones. Previous studies of VLCD-induced rapid weight loss have generally been small, of short duration, lacked control groups and used formulations with lower amounts of fat compared with the formulations used today.10, 11, 12, 13, 14 These previous studies have all identified gallstone formation with ultrasonography after VLCD use. However, the majority of the gallstones found in these studies were asymptomatic, and few led to symptoms. The risk of symptomatic gallstones requiring hospital care and/or cholecystectomy, potentially serious adverse events after VLCD use, has not been studied. Further, to the best of our knowledge, there are no large-scale studies on the safety of commercial weight loss programs.
The aim of this matched cohort study was to investigate in a real-life setting the risk of symptomatic gallstones leading to hospitalization or cholecystectomy after using VLCD (500 kcal per day for 6–10 weeks) compared with participants on LCD (1200–1500 kcal per day for up to 3 months) during a 1-year commercial weight loss program.
Methods
This matched cohort study was conducted in the commercial weight loss setting in Sweden. Participant data were retrieved from the database used by the commercial company to track customer progress and compliance. These data were linked to the National Patient Register,15 containing inpatient and nonprimary outpatient care, for outcome ascertainment, and to the Causes of Death Register for follow-up of vital status (Figure 1). The regional Ethics Committee in Stockholm, Sweden, approved the study.

Flow chart of included participants and matching.
Participants
Included participants were consecutively enrolled adult customers (age ⩾18years; n=8361) from the commercial weight loss company Itrim in Sweden (www.itrim.se) from 1 January 2006 to 31 May 2009. Data were collected from 28 centers across Sweden, as described elsewhere.6
Interventions
The weight loss program was of 1-year duration and comprised an initial 3-month weight loss phase, followed by a 9-month weight maintenance phase. At enrollment, participants selected one of three programs (VLCD, LCD or normal food, as described elsewhere6). In this study, we report data from the VLCD and LCD groups, as these are the two programs including liquid formula diets. Although all participants were paying customers and were free to choose weight loss method, the company used criteria for VLCD use, similar to the recommendations in the European (Scientific Co-operation ) SCOOP-report on VLCD use (Supplementary Table 1).16 VLCD participants needed to sign a form, where they had been informed that VLCD use carries an increased risk of the adverse events listed in the SCOOP-report on VLCD use.16
Weight loss phase (0–3 months)
VLCD: Liquid-based formula diet of 500 kcal per day for 6–10 weeks (Itrim, Stockholm, Sweden; 125 kcal per sachet, 4 sachets per day, each sachet contained 13 g protein, 15 g carbohydrates, 2 g fat and 3 g fiber; approved as sole source VLCD by the Swedish National Food Agency), followed by a 2-week gradual introduction of normal food. Early introduction of normal food (6 as opposed to the full 10 weeks) occurred when the participant was either satisfied with the achieved weight loss or had reached a body mass index (BMI) <25.0 kg m−2.
LCD: consisting of two calorie-restricted normal food meals and two formula diet meal replacement sachets (á 125 kcal), providing a total caloric intake of ∼1200–1500 kcal per day depending on body size and exercise levels. The normal food consisted of restricted portion sizes with a low overall energy density, high in protein, and with a low-glycemic index.6
Weight maintenance phase (3–12 months)
After the weight loss phase, the two groups entered the same 9-month weight maintenance program that included an exercise program (circuit training, with a mix of aerobic and strength training work-out stations, at the center 2–3 times per week for 30–45 min, physically active transport to and from work and using a Yamax SW-200 pedometer to encourage walking), dietary advice, self-monitoring and behavioral changes. Dietary advice included the use of restricted portion sizes, and eating a diet rich in protein and with a low-glycemic index, with a low overall energy density.6
Data collection
Participant data
Anthropometric data were collected by company-trained health coaches at baseline, 3, 6 and 12 months, and recorded into the database of the commercial company. Body weight was measured in a nonfasting state with the Tanita TBF-300 bioelectrical impedance monitor (Tanita Corporation, Tokyo, Japan). Waist circumference was measured midway between the iliac crest and the lower rib cage (exhaled) with a measuring tape and was classified as normal (<80 cm for women/<94 cm for men), increased risk (80–87/94–101 cm) and high risk (⩾88/102 cm).17 Height (without shoes) was measured by a wall-mounted stadiometer. World Health Organization BMI criteria (kg m−2) were used to classify participants as underweight (<18.5), normal weight (18.5–24.9), overweight (25.0–29.9) and obese class I/II/III (30.0–34.9/35.0–39.9/⩾40).18
Register data
Data on gallstones requiring hospital care, cholecystectomy, mortality and comorbidity were retrieved from National registers via register linkage. In Sweden, all the residents have a 10-digit personal identification number recorded in the medical files and nationwide health and census registers, enabling deterministic linkage.
