
Abstract
Purpose: Blood phenylalanine monitoring is critical for the management of phenylketonuria. We compared three methods for measuring blood phenylalanine concentration: the amino acid analyzer, high-performance liquid chromatography with fluorometric detection, and tandem mass spectrometry.
Methods: We studied 22 female patients with phenylketonuria, ages 12–48 years, who attended our Metabolic Camp. Blood was collected into heparinized tubes (for analysis by the amino acid analyzer) or filter paper (for analysis by high-performance liquid chromatography with fluorometric detection and tandem mass spectrometry).
Results: Blood phenylalanine concentrations of plasma measured by the amino acid analyzer were significantly higher than those obtained from whole blood on filter paper by high-performance liquid chromatography (difference: 102 μM; 95% confidence interval: 23, 181) and tandem mass spectrometry (difference: 137 μM; 95% confidence interval: 58, 216). Phenylalanine concentrations from high-performance liquid chromatography and tandem mass spectrometry were not significantly different (P = 0.5).
Conclusions: When monitoring blood phenylalanine concentrations for dietary compliance, clinicians should be mindful of the method being used; analyses of whole blood on filter paper were consistently approximately 15% lower than analyses of plasma.
Similar content being viewed by others
Main
Phenylketonuria (PKU) is an inborn error of metabolism that results from a recessive genetic mutation, usually in the gene encoding phenylalanine hydroxylase, an enzyme responsible for the hydroxylation of the amino acid phenylalanine (Phe) to tyrosine (Tyr), which is an important intermediate in the production of neurotransmitters. If PKU goes untreated, Phe metabolites accumulate and neurotransmitters decrease, leading to mental retardation, behavior disorders, and seizures. However, these negative effects can be successfully prevented with dietary treatment, if it is initiated during the first few days of life, so all states now include PKU in their newborn screening panels.
Although there are no universal guidelines, a generally accepted approach to the management of PKU is a strict diet including the amount of intact protein needed to maintain blood Phe concentrations in the treatment range and supplementation with a Phe-free metabolic formula (i.e., medical food) such that blood Phe concentrations do not exceed 360 μM (6 mg/dL; to convert μM to mg/dL, divide by 60) at least through age 6.1 Lower Phe concentrations have been associated with normal cognitive abilities in adolescents and adults, indicating that optimal outcomes may be obtained when Phe levels are maintained at 120–360 μM through age 12 and 120–900 μM thereafter.2 Strict control of blood Phe concentration is also critical during pregnancy; a child born to a mother whose PKU is not under metabolic control can suffer mental retardation, microcephaly, and congenital heart failure.3
Aspiring to lifelong dietary compliance means a critical need for simple, rapid, and accurate methods of monitoring blood Phe concentrations. A simple screening method for PKU in newborns, the Guthrie bacterial inhibition assay,4 has been in use for over four decades. Since then, several new methods have been developed, including the amino acid analyzer (AAA), fluorometry,5 high-performance liquid chromatography (HPLC),6,7 and tandem mass spectrometry (MS/MS).8,9 These new techniques have proved vital to improving the accuracy and speed at which newborn screening can be done,10,11 but few studies have examined the validity of these methods for quantitative analysis of the absolute blood Phe concentrations required for patient monitoring.
Patients with PKU differ with regard to their amount of active enzyme, taste preferences for medical foods, and willingness to comply with a prescribed diet. All these factors make treatment highly individualized and monitoring critical. At the Emory University Division of Medical Genetics, we routinely see patients with PKU at metabolic clinics and a yearly summer camp, where blood is drawn and analyzed by AAA. In between these visits, patients perform fingerpricks at home, spot their blood on filter paper, and mail the sample to our clinic where it is analyzed by HPLC or, more recently, by MS/MS. Because the same patient is likely to have their blood analyzed by AAA and either HPLC or MS/MS, or possibly by all three of the methods currently used in our laboratories, we were interested in comparing the blood Phe concentrations obtained from these three methods. Thus, our objective was to analyze how the three methods (AAA of plasma and HPLC and MS/MS of filter paper whole blood spots) compare for monitoring blood Phe concentrations.
