
Abstract
Purpose: To further assess the frequency of subtelomeric aberrations in a selected population and to examine the feasibility of a clinical testing.
Methods: Patients were selected based on the following criteria: (1) mental retardation (IQ < 70) or developmental delay with dysmorphic features; (2) a normal karyotype at the level of resolution of 450 to 500 bands; and (3) exclusion of other possible etiologies by a full genetic assessment and relevant tests. Fluorescence in situ hybridization (FISH) was performed using multiple subtelomeric probes. Abnormal findings were confirmed by 24-color spectral karyotyping or FISH with a specific subtelomeric probe, and family studies were carried out to determine inheritance.
Results: Clinically significant aberrations were detected in 6 of 150 proband patients (4%), while deletion of the 2q subtelomeric region appeared to be a common variant (6%).
Conclusions: FISH with multiple subtelomeric probes is a valuable clinical test for establishing a definitive diagnosis for patients with unexplained mental retardation/developmental disorders.
Similar content being viewed by others


Main
Approximately 1 of 500 phenotypically normal individuals have a visible balanced chromosomal rearrangement when analyzed at the resolution level of 400 bands.1 Empiric data suggest that the least unbalanced gametes are the most likely to produce a viable chromosomally abnormal conceptus.2 The regions near the chromosome ends are usually gene rich,3 and many cryptic translocations involving the terminal bands have been described.4–14 A complete set of probes specific to each human subtelomeric region was isolated in 1996.15 Soon after, a FISH procedure using 41 subtelomeric probes for all 24 different chromosomes was developed.16,17 FISH with multiple subtelomeric probes has been proven to be useful in the study of patients with idiopathic mental retardation. However, the reported frequency of subtelomeric abnormalities in this population has been inconsistent.18–25 This study is to further assess the frequency of subtelomeric aberrations in patients with developmental disabilities and to determine the feasibility of using this technology in clinical testing.
MATERIALS AND METHODS
Patients
All patients were selected by clinical geneticists according to the following criteria: (1) moderate to severe mental retardation (IQ < 70) or developmental delay with dysmorphic features and/or congenital malformations; (2) a normal karyotype at the level of resolution of >450 bands; (3) exclusion of other possible etiologies by a full genetic assessment and relevant tests, for example, Fragile X syndrome being excluded by DNA testing or a microdeletion syndrome, if suspected, being excluded by FISH with specific DNA probes. A total of 150 patients were entered into this study.
FISH with Cytocell Multiprobe-T system
The Cytocell Multiprobe-T system (Cytocell, Ltd., Oxfordshire, UK) were used in this study. The system includes a template slide and a hybridization device containing 41 probes specific to all the subtelomeric regions of human chromosomes, with the exception of the short arms of chromosomes 13, 14, 15, 21, and 22, as they lack unique sequences. There are 24 hybridization surfaces (bosses) in the device containing probes for each of the chromosome arms, allowing simultaneous hybridization of all 41 probes to the template chromosome slide.16 The short arm probes are directly labeled with FITC (green) and the long arm probes with Texas Red (red). The protocols recommended by the manufacturer were followed with slight modifications, according to the results of each particular batch of probes and devices. For each chromosome, 5 to 10 metaphases were analyzed. More than 10 cells were analyzed for the particular chromosome if a deletion was detected.
Spectral karyotyping
Spectral karyotyping (SKY) was performed as previously described26 for the patient and the parents when a rearrangement was detected by FISH using the Multiprobe-T system.
FISH with Vysis probes
FISH was performed using individual subtelomeric probes produced by Vysis, Inc. (Downers Grove, IL) for the patient and the parents when a deletion was detected. The protocols recommended by the manufacturer were used.
High resolution G-banding
Chromosomes were re-examined at a higher level of resolution for the abnormal cases if the previous analysis was at a resolution lower than 500 bands.
Clinical and family studies
The clinical features of the patients with subtelomeric aberrations were recorded. For the cases with a 2q deletion, parents and other family members were examined and their phenotypes were compared.
RESULTS
Frequency
Subtelomeric alterations were detected in 15 of 150 proband patients (10%). Among the abnormal cases, four had an unbalanced cryptic rearrangement (2.7%), two had a 1ptel deletion (1.3%), and nine had a 2qtel deletion (6%). The frequency of subtelomeric aberrations was 4% in this study population when the cases with 2qtel deletion were excluded.
Aberrations and clinical features
The karyotypes of the abnormal cases were described in combining the results of multi-telomere FISH, conventional G-banding analysis, SKY, and parental studies (Figs. 1 and 2). The abbreviated term tel was used in the nomenclature to represent the subtelomeric region. The loci for which probes were used17 were not included in the descriptions of aberrations except for the 2q deletion.