History of gallstones, comorbidity and drug use
Data on the history of gallstones requiring hospital care during the 5 years before program were collected from the National Patient Register, which contains nationwide data on inpatient and nonprimary outpatient care in Sweden. Cholecystectomy history was retrieved from the same source from 1987 and onward. Data on hospital visits for malignancies (International Classification of Diseases [ICD] version 10 codes C00–C97) and circulatory disease (I00–I99) were also collected.
Drug dispensation data were retrieved from the nationwide Prescribed Drug Register during the 6 months preceding program start for antidiabetic drugs (Anatomical Therapeutic Classification [ATC] classification system codes A10A and A10B), antihypertensive drugs (C02, C03, C07, C08, C09), lipid-lowering drugs (C10AA, C10AB, C10AC, C10AD, C10B, C10AX), antidepressants (N06A), the antiobesity drugs orlistat (A08AB01), sibutramine (A08AA10) and rimonabant (A08AA11) and ursodeoxycholic acid (A05A).
Outcome and follow-up data
The primary outcome was gallstones requiring hospital care (cholelithiasis, ICD10 code K80). Cholecystectomy (procedure codes JKA20/JKA21) and all-cause mortality were investigated as secondary outcomes. Participants were followed from program start until first event, death, program end or 31 December, 2009, whichever came first. Cholecystectomized patients were excluded in the analysis of cholecystectomy but included in the analysis of gallstones requiring hospital care, as gallstones still can form in the gall ducts.
Gallstone and cholecystectomy data were retrieved from the National Patient Register.15 Mortality data were retrieved from the Causes of Death Register, which contains information on >99% of all deaths in Sweden.19
Statistical analysis
LCD participants were matched with replacement to VLCD participants 1:1 by age (+/−1-year), sex, BMI category, waist circumference category and previous gallstones. Analyses included all matched patients and were analyzed by intention to treat.
Kaplan–Meier curves were constructed to illustrate the absolute risk. To compare the risk of gallstones and cholecystectomy between the programs, we used conditional Cox regression to estimate hazard ratios over the 1-year follow-up (conditioned on the matching factors and adjusted for factors with significant differences at baseline).
A sensitivity analysis was conducted restricting the study population to participants without gallstones requiring hospital care during the 5 years preceding program start. Mortality was not analyzed due to few cases (one death due to unknown cause occurred in the VLCD group after the weight loss phase).
An exploratory analysis, combining the two intervention groups, was also conducted using multivariable Cox regression to investigate factors potentially associated with gallstones requiring hospital care, or cholecystectomy, including age, sex, baseline BMI, history of gallstones and weight loss during the rapid weight loss phase (0–3 months).
Data were analyzed using SAS (version 9.3). All reported P-values are two-sided and P-values <0.05 were regarded as statistically significant.
Results
After matching LCD participants (n=4588) with replacement to VLCD participants (n=3773) 1:1 by age, sex, BMI, waist circumference, and previous gallstones, 3320 participants remained in each group (Figure 1).
Baseline characteristics
At baseline, the mean age was 46 years, mean BMI 33.4 kg m−2 and 83% were women. Fifty-one percent of the participants were class I obese, 23% were class II obese, 8% were class III obese and 19% were overweight.
The two treatment groups were balanced regarding circulatory disease, malignancy history and the use of lipid-lowering drugs and antidepressants. There were fewer users in the VLCD than in the LCD group of antidiabetes drugs (1.8 versus 3.3%; mean difference, −1.4%, 95% CI −0.7 to −2.2%; P<0.001) and antihypertensives (16.7% versus 19.4%; mean difference, −2.7%, 95% CI −0.8 to −4.5%; P=0.005; Table 1). At baseline, 0.9% (n=58/6640) had a history of gallstones requiring hospital care, of which 74% (n=43/58) had been cholecystectomized (Table 1).