MATERIALS AND METHODS
Study participants
The Metabolic Camp for Girls at Emory University was created in 1994 to address the needs of adolescents who must cope with maintaining a restrictive diet and desirable blood Phe concentration.12 Adolescent girls were targeted first, because of the potentially detrimental effects of poor metabolic control on their offspring; our newer camps have been broadened to include women of various ages. Campers spend a week living in a house on campus with researchers and metabolic nutritionists who serve as “camp counselors.” Camp activities include PKU and diet education, cooking classes, medical food preparation, sampling of new supplements, and social outings. We obtained data for this analysis from participants in a weeklong 2004 camp: 25 girls and women aged 12–48 years.
Blood samples
On the first and last mornings of camp, participants visited Emory University's General Clinical Research Center (GCRC), where their heights and weights were measured. Blood was collected (2–3 mL) into a heparinized tube for analysis by AAA, and spotted directly onto filter paper from blood collection tubing for analysis by HPLC with fluorometric detection wand MS/MS. Parents (when a camper was younger than 18 years) or campers gave informed consent prior to the camp, and all data collection was approved by the Institutional Review Board at Emory University.
Plasma amino acid analysis by the AAA
We used a Beckman 6300 AAA equipped with an in-line colorimetric detector for amino acids analysis, as described previously13 with minor modifications. Plasma samples were deproteinized with an equal volume of 6% sulfosalicylic acid, and 400 μL of supernatant was mixed with 500 μL of Lithium B buffer and 100 μL of 0.25 mM S-aminoethylcysteine (SAEC) before analysis. The sample was injected onto a Beckman high-performance cation-exchange column (10 × 0.4 cm), and the free amino acids were separated using a combination of Beckman Coulter's lithium buffers A, D, E, and F (pH range from 2.9 to 3.9) of variable ionic strength and temperature program. Amino acids were then measured colorimetrically at wavelengths 570 and 440 nm after postcolumn derivatization with ninhydrin. Beckman standard mixture was used as calibrator. The Beckman System Gold software was used to identify and quantify the amino acids present in the sample based on their respective retention times and absorbance values.
Dried blood spots amino acid analysis by HPLC with fluorometric detection
The amino acid chemistry AccQTag (Waters Corporation, Milford, MA) was used for HPLC analysis, as described previously14 with modifications. A 3-mm diameter circle was punched out of filter paper containing the blood sample and extracted with 50 μL of a 70%-ethanol solution containing 5 μM (Br)2 L-Tyr (an internal standard) for 20 minutes via sonication. After centrifugation, 20 μL supernatant was transferred to another tube and derivatized with AccQFluor (Waters Corporation) reagent (6-aminoquinolyl-N-hydroxysuccinimidyl carbamate) at 55°C for 10 minutes to yield stable products that fluoresced at 395 nm. The Waters 2690 Separations Module with the Waters 2475 Fluorescence Detector was used for HPLC analysis. The derivatized samples were separated on a Waters AccQTag column at 37°C with a flow rate of 1 mL/minute. Mobile phase A consisted of AccQTag eluent A concentrate (PN: WAT052890)/water (1:10, v/v), mobile phase B was HPLC-grade acetonitrile, and mobile phase C was HPLC-grade water. Gradient conditions were initial = 100% A; 0.02 minutes = 86% A and 14% B; 3 minutes = 85% A and 15% B; 6 minutes = 79% A and 21% B; 9 minutes = 60% B and 40% C; and 12 minutes = 100% A, followed by 5 minutes equilibration with initial mobile phase (100% A). The emission and excitation wavelengths of the fluorescence detector were set at 250 and 395 nm, respectively. Waters Empower software was used for data analysis.
