
Abstract
Although the upper arm has the shape of a truncated cone, cylindrical cuffs and bladders are currently used for blood pressure (BP) measurement. The aims of this study were to describe upper arm characteristics and to test the accuracy of a standard adult-size conical cuff coupled to an oscillometric device over a wide range of arm circumferences. Arm characteristics were studied in 142 subjects with arm circumferences ranging from 22 to 45 cm (study 1). In a subset of 33 subjects with the same range of arm circumferences, a rigid conical cuff with standard-size bladder (12.6 × 24.0 cm) and a rigid cylindrical cuff (13.3 × 24.0 cm), both coupled to a Microlife BP A100 device, were tested according to the requirements of the protocol of the European Society of Hypertension (ESH; study 2). Study 1. In all subjects, upper-arm shape was tronco-conical with slant angles ranging from 89.5° to 82.2°. In a multiple linear regression analysis, only arm circumference was an independent predictor of conicity (P<0.001). Study 2. The rigid conical cuff passed all three phases of the ESH protocol for systolic and diastolic BPs. Mean device-observer BP differences obtained with the conical cuff were unrelated to arm circumference. When the rigid cylindrical cuff was used, ESH criteria were not satisfied, and the cuff overestimated systolic BPs in subjects with large arms. BP can be measured accurately with the use of a standard-size rigid conical cuff coupled to a BP A100 device for a wide range of arm circumferences.
Similar content being viewed by others
Introduction
Although the upper arm has the shape of a truncated cone, cylindrical (rectangular) cuffs and bladders are currently used for brachial blood pressure (BP) measurement. However, when the arm circumference near the shoulder is much greater than the arm circumference near the elbow, a cylindrical cuff may challenge the ability of a health care provider to measure BP. In such arms, the elbow end of the cuff remains loose and may extend past the elbow in subjects with short humerus bones. When a large-size cylindrical cuff is inflated, it will expand irregularly over the lower part of a conical arm, making it impossible for a doctor to perform a reliable measurement. This problem is even greater for cuffs made of rigid material, which can barely fit the distal part of a conical arm. In a previous study performed with obese patients, a conical cuff was shown to reflect arterial BP more accurately than standard cylindrical cuffs.1 However, this problem has been overlooked in the literature, and it is not known what shape and size an optimal cuff should have in order to fit the arms of most subjects. Thus, the aims of the present study were to study the shape of the upper arm in a large sample of subjects with a wide range of arm circumferences and to test a conical cuff potentially suitable for the majority of the subjects. We also evaluated the accuracy of a rigid conical cuff in comparison with a rigid cylindrical cuff, both coupled to a validated oscillometric automatic device (BP A100 model, Bonso et al.2) in a subsample of the main group.
Methods
Subjects
Arm characteristics were studied in 142 subjects (of whom 74 were men) aged 58±18 years, with mid-arm circumference ranging from 22 to 45 cm (study 1). This study was designed with the aim of assessing the shape of the arm in a large sample. A validation study was performed in 33 out of these 142 subjects with BPs within the range required by European Society of Hypertension (ESH) rules (study 2). In all, 28 subjects were excluded from the validation study because the BP ranges were complete (n=18), Korotkoff sounds were of poor quality (n=4), the BP was out of range (n=4) or there was atrial fibrillation (n=2). All subjects agreed to participate in the protocol and gave informed consent.
Measurements
To calculate the frustum of a cone slant angle, the length of the upper arm was measured from the axilla to the antecubital fossa, the proximal arm circumference was measured just below the axilla, and the distal arm circumference was measured just above the antecubital fossa. For all measurements, subjects were placed in the supine position with arms resting comfortably at the sides and forearms in the pronated position.
In this calculation, the limb is visualized to be in the shape of a truncated cone. The circumferences of the extremity at the proximal and distal limits of the segment, together with the length between them, were used to calculate the slant angle (SA, in degrees), using the formula:

where ‘C1’ is the proximal arm circumference, ‘C2’ is the distal arm circumference and ‘L’ is the arm length. The conicity index (CI, in percent) was calculated from the formula:

where ‘D1’ is the proximal arm diameter, ‘D2’ is the distal arm diameter and ‘L’ is the arm length. The upper-arm middle circumference was measured at the midpoint of the distance between the acromion and the olecranon. Skinfold thickness was measured in triplicate at the triceps and biceps with a manual caliper, and the average of the six measurements was defined as the skinfold thickness. BP was measured with a mercury sphygmomanometer in the sitting position.