Weight change
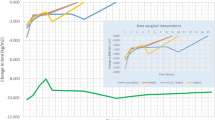
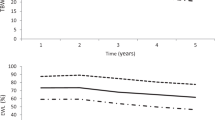
Eighty-two percent of the VLCD group and 78% in the LCD group completed the 1-year program (odds ratio, 1.3, 95% CI 1.2–1.5; P<0.001). After the initial weight loss phase (0–3 months; baseline observation carried forward), weight loss was 12.7 versus 7.9 kg (adjusted mean difference, 4.6, 95% CI 4.4–4.9; P<0.001). After the entire 1-year program, weight loss was 11.1 versus 8.1 kg (adjusted mean difference, 2.8, 95% CI 2.4–3.1; P<0.001; Figure 2). Data for the unmatched population have been described elsewhere.6

Weight change during the 1-year program LOCF, last observation carried forward (to 12 months); BOCF, baseline observation carried forward (to 12 months).
Risk of gallstones requiring hospital care
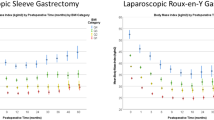
During 6361 person–years of follow-up, 48 gallstones occurred in the VLCD group and 14 in the LCD group (152 versus 44 per 10 000 person–years; conditional hazard ratio, 3.4, 95% CI 1.8−6.3; P<0.001; Figure 3; Table 2). The risk difference was 108 per 10 000 person–years (95% CI 59–157; P<0.001), resulting in a number-needed-to-harm of 92 (95% CI 63–168; P<0.001). Adjusting the main analysis for weight loss during the first 3 months attenuated the hazard ratio, but the hazard ratio remained higher with VLCD than LCD (2.5, 95% CI 1.3–5.1; P<0.001).

Risk of gallstones requiring hospital care (upper panel) and cholecystectomy (lower panel) by weight loss program. VLCD, very-low-calorie diet; LCD, low calorie diet.
Risk of cholecystectomy
Including only participants who did not undergo a cholecystectomy preceding program start (n=3159 in the VLCD group and 3159 in the LCD group), 38 cases of cholecystectomy were performed during 6067 person–years of follow-up, of which 29 were in the VLCD group and 9 in the LCD group (96 versus 30 per 10 000 person–years; conditional hazard ratio, 3.2, 95% CI 1.5–6.8; P=0.003; number-needed-to-harm, 151, 95% CI 94–377; P<0.001; Figure 3; Table 2). Adjustment for weight loss during the first 3 months attenuated the hazard ratio (2.2, 95% CI 0.9–5.2; P=0.08).
Sensitivity analysis
Excluding participants with gallstones requiring hospital care during the 5 years preceding program start (n=58) resulted in similar results for gallstones (46 versus 13 in the VLCD and LCD group, respectively; 147 versus 41 per 10 000 person–years; hazard ratio, 3.4, 95% CI 1.8–6.3; number-needed-to-harm, 94, 95% CI 65–173; P<0.001) and cholecystectomy (28 in the VLCD group compared with 9 in the LCD group; 93 versus 30 per 10 000 person–years; hazard ratio, 3.2, 95% CI 1.5–6.8; number-needed-to-harm, 158, 95% CI 97–420; P=0.002).
Exploratory analysis: predictors of gallstones and cholecystectomy during follow-up
In multivariable analysis, the risk of developing gallstones requiring hospital care was higher in women than in men, in younger than in older participants, in those with a higher baseline BMI, among those who lost the most weight and in those with a history of gallstones (irrespective of cholecystectomy status; Supplementary Table 2). For cholecystectomy, the same factors as for gallstones requiring care were associated with an increased risk for cholecystectomy (Supplementary Table 3).
Discussion
In our analysis of symptomatic gallstones requiring hospital care or cholecystectomy in participants using either VLCD or LCD for the first 3 months of a 1-year commercial weight loss program, we found the absolute risk of gallstones as well as cholecystectomy to be low but approximately three times higher in the VLCD than in the LCD group. After adjusting for weight loss during the first 3 months, the risk was attenuated but remained higher with VLCD than LCD, suggesting a direct effect of VLCD on gallstone disease. To the best of our knowledge, this is the largest controlled study of VLCD and of the risk of severe gallstone problems and the first large-scale safety analysis of a commercial program.