Dried blood spots amino acids analysis by tandem MS/MS
A 3-mm diameter circle was punched out of filter paper containing the blood sample and extracted with 100 μL of methanol containing stable isotope-labeled amino acid internal standards for 20 minutes via sonication. After evaporation of the solvent, amino acids were butylated with 3 N butanolic HCL for 15 minutes at 65°C. After evaporation to dryness, the samples were redissolved to 100 μL of mobile phase (80% acetonitrile). Micromass Quattro micro tandem mass spectrometer with Waters 2795 HPLC system was used for MS/MS analysis. LC flow rate was programmed with initial flow rate = 0.15 mL/minute, 0.12 minutes = 0.04 mL/minute, 1.1 minutes = 0.6 mL/minute, and 1.2 minutes = 0.15 mL/minute, followed by 0.8 minutes equilibration with initial flow rate for the next injection. Neutral loss of 102 in positive electrospray ionization mode detected L-Phe and L-Tyr. Mass spectrometer parameters were capillary voltage at 3.5 kV and the cone voltage at 35 V, and the collision energy was 25 V. The collision gas was argon. The intensity of L-Phe and L-Tyr were compared to their stable isotope-labeled internal standards. NeoLynx software was used for data analysis.
Dietary assessment
Campers completed 3-day food records for the 3 days immediately prior to the first day of camp, which we then analyzed with the Ross AAA software program (version 3.1, 1997, Ross Products Division, Columbus, OH).
Statistical analysis
SAS (version 9.1, SAS Institute, Cary, NC) was used for all statistical analysis. We excluded three campers for incomplete data (they had early morning flights and left campus before visiting the GCRC for measurements and blood draws), giving us a final sample size of n = 22. For each of the three methods, all samples were analyzed in duplicate, and the average was used. To compare the three methods, we calculated the difference in least-squares means (PROC MIXED in SAS) and created Bland-Altman difference plots.15 P < 0.05 was considered significant.
RESULTS
Among the 22 female campers, mean age was 20 years and mean BMI was 24.9 kg/m2 (Table 1). Seven campers were classified as overweight or obese (BMI ≥ 25 kg/m2). Upon arrival at camp, mean energy and protein intake were 1674 kcal/day and 59 g/day, and intake of Phe and Tyr were 9.9 and 82.4 mg/kg/day, respectively.
The largest difference of least-squares means when comparing the three methods was between AAA and MS/MS, with mean Phe concentrations from AAA approximately 137 μM higher than those from MS/MS (Table 2). Results from AAA were also significantly higher than those obtained from HPLC (102 μM). No significant difference was found between mean Phe concentrations analyzed by HPLC and MS/MS.
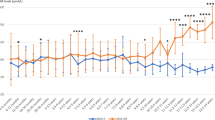
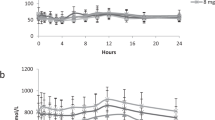
In our Bland-Altman figures, we plotted percent difference of Phe concentrations against average Phe concentrations. Phe concentrations obtained from AAA were on average 12% higher than those obtained from HPLC (Fig. 1); there appears to be less of a difference at lower concentrations of Phe. Phe concentrations obtained from AAA were on average 19% higher than those obtained from MS/MS (Fig. 2). Although there was no significant difference in Phe concentrations obtained from HPLC and MS/MS, the difference plot does reveal that on average measures were approximately 5% higher for HPLC (Fig. 3). The figure suggests that any difference is slightly greater at lower concentrations of Phe.

Bland-Altman plot of the percent difference in phenylalanine concentration (amino acid analyzer–high-performance liquid chromatography) versus the average concentration of phenylalanine determined by the two methods. Mean percent difference is indicated by the solid line and 95% limits by the dashed lines.

Bland-Altman plot of the percent difference in phenylalanine concentration (amino acid analyzer–tandem mass spectrometry) versus the average concentration of phenylalanine determined by the two methods. Mean percent difference is indicated by the solid line and 95% limits by the dashed lines.

Bland-Altman plot of the percent difference in phenylalanine concentration (high-performance liquid chromatography–tandem mass spectrometry) versus the average concentration of phenylalanine determined by the two methods. Mean percent difference is indicated by the solid line and 95% limits by the dashed lines.