Procedures
All procedures followed were in accordance with institutional guidelines. For study 1, anthropometric characteristics were measured for 142 subjects. Evaluation of the accuracy of the conical cuff vs. that of the cylindrical cuff (study 2) was performed according to ESH protocol, using the same 33 subjects for assessment of each cuff type.3 The validation team consisted of three persons experienced in device validation. The two observers used for the present validation study (EB and FD) have participated in previous published validation studies.2, 4 Devices were tested according to the suggestions of the ESH, and the agreement between these two observers was 0.7±2.1 mm Hg for systolic BP (SBP) and −0.5±2.8 mm Hg for diastolic BP (DBP). Both observers were blinded to each other's measurement values and took BP measurements with a mercury sphygmomanometer placed on the upper arm. For arm circumferences ⩽30 cm, a 12 × 24 cm bladder was used. For arm circumferences >30 cm, the bladder had to cover at least 80% of the arm circumference. A series of graduated-size sphygmomanometer cuffs were used; each cuff was adapted for use on a limb of a size related to that cuff.2 To quantify the error due to miscuffing in large arms, observer measurements were also performed with a standard bladder (12 × 24 cm) in the subjects with arm circumferences >30 cm (n=17). Sequential measurements of the same arm were performed. Before starting comparative readings, the two observers took a BP measurement, and the mean values were used to categorize the participant into a low, medium or high range for both SBP and DBP, separately. Then, BP was measured with the test device by the supervisor, in order to allow the test instrument to determine the BP characteristics of the subject. Thereafter, four sequential readings were taken by observers 1 and 2 (BP1, BP3, BP5 and BP7), and three readings were taken by the supervisor with each of the two cuffs connected to the oscillometric device (BP2conical and BP2cylindrical, BP4conical and BP4cylindrical, and BP6conical and BP6cylindrical). The conical and cylindrical cuffs were tested in a crossover manner. The discrepancy between the readings provided by the device coupled to each of the two cuffs and the mean of observers’ measurements were allocated into three zones of accuracy, as suggested by ESH protocol.3 In the 17 subjects with arm circumference >30 cm, observer measurements were also performed with a 12 × 24 cm bladder (ST) soon after the first measurements, with an appropriately sized bladder (A-S). Thus, in these subjects, the observer measurement sequence was BP1A−S and BP1ST, BP3A−S and BP3ST, BP5A−S and BP5ST, BP7A−S and BP7ST.
Cuffs and BP device
A rigid conical cuff and a rigid cylindrical cuff, both coupled to a Microlife BPA100 device, were tested in this study. The cuffs were formed of a flexible compliant laminate having two layers that are impermeable to air. The conical cuff was formed with an upper, longer, arcuate edge of 28.6 cm and a lower, shorter edge of 27.2 cm (Figure 1). Radial edges extended between the upper and lower edges. The slant angle of the frustum of the cone corresponding to the cuff and bladder when the cuff was encompassing a limb was 88°. In the cylindrical cuff, both the upper and lower sides had the same length (27.0 cm). The cylindrical cuff was provided with a rectangular 13.3 × 24.0 cm bladder. The bladder for the conical cuff had a slightly arcuate upper edge and was 12.9 × 24.0 cm in size (Figure 1). The BPA 100 device used was an oscillometric automatic device, which has proved accurate for BP measurement at the upper arm.2, 5 This device included novel technology that performed an analysis of the oscillometric signal amplitude during cuff inflation. After this analysis, a microprocessor made an adjustment of the gain factor based on the individual arm characteristics for the following deflationary measurement phase.2

Schematic representation of a conical cuff.
Statistical analysis
Data are presented as mean±s.d. unless specified. For comparisons, ANOVA was used adjusting for age and sex. The significance of differences in categorical variables was assessed with the χ2-test or Fisher's exact test. Relationships between continuous variables were assessed using Pearson's correlation test. Predictors of CI and of the discrepancy between observer and device measurements were included in linear multivariable regression analyses. A P-value <0.05 was considered statistically significant
Results
Study 1
Arm characteristics were evaluated in 142 subjects (74 men) aged 58±18 years, with mid-arm circumferences ranging from 22 to 45 cm. The mean±s.d. SBP was 146±21 mm Hg, (range, 110–180 mm Hg), and the mean DBP was 90±15 mm Hg (range, 54–112 mm Hg). In all subjects, upper-arm shape was tronco-conical, with slant angles ranging from 89.5° to 82.2° (mean, 86.2±1.6°) and conicity indices ranging from 1.3 to 27.6% (mean, 13.3±5.6%). The circumference near the shoulder was always greater than the circumference near the elbow with differences ranging from 1 to 20 cm and a mean value of 8.7±3.8 cm. Conicity indices were similar in men and women and were correlated to mid-arm circumference (P<0.001), average skinfold thickness (P<0.001), and body weight (P<0.001), but were unrelated to arm length. However, in a multiple linear regression including age, sex, BP and all anthropometric variables, only arm circumference independently predicted the CI (P<0.001).