Previous research
Previous studies have investigated the association between VLCD and ultrasonography-assessed gallstone formation, rather than the risk of gallstones as a serious adverse event requiring hospital care and/or cholecystectomy. The majority of these studies were conducted in the late 1980s and early 1990s using VLCDs containing low levels of fat (≈1g per day).10, 11, 12, 13, 14 In a review of these studies,20 Everhart reported that 10–25% of VLCD participants developed gallstones, one-third of which were symptomatic. Limitations of these studies were the lack of control groups, small sample sizes and short follow-up (8–36 weeks).10, 11, 12, 13, 14 Later studies included VLCDs containing higher fat content (12–30 g per day),21, 22, 23, 24 two of which were randomized controlled trials.21, 22 None developed systematic gallstones in the high-fat group in either of the studies, suggesting that an adequate fat intake reduces gallstone formation. The fat content of the VLCD in our study was 7–9 g per day, consistent with the 7 g per day recommendation given by the European SCOOP-report on VLCD use.16 The higher risk with VLCD in our study suggests that fat content may need to be increased even further to reduce the risk to LCD levels.
Mechanisms
Increased risk for gallstone formation during VLCDs could be explained by inadequate fat content of the diet and/or the rapid weight loss associated with VLCDs. Rapid weight loss, either by VLCD or bariatric surgery, is a known risk factor for gallstone formation.20 The two most commonly suggested mechanisms for gallstone formation are supersaturation of bile with cholesterol, leading to cholesterol crystallization and stone formation, and the insufficient gallbladder emptying due to impaired motility.25 Rapid weight loss induced by VLCDs is believed to affect both the mechanisms: Supersaturation is believed to be caused by decreased bile salt levels and increased cholesterol levels, and impaired motility due to reduced gallbladder stimulation because of the low-fat content.26, 27 However, as described previously, a fat intake of 7–10 g per day has been reported as a threshold for maintaining an efficient gallbladder emptying.16, 26 The majority of the gallstones requiring hospital care occurred during the maintenance phase (37/48 in the VLCD group and 8/14 in the LCD group). This was also the case in a previous study of VLCD as a treatment for sleep apnea (3/3 gallstones reported during the maintenance phase).28, 29
Clinical implications
Increased risk of gallstone formation during and after VLCD-induced rapid weight loss is incorporated in clinical recommendations as an adverse event, advising physicians to inform patients about this risk, but the risk magnitude has been unclear.7, 16, 20 Our findings indicate a small, absolute but substantially elevated relative risk of gallstones requiring hospital care and/or cholecystectomy when using VLCD instead of LCD.
Whether the benefits of the additional weight loss in the VLCD group are worth the extra risk for gallstones and cholecystectomy may depend on patients’ disease and risk factor status, as well as their preferences. Supplementation with omega-3 fatty acids and/or the use of ursodeoxycholic acid during the rapid weight loss phase could possibly reduce gallstone formation.26, 30
Strengths and limitations
The strengths of the current study include the large sample of weight loss participants in a real-life setting, with a direct VLCD and LCD comparison. With the risk of symptomatic gallstones being low, statistical power may become an issue in smaller studies. Our large study made it possible to study the risk of symptomatic gallstones leading to hospitalization and/or cholecystectomy as a serious adverse event to VLCD. Further, the outcomes were prospectively reported and data were collected routinely on a nationwide level in the universally accessible Swedish health-care system, with virtually complete follow-up.
The main limitation was the nonrandomized design. Baseline differences in age, sex, BMI, waist circumference and gallstone history were handled by matching. Multivariable adjustment was used for handling remaining baseline imbalances. However, residual confounding may exist. The results appeared to be robust in our sensitivity analyses.
Second, participants had selected and paid for the treatment themselves, possibly limiting generalizability to the wider overweight and obese population. Finally, the National Patient Register contains data on inpatient and nonprimary outpatient visits for gallstones, not visits in primary care, or undetected asymptomatic gallstones. Our results may therefore not be generalizable to mild or asymptomatic gallstones. However, our primary outcomes were gallstones requiring hospital care and cholecystectomies. Gallstones treated in the primary care, at home, or not treated at all, are likely both less serious for the patient and less costly for society.