DISCUSSION
We found meaningful differences in blood Phe concentrations as measured by AAA, HPLC, and MS/MS. AAA analysis of plasma gave the highest measures for blood Phe concentrations; HPLC and MS/MS, both of which made use of blood samples from filter paper, did not differ from one another statistically, and Phe concentrations were consistently about 12% lower for HPLC and 19% lower for MS/MS compared with AAA. The concentrations of blood Phe obtained via the three methods differ enough to have a real clinical impact, since the different values would likely trigger distinct adjustments in diet or metabolic foods by a clinician or metabolic dietician, particularly at higher Phe concentrations.
In this analysis, we compared three methods using blood samples (plasma or filter paper) prepared and analyzed as is done for Phe concentration monitoring in our laboratories; we did not compare analyses of plasma versus whole blood on filter paper for the same method. Furthermore, our filter paper blood samples were spotted from the venous blood sample taken from each camper and not from a fingerprick; therefore, these samples are not perfectly representative of ones that would be mailed to us for routine monitoring. We elected to use the venous samples only to avoid unnecessary stress to our campers from extra sticks, as well as to ensure complete and consistent saturation of the filter paper with blood.
The differences we found in Phe concentration were more likely due to the form of the blood sample than to the method of analysis. As explained earlier, our samples differ in their method of extraction: we used deproteination to produce free amino acids in plasma for analysis by AAA, whereas Phe was extracted directly into ethanol or methanol from whole blood on filter paper for analysis by HPLC or MS/MS, respectively. The volume of blood obtained from a dried filter paper blood spot can vary depending on the hematocrit, concentration of hemoglobin, and center versus periphery punch.16,17 We unearthed very little research comparing quantification of Phe concentrations from samples of plasma versus whole blood on filter paper with which to compare our results. Allard et al.18 found that Phe concentrations from MS/MS of whole blood on filter paper were approximately 10% lower than AAA analysis of both plasma and whole blood on filter paper. The difference between AAA of plasma and MS/MS of filter paper is similar to our own findings; however, they did not find a difference in Phe concentrations when analyzing plasma versus dried blood spots with the AAA (mean percent difference of 0.6%), which contradicts our hypothesis that the results are likely due to differences in the blood sample rather than in the method of analysis. Our findings are more consistent with those of Dale et al.,19 who found higher Phe concentrations in the HPLC analysis of plasma compared to dried blood spots.
Our analysis was strengthened by a relatively large sample of girls and women with PKU from whom fasting blood samples were collected and spotted directly onto filter paper at two time points by trained phlebotomists at the General Clinical Research Center. Our results underscore the need for those involved in monitoring Phe concentrations to be as aware of the methodology used as the results obtained. More research is needed to compare the quantification of Phe concentrations from plasma versus whole blood on filter paper using these different methodologies; a better understanding of differences in analytical methods for Phe monitoring is essential to the development of guidelines for clinicians and metabolic nutritionists who work with PKU patients.
References
Wappner R, Cho S, Kronmal RA, Schuett V, et al. Management of phenylketonuria for optimal outcome: a review of guidelines for phenylketonuria management and a report of surveys of parents, patients, and clinic directors. Pediatrics 1999; 104: e68.
Phenylketonuria: Screening and Management: NIH Consensus Statement; October 16–18, 2000; 17: 1–27.
Rouse B, Azen C, Koch R, Matalon R, et al. Maternal Phenylketonuria Collaborative Study (MPKUCS) offspring: facial anomalies, malformations, and early neurological sequelae. Am J Med Genet 1997; 69: 89–95.
Guthrie R, Susi A . A simple phenylalanine method for detecting phenylketonuria in large populations of newborn infants. Pediatrics 1963; 32: 338–343.
Gerasimova NS, Steklova IV, Tuuminen T . Fluorometric method for phenylalanine microplate assay adapted for phenylketonuria screening. Clin Chem 1989; 35: 2112–2115.
Roesel RA, Blankenship PR, Hommes FA . HPLC assay of phenylalanine and tyrosine in blood spots on filter paper. Clin Chim Acta 1986; 156: 91–96.
Rudy JL, Rutledge JC, Lewis SL . Phenylalanine and tyrosine in serum and eluates from dried blood spots as determined by reversed-phase liquid chromatography. Clin Chem 1987; 33: 1152–1154.