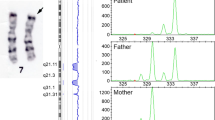
Two example cases showing the analysis of FISH using the Multiprobe-T system (green for ptel and red for qtel), SKY (each chromosome is shown with a display color on left and a classified color on right), and G-banding. (A) A partial metaphase of Case 2 showing normal hybridization patterns on both chromosomes 7 and additional signals (arrow) of 7ptel (green) on the der(18). (B) A partial metaphase of Case 2 showing a normal chromosome 18 and the der(18) with deletion of 18qtel (arrow). (C) A reciprocal translocation t(7;18)(ptel;qtel) detected by SKY in the mother of Case 2 and her normal G-banded chromosomes 7 and 18 at the level of >550 bands. (D) A partial metaphase of Case 3 showing a normal chromosome 4 and the der(4) with 4ptel deletion (arrow). (E) A partial metaphase of Case 3 showing normal hybridization patterns on both chromosomes 12 and additional signals of 12qtel (red) on the der(4) (arrow). (F) SKY and G-banded chromosomes 4 and 12 of Case 3, with arrow indicating the translocated segment on the der(4) visualized by SKY and a questionable banding pattern at the level of >650 bands.

A metaphase of Case 5 showing deletion of 1ptel (arrow) detected by FISH using the Multiprobe-T system and normal G-banded chromosomes 1 at the level of >850 bands.
Case 1
46,XX. ish der(1)t(1;3)(qtel;qtel), representing a deletion of 1qtel and a partial trisomy of 3qtel. The der(1) was also detected by SKY, and the translocated segment was identified to be originating from chromosome 3. This 33-month-old girl was the only child of the couple and presented with severe developmental delay and a left occipitoparietal stroke. Both her birth weight and head circumference were on the 10th centile. She had multiple congenital malformations including cleft palate, mild talipes equinovarus, agenesis of the corpus callosum, tethered cord, and aqueductal stenosis with Chiari I malformation. Her dysmorphic features included squared forehead, bilateral epicanthal folds, anteverted nares, prominence over the metopic suture, oval-shaped left iris, smooth philtrum, deeply grooved tongue, unilateral fused lower central and lateral incisors, downturned corners of mouth, micrognathia, and lumbar lordosis. She also had seizures starting at 10 months. SKY for the father revealed a reciprocal translocation t(1;3)(qtel;qtel), which could not be identified by G-banding at the level of 550 bands. There was no family history of recurrent miscarriages or stillbirth.
Case 2
46, XX. ish der(18)t(7;18)(ptel;qtel), representing a deletion of 18qtel and a partial trisomy of 7ptel. The small segment translocated onto der(18) was clearly identified by SKY to be originating from chromosome 7. The patient presented at 18 years with profound mental retardation, severe growth restriction, failure to undergo puberty, and behavior problems. Her dysmorphic features included microcephaly, cleft palate, bilateral ptosis, hypertelorism, epicanthal folds, wide low nasal bridge, anteverted nares and downturned corners of the mouth, camptodactyly of the fingers, scoliosis, and bilateral talipes equinovarus. She also had pulmonary stenosis, wasting of the calf muscles, hypotonia, and severe periodontal disease. Hypothyroidism developed at age 15 years. SKY for the mother revealed a reciprocal translocation t(7;18)(ptel;qtel), which was not identifiable with G-banding analysis at the level of 550 bands. However, the mother did not have a history of recurrent miscarriages or stillbirths.
Case 3
46,XX. ish der(4)t(4;12)(ptel;qtel), representing a deletion of 4ptel and a partial trisomy of 12qtel. The derivative chromosome 4 was detected by SKY, but the origin of the translocated segment on the der(4) was too small to be identified with certainty. A subtle difference at the 4p terminal region was noted in a repeat G-banding analysis at the level of >650 bands. The patient was a newborn, delivered from a 29-year-old mother who had six previous first trimester losses and three other children with different partners. Amniocentesis was performed for intrauterine growth retardation, and a normal karyotype was reported. The baby presented with hypotonia, feeding difficulties, and dysmorphic features, including prominent eyes with heavy eyelids, epicanthal folds, downslanting eye fissures, telecanthus, relatively large mouth, short philtrum, prominent clitoris, and bowed tibias. These features are consistent with Pitt-Rogers-Danks syndrome or Wolf-Hirschhorn syndrome with clinical variations. The mother was suspected to be a carrier of a cryptic translocation, but she refused to have cytogenetic analysis. G-banding and SKY analysis of other two children showed normal results.