Conclusion
The absolute risk of gallstones as well as cholecystectomy was found to be low but approximately three times higher in the VLCD than in the LCD group during the 1-year commercial weight loss program. After adjusting for weight loss during the first 3 months, the risk was attenuated but remained higher with VLCD than LCD, suggesting a direct effect of VLCD on gallstone disease.
References
Sjostrom L, Narbro K, Sjostrom CD, Karason K, Larsson B, Wedel H et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med 2007; 357: 741–752.
Tsai AG, Wadden TA . Systematic review: an evaluation of major commercial weight loss programs in the United States. Ann Intern Med 2005; 142: 56–66.
Heshka S, Anderson JW, Atkinson RL, Greenway FL, Hill JO, Phinney SD et al. Weight loss with self-help compared with a structured commercial program: a randomized trial. JAMA 2003; 289: 1792–1798.
Rock CL, Flatt SW, Sherwood NE, Karanja N, Pakiz B, Thomson CA . Effect of a free prepared meal and incentivized weight loss program on weight loss and weight loss maintenance in obese and overweight women: a randomized controlled trial. JAMA 2010; 304: 1803–1810.
Jebb SA, Ahern AL, Olson AD, Aston LM, Holzapfel C, Stoll J et al. Primary care referral to a commercial provider for weight loss treatment versus standard care: a randomised controlled trial. Lancet 2011; 378: 1485–1492.
Hemmingsson E, Johansson K, Eriksson J, Sundstrom J, Neovius M, Marcus C . Weight loss and dropout during a commercial weight-loss program including a very-low-calorie diet, a low-calorie diet, or restricted normal food: observational cohort study. Am J Clin Nutr 2012; 96: 953–961.
National Task Force on the Prevention and Treatment of Obesity NIoH. Very low-calorie diets. JAMA 1993; 270: 967–974.
Saris WH . Very-low-calorie diets and sustained weight loss. Obes Res 2001; 9 (Suppl 4): 295S–301S.
Tsai AG, Wadden TA . The evolution of very-low-calorie diets: an update and meta-analysis. Obesity (Silver Spring) 2006; 14: 1283–1293.
Broomfield PH, Chopra R, Sheinbaum RC, Bonorris GG, Silverman A, Schoenfield LJ et al. Effects of ursodeoxycholic acid and aspirin on the formation of lithogenic bile and gallstones during loss of weight. N Engl J Med 1988; 319: 1567–1572.
Kamrath RO, Plummer LJ, Sadur CN, Adler MA, Strader WJ, Young RL et al. Cholelithiasis in patients treated with a very-low-calorie diet. Am J Clin Nutr 1992; 56 (1 Suppl): 255S–257S.
Liddle RA, Goldstein RB, Saxton J . Gallstone formation during weight-reduction dieting. Arch Intern Med 1989; 149: 1750–1753.
Shiffman ML, Kaplan GD, Brinkman-Kaplan V, Vickers FF . Prophylaxis against gallstone formation with ursodeoxycholic acid in patients participating in a very-low-calorie diet program. Ann Intern Med 1995; 122: 899–905.
Yang H, Petersen GM, Roth MP, Schoenfield LJ, Marks JW . Risk factors for gallstone formation during rapid loss of weight. Dig Dis Sci 1992; 37: 912–918.
Ludvigsson JF, Andersson E, Ekbom A, Feychting M, Kim JL, Reuterwall C et al. External review and validation of the Swedish national inpatient register. BMC Public Health 2011; 11: 450.
SCOOP-VLCD. SCOOP-VLCD Task 7.3. Scientific Co-operation on Questions Relating to Food: Directorate-General Health and Consumer Protection, European Union. In 2002.
Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009; 120 (16): 1640–1645.
WHO. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser 2000; 894, i-xii 1–253.
Socialstyrelsen. The Causes of Death Register. Available from http://www.socialstyrelsen.se/register/dodsorsaksregistret 2011.
Everhart JE . Contributions of obesity and weight loss to gallstone disease. Ann Intern Med 1993; 119: 1029–1035.
Festi D, Colecchia A, Orsini M, Sangermano A, Sottili S, Simoni P et al. Gallbladder motility and gallstone formation in obese patients following very low calorie diets. Use it (fat) to lose it (well). Int J Obes Relat Metab Disord 1998; 22: 592–600.