Study 2
In all, 33 subjects (19 men) with BP values within the range required by ESH rules were used for the validation study. Their average SBP was 144±21 mm Hg (range, 110–180 mm Hg), and their average DBP was 87±15 mm Hg (range, 54–110 mm Hg). Characteristics of the 33 subjects used for the validation study and those of the rest of the group are reported in Table 1. Demographic variables were similar in the two groups. However, upper arm length, proximal circumference and CI were greater in the subjects who participated in the validation study (Table 1).
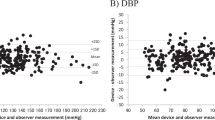
The standard-size rigid conical cuff coupled to the BPA100 device passed all three phases of the ESH protocol for systolic and diastolic BPs (Table 2). In contrast, when the standard-size rigid cylindrical cuff connected to the BP A100 device was tested, the requirements of the ESH protocol were not satisfied for SBP (Table 3). Device-observer BP differences obtained with the cuff with conical shape are presented in Figure 2. Differences were unrelated to arm circumference for both SBP (r=0.21, P=0.24) and DBP (r=−0.11, P=0.55). In addition, when the subjects were divided into two subgroups of arm circumference above or below the median (30.0 cm), similar device-observer differences (either with sign or in absolute values) were observed in the two groups (Table 4). However, when the rigid cylindrical cuff was tested, a marked overestimation of SBP was observed in the subjects with arm circumference >30 cm (Table 4). The device-observer discrepancies differed significantly according to arm size for DBP as well, but there was not a clear tendency for the device to overestimate DBP in the group with larger arms.

Plots of systolic (upper plot) and diastolic (lower plot) BP A100-observer blood pressure differences obtained with the rigid conical cuff. The x axis represents the mean of device and observer measurements. The y axis represents the difference between the device and observer measurements. A positive value indicates that the device measurement was greater than the observer measurement.
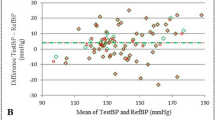
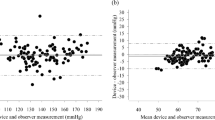
In a multiple linear regression, both systolic and diastolic device-observer BP differences obtained with the rigid conical cuff were unrelated to age, sex, BP, body height and weight, arm length and circumference, skinfold thickness and arm CI (Figure 3). Systolic and diastolic device-observer BP differences obtained with the rigid cylindrical cuff were closely correlated to arm circumference (P<0.001), skinfold thickness (P<0.001) and CI (P<0.001, Figure 4). In multiple regression analyses, independent predictors of the SBP device-observer differences obtained with the rigid cylindrical cuff included male gender (P=0.001), CI (P=0.001), skinfold thickness (P=0.028) and arm length in an inverse manner (P=0.020). Independent predictors of the DBP device-observer difference included male gender (P=0.005) and CI (P<0.001). In the 17 subjects with arm circumferences >30 cm, the auscultatory BP measurement performed by the observers with the standard-size cuff overestimated systolic and diastolic BPs taken with the appropriate-size cuffs by 15.0±8.9 mm Hg and 14.5±7.4 mm Hg, respectively.

Plots of the systolic (upper plot) and diastolic (lower plot) BP A100-observer blood pressure differences obtained with the rigid conical cuff. The x axis represents the conicity index. The y axis represents the difference between the device and observer measurements. A positive value indicates that the device measurement was greater than the observer measurement. Systolic and diastolic blood pressure differences were unrelated to conicity index.

Plots of the systolic (upper plot) and diastolic (lower plot) BP A100-observer blood pressure differences obtained with the rigid cylindrical cuff. The x axis represents the conicity index. The y axis represents the difference between the device and observer measurements. A positive value indicates that the device measurement was greater than the observer measurement. Systolic and diastolic blood pressure differences were correlated with the conicity index.
Discussion
Our results show that the upper arm shape was tronco-conical in all subjects investigated, with the circumference near the shoulder being greater than the circumference near the elbow. The difference between the circumferences ranged from 1 to 20 cm, with an average value of 8.7 cm. The conical shape of the arm was closely correlated to the degree of obesity and arm circumference. However, in a linear multiple regression analysis, only arm circumference remained an independent predictor of the CI.