Chace DH, Sherwin JE, Hillman SL, Lorey F, et al. Use of phenylalanine-to-tyrosine ratio determined by tandem mass spectrometry to improve newborn screening for phenylketonuria of early discharge specimens collected in the first 24 hours. Clin Chem 1998; 44: 2405–2409.
Rashed MS, Ozand PT, Bucknall MP, Little D . Diagnosis of inborn errors of metabolism from blood spots by acylcarnitines and amino acids profiling using automated electrospray tandem mass spectrometry. Pediatr Res 1995; 38: 324–331.
Ceglarek U, Muller P, Stach B, Buhrdel P, et al. Validation of the phenylalanine/tyrosine ratio determined by tandem mass spectrometry: sensitive newborn screening for phenylketonuria. Clin Chem Lab Med 2002; 40: 693–697.
Schulze A, Lindner M, Kohlmuller D, Olgemoller K, et al. Expanded newborn screening for inborn errors of metabolism by electrospray ionization-tandem mass spectrometry: results, outcome, and implications. Pediatrics 2003; 111: 1399–1406.
Singh RH, Kable JA, Guerrero NV, Sullivan KM, et al. Impact of a camp experience on phenylalanine levels, knowledge, attitudes, and health beliefs relevant to nutrition management of phenylketonuria in adolescent girls. J Am Diet Assoc 2000; 100: 797–803.
Hommes FA . Techniques in diagnostic human biochemical genetics: a laboratory manual. New York: John Wiley, 1991.
Cohen SA, Michaud DP . Synthesis of a fluorescent derivatizing reagent, 6-aminoquinolyl-N-hydroxysuccinimidyl carbamate, and its application for the analysis of hydrolysate amino acids via high-performance liquid chromatography. Anal Biochem 1993; 211: 279–287.
Bland JM, Altman DG . Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: 307–310.
O'Broin SD, Kelleher BP, Gunter E . Evaluation of factors influencing precision in the analysis of samples taken from blood spots on filter paper. Clin Lab Haematol 1995; 17: 185–188.
Adam BW, Alexander JR, Smith SJ, Chace DH, et al. Recoveries of phenylalanine from two sets of dried-blood-spot reference materials: prediction from hematocrit, spot volume, and paper matrix. Clin Chem 2000; 46: 126–128.
Allard P, Cowell LD, Zytkovicz TH, Korson MS, et al. Determination of phenylalanine and tyrosine in dried blood specimens by ion-exchange chromatography using the Hitachi L-8800 analyzer. Clin Biochem 2004; 37: 857–862.
Dale Y, Mackey V, Mushi R, Nyanda A, et al. Simultaneous measurement of phenylalanine and tyrosine in phenylketonuric plasma and dried blood by high-performance liquid chromatography. J Chromatogr B Analyt Technol Biomed Life Sci 2003; 788: 1–8.
Acknowledgements
We thank all of the Metabolic Camp campers for their willingness to participate in this study. We also thank Mary Jane Kennedy for coordinating this study, Tisa Harper and Hong Wang for assistance with analysis of the blood samples, Emory University's General Clinical Research Center, and MetGen, Inc.
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclosure: The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Gregory, C., Yu, C. & Singh, R. Blood phenylalanine monitoring for dietary compliance among patients with phenylketonuria: comparison of methods. Genet Med 9, 761–765 (2007). https://doi.org/10.1097/GIM.0b013e318159a355
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1097/GIM.0b013e318159a355
Keywords
This article is cited by
-
Phenylketonuria
Nature Reviews Disease Primers (2021)
-
Dried blood spot versus venous blood sampling for phenylalanine and tyrosine
Orphanet Journal of Rare Diseases (2020)
-
The complete European guidelines on phenylketonuria: diagnosis and treatment
Orphanet Journal of Rare Diseases (2017)
-
Efficacy, safety and population pharmacokinetics of sapropterin in PKU patients <4 years: results from the SPARK open-label, multicentre, randomized phase IIIb trial
Orphanet Journal of Rare Diseases (2017)
-
Correlation of age‐specific phenylalanine levels with intellectual outcome in patients with phenylketonuria
Journal of Inherited Metabolic Disease (2011)