Gebhard RL, Prigge WF, Ansel HJ, Schlasner L, Ketover SR, Sande D et al. The role of gallbladder emptying in gallstone formation during diet-induced rapid weight loss. Hepatology 1996; 24: 544–548.
Hoy MK, Heshka S, Allison DB, Grasset E, Blank R, Abiri M et al. Reduced risk of liver-function-test abnormalities and new gallstone formation with weight loss on 3350-kJ (800-kcal) formula diets. Am J Clin Nutr 1994; 60: 249–254.
Spirt BA, Graves LW, Weinstock R, Bartlett SJ, Wadden TA . Gallstone formation in obese women treated by a low-calorie diet. Int J Obes Relat Metab Disord 1995; 19: 593–595.
Maddrey WC, Schiff ER, Sorrell MF . Ovid. Schiff's diseases of the liver. In: Chapter 22 Gallstone Disease: Pathogenesis and Treatment 10th ed. Lippincott Williams & Wilkins: Philadelphia, 2007. pp p.640–663.
Festi D, Colecchia A, Larocca A, Villanova N, Mazzella G, Petroni ML et al. Review: low caloric intake and gall-bladder motor function. Aliment Pharmacol Ther 2000; 14 (Suppl 2): 51–53.
Erlinger S . Gallstones in obesity and weight loss. Eur J Gastroenterol Hepatol 2000; 12: 1347–1352.
Johansson K, Hemmingsson E, Harlid R, Trolle Lagerros Y, Granath F, Rossner S et al. Longer term effects of very low energy diet on obstructive sleep apnoea in cohort derived from randomised controlled trial: prospective observational follow-up study. BMJ 2011; 342: d3017.
Johansson K, Neovius M, Lagerros YT, Harlid R, Rossner S, Granath F et al. Effect of a very low energy diet on moderate and severe obstructive sleep apnoea in obese men: a randomised controlled trial. BMJ 2009; 339: b4609.
Mendez-Sanchez N, Gonzalez V, Aguayo P, Sanchez JM, Tanimoto MA, Elizondo J et al. Fish oil (n-3) polyunsaturated fatty acids beneficially affect biliary cholesterol nucleation time in obese women losing weight. J Nutr 2001; 131: 2300–2303.
Acknowledgements
This study was partly funded by a grant from the Itrim International. The funders had no role in the design or conduct of the study; analysis or interpretation of the data; preparation, review or approval of the manuscript.
Author Contributions
Dr Johansson and Dr Neovius had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: Johansson, Neovius. Acquisition of data: Johansson, Neovius, Hemmingsson. Analysis and interpretation of data: Johansson, Neovius, Sundström. Drafting of the manuscript: Johansson, Neovius. Critical revision of the manuscript for important intellectual content: Johansson, Neovius, Sundström, Hemmingsson, Marcus. Statistical analysis: Johansson, Neovius. Obtained funding: Hemmingsson. Study supervision: Johansson, Neovius.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
All authors have completed ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Hemmingsson report that he has received consultancy fees from Itrim and was employed part-time by Itrim as program director during 2006-2008. Drs Neovius, Sundström and Marcus report that they are members of Itrim’s Scientific Advisory Board. Dr Johansson has no financial relationships with Itrim, but received a grant from Cambridge Weight Plan, Northants, (manufacturer of another VLCD formula) for two studies examining the effect of weight loss on obstructive sleep apnea.28, 29
Additional information
Supplementary Information accompanies this paper on International Journal of Obesity website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by/3.0/
About this article
Cite this article
Johansson, K., Sundström, J., Marcus, C. et al. Risk of symptomatic gallstones and cholecystectomy after a very-low-calorie diet or low-calorie diet in a commercial weight loss program: 1-year matched cohort study. Int J Obes 38, 279–284 (2014). https://doi.org/10.1038/ijo.2013.83
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijo.2013.83
Keywords
This article is cited by
-
Meal replacement in dietary management of type-2 diabetes mellitus: a scoping review protocol
Systematic Reviews (2020)
-
The management of very low-calorie ketogenic diet in obesity outpatient clinic: a practical guide
Journal of Translational Medicine (2019)
-
Gallstones
Nature Reviews Disease Primers (2016)
-
Follow the LEADER—Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results Trial
Diabetes Therapy (2016)
-
Gallstone disease in severely obese children participating in a lifestyle intervention program: incidence and risk factors
International Journal of Obesity (2014)