The conical shape of the upper arm often challenges the ability of the health care personnel to measure BP accurately. In fact, the use of a cylindrical cuff on large arms may cause an overestimation of the true BP, as shown many years ago by Maxwell et al.1 with the auscultatory method in a general population. Using a conical cuff, these authors obtained lower SBP and DBP readings compared with those obtained with a cylindrical cuff in obese individuals. This discrepancy was attributed to the fact that the conical cuff fits better on larger upper arms than the cylindrical cuff. BP measurement with a cuff of the appropriate size is particularly difficult in obese subjects with short humerus bones. In such arms, the elbow end of a thigh-sized cuff may extend past the elbow by several centimeters. These problems are clearly greater when cuffs made of rigid material are used.6 Typically, a user (who may be the patient, if the patient is taking his or her own BP) will wrap the cuff, using his or her own tactile sense to gauge the amount of tension applied to the cuff, often resulting in improper wrapping of the cuff. Improper cuff tension will result in an incorrect BP measurement. If too little tension is provided, too much air must be pumped into the bladder and the measurement cycle may be unnecessarily long, resulting in an inaccurate measurement. If too much tension is provided, the blood vessels in the arm may be compressed before the bladder being inflated, also resulting in an inaccurate measurement. Therefore, there exists a need for a cuff that a user can apply while being assured that the proper amount of tension is being used for its placement. A solution may be achieved with the use of rigid cuffs, for which the amount of tension may be pre-set by the manufacturer to conform to the amount of tension required for accurate BP measurement. However, a rigid cylindrical cuff cannot exert a uniform pressure on a conical arm, because the distal part will remain loose and will transmit a lower pressure to the subcutaneous tissue overlying the artery. This condition can be frequently encountered in subjects with large arms (for whom large-size cuffs should be used) and can be an important source of measurement errors, particularly in men with muscular arms.7 Indeed, in the present study, male gender was a significant predictor of the device-observer BP discrepancy observed with the use of the cylindrical cuff, which may be because of the effect of bulging bicep muscles in individuals whose arms have highly muscular compositions.
Today, standard-size cuffs are available that, when coupled to oscillometric devices, can provide accurate measurements over a wide range of arm circumferences, up to 40 cm and higher.2, 8 It should be noted that the present recommendations for cuff size with relation to arm circumference apply to the auscultatory method, whereas little is known about the relationship between cuff size and performance for oscillometric devices. Some oscillometric devices are provided along with software that performs an analysis of the measurement signal during cuff inflation and, subsequently, adjusts the device parameters based on the characteristics of the individual arm being measured for the following deflationary phase.2, 8 These devices have been shown to provide reliable BP readings when coupled to cuffs of standard size as well, but such cuffs are considered inappropriate for measuring BP with traditional sphygmomanometry in subjects with arm circumference >32 cm.9, 10 However, if a rigid cylindrical cuff is used these devices may also provide inaccurate readings when used in large-size conical arms because of the aforementioned reasons. In the present study, when the rigid cylindrical cuff was used in combination with the BP A100 monitor, the device performed better than the auscultatory method, especially for DBP. However, this combination clearly overestimated SBP in the group of subjects with mid-point arm circumferences >30 cm. In contrast, when the conical cuff was used, the device provided accurate readings, with similar device-observer differences in the group with standard arm sizes and the group with large arms, and comfortably passed phases 1 and 2 of the ESH protocol.
Although choice of appropriate cuff is a key element for obtaining an accurate BP measurement,11, 12, 13 data from the literature indicate that arm size is not taken into account by patients performing home BP monitoring and even by some health care professionals.11, 14 The use of a single cuff able to measure BP accurately over a wide range of arm circumferences, would thus improve the accuracy of BP measurement. The present results obtained with the BP A100 monitor coupled to a standard size rigid conical cuff show that this equipment can measure BP accurately in subjects with arm circumferences ranging from 22 to 44 cm. The results further emphasize the importance of using a conical cuff in subjects with large arms, at least when the non-stretch bag surrounding the bladder is constructed of rigid material.
References
Maxwell GF, Pruijt JF, Arntzenius AC . Comparison of the conical cuff and the standard rectangular cuffs. Int J Epidemiol 1985; 14: 468–472.
Bonso E, Dorigatti F, Palatini P . Accuracy of the BP A100 blood pressure measuring device coupled with a single cuff with standard-size bladder over a wide range of arm circumferences. Blood Press Monit 2009; 14: 216–219.
O’Brien E, Pickering T, Asmar R, Myers M, Parati G, Staessen J, Mengden T, Imai Y, Waeber B, Palatini P, Gerin W . Working Group on Blood Pressure Monitoring of the European Society of Hypertension. European Society of Hypertension International protocol for validation of blood pressure measuring devices in adults. Blood Press Monit 2002; 7: 3–17.
Bonso E, Dorigatti F, Palatini P . Validation of Panasonic EW3106 and EW3109 devices for blood pressure measurement according to the International Protocol. Blood Press Monit 2010; 15: 55–58.
Stergiou GS, Giovas PP, Neofytou MS, Adamopoulos DN . Validation of the Microlife BPA100 Plus device for self-home blood pressure measurement according to the International Protocol. Blood Press Monit 2006; 11: 157–160.
Evans CE, Haynes RB, Goldsmith CH, Hewson SA . Home blood pressure-measuring devices: a comparative study of accuracy. J Hypertension 1989; 7: 133–142.
Fonseca-Reyes S, Fajardo-Flores I, Montes-Casillas M, Forsyth-MacQuarrie A . Differences and effects of medium and large adult cuffs on blood pressure readings in individuals with muscular arms. Blood Press Monit 2009; 14: 166–171.
Stergiou GS, Tzamouranis D, Nasothimiou EG, Protogerou AD . Can an electronic device with a single cuff be accurate in a wide range of arm size? Validation of the Visomat Comfort 20/40 device for home blood pressure monitoring. J Hum Hypertens 2008; 22: 796–800.
Hussain A, Cox JG . An audit of the use of sphygmomanometers. Br J Clin Pract 1996; 50: 136–137.
Villegas I, Arias IC, Botero A, Escobar A . Evaluation of the technique used by health-care workers for taking blood pressure. Hypertension 1995; 26: 1204–1206.
O’Brien E . Review: a century of confusion; which bladder for accurate blood pressure measurement? J Hum Hypertens 1996; 10: 565–572.
Alpert BS . Cuff width and accuracy of measurement of blood pressure. Blood Press Monit 2000; 5: 151–152.
McKay DW, Campbell NR, Parab LS, Chockalingam A, Fodor JG . Clinical assessment of blood pressure. J Hum Hypertens 1990; 4: 639–645.
Stergiou GS, Malakos JS, Voutsa AV, Achimastos AD, Mountokalakis TD . Home monitoring of blood pressure: limited value in general practice. J Hum Hypertens 1996; 10: 219–232.
Acknowledgements
This work was funded by a grant from Microlife AG, Espenstrasse 139, CH 9443, Widnau, Switzerland and by the University of Padova, Padua, Italy.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
In this appendix, basic information about the Microlife BP A100 is reported.
Device identification:
Microlife BP A100
Microlife AG, Espenstrasse 139, CH 9443, Widnau, Switzerland.
This device is a fully automatic, upper-arm type blood pressure monitor. Its measurement range spreads over 30–280 mmHg for BP.
The applied rigid conical cuff is suitable for arm circumferences ranging from 22.0 to 44.0 cm.
Thirty data memory. PAD: Pulse arrhythmia detection during measurement.
Method of BP measurement:
Oscillometric, corresponding to the Korotkoff method: phase I systolic, phase V diastolic.
Factors affecting accuracy: movement artifacts, arrhythmias
Validation studies:
EN 1060-4: 2004, ANSI/AAMI SP10:2002/(R)2008+Amendments
Service facilities:
Microlife distributors—refer to www.microlife.com or Microlife European Headquarter: Microlife AG, Espenstrasse 139, CH 9443, Widnau, Switzerland.
Rights and permissions
About this article
Cite this article
Bonso, E., Saladini, F., Zanier, A. et al. Accuracy of a single rigid conical cuff with standard-size bladder coupled to an automatic oscillometric device over a wide range of arm circumferences. Hypertens Res 33, 1186–1191 (2010). https://doi.org/10.1038/hr.2010.146
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2010.146
Keywords
This article is cited by
-
Current applications and limitations of European guidelines on blood pressure measurement: implications for clinical practice
Internal and Emergency Medicine (2022)
-
ClearSight™ finger cuff versus invasive arterial pressure measurement in patients with body mass index above 45 kg/m2
BMC Anesthesiology (2021)
-
In search of the optimal cuff for blood pressure measurement in people with severe obesity
Hypertension Research (2021)
-
Correlation of patient characteristics with arm and finger measurements in Asian parturients: a preliminary study
BMC Anesthesiology (2020)
-
Upper limb dimensions in adults presenting for elective surgery – implications for blood pressure measurement
BMC Anesthesiology (2020)