Case 4
46,XX. ish der(5)t(5;20)(ptel;ptel), representing a deletion of 5ptel and a partial trisomy of 20ptel. The small segment translocated onto the derivative 5 was also identified by SKY to be originating from chromosome 20. The patient was an 18-month-old girl, born to a 31-year-old mother through donor insemination. She presented with developmental delay and grossly dysmorphic features, including cleft lip and palate, flat occiput, and very long and narrow fingers. She also had tetralogy of Fallot, patent ductus arteriosus, motor and speech delay, jerky movements, and possible seizures. SKY showed a normal result in the mother. The sperm donor was not available for analysis.
Cases 5 and 6
46,XX. ish del(1)(ptel). Both had a de novo deletion in the subtelomeric region of 1p. Upon review of the G-banded karyotypes after FISH analysis, the deletion was not detectable in Case 5 but was questionable in Case 6 with G-banding at the level of 850 bands. Case 5 was 9 years old, and Case 6 was 5 years of age. Both had significant developmental delay, brachycephaly, hypotonia, severe speech delay, short stature, and a history of severe intrauterine growth retardation with a birth weight below the 5th centile. Case 5 had a head circumference on the 3rd centile when evaluated at 3 years. Similarly, the head circumference of Case 6 was on the 2nd centile at 4 years of age. Both patients also had a broad-based gait. These features are consistent in general with the phenotype described for patients with a 1p36 deletion.8
Cases 7 to 14
ish del(2)(qtel)(D2S2986-). The 2qtel deletion detected by the Multiprobe-T system was re-examined by FISH with the Vysis probe (VIJ yRM2112). In all the cases, FISH with the Vysis probe showed signals in both chromosomes 2. However, it was observed in one research site (London, ON) that the 2qtel signals on one chromosome 2 were much weaker than those on the other. Parental and family studies did not show a paternal or maternal transmission pattern suggestive of an imprinting locus. Family studies were completed for six cases. Three families had multiple members with mental retardation or learning disabilities. In these families, segregation of the del(2)(qtel) did not correlate with the phenotypes of the family members, i.e., some individuals with a del(2)(qtel) were phenotypically normal, while some individuals lacking a del(2qtel) had mental retardation or learning disabilities. In three other families, the del(2)(qtel) was inherited from a phenotypically normal parent. The clinical features of the probands were extremely variable. For example, one patient had mild retardation, slight asymmetry of the face, and large protruding ears without other significant dysmorphism, while the other who inherited the del(2qtel) from a phenotypically normal father showed profound retardation, coarse facial features, and multiple congenital anomalies.
DISCUSSION
Cases with cryptic chromosomal translocations have been reported.4–14 Efforts have been made to establish strategies for screening cryptic subtelomeric rearrangements, because this type of aberration is considered to be an important cause of unexplained mental retardation.6,8,15 A FISH strategy using multiple subtelomeric probes has been developed recently.16 However, by using the new FISH technique, the detection rates have ranged from <1% to as high as 23% of the patients studied.18–25 Variable population size and different criteria used for selecting patients have been considered to be the explanation for the different estimates.28 Three previous studies have included a large number of patients.18,22,27 Knight et al.18 studied 284 patients with moderate to severe idiopathic mental retardation and 182 patients with mild mental disability. The frequency of subtelomeric aberrations was estimated to be 7.4% in the first group and only 0.5% in the second. In a similar study, Vorsanova et al.22 found subtelomeric abnormalities in 8 of 209 patients (3.8%) with mild to severe mental retardation and congenital anomalies. Ballif et al.27 recently reported their detection of clinically significant subtelomeric alterations in 2.6% of cases with apparently normal karyotypes. However, the cases included in the report were submitted for a variety of clinical reasons instead of being selected for mental retardation. In our study, subtelomeric alterations were detected in 10% of the patients. When the deletion of 2qtel is excluded, the detection rate of clinically relevant abnormalities is 4%, which is quite similar to the reports described above.
A polymorphism at the 2q telomere was first identified by Macina et al.29 Deletion of 2qtel has been reported in study populations with a frequency ranging from 1.5% to 8.2%.19,23–25,27 When all the data are considered, the average prevalence of the 2qtel deletion is approximately 5%. In our study, 6% of the patients had the 2qtel deletion, and segregation analysis of the 2qtel deletion in relevant family members showed no correlation with mental retardation and other phenotypic anomalies. Our observations support the conclusion that the deletion of the locus D2S2986 in the 2qtel region detected by the current Cytocell Multiprobe-T system is a common variant. When a 2qtel deletion is detected, however, it is important to test the deletion by FISH using a second probe, such as the one from Vysis, and to test the parents to determine its inheritance. Without further studies, a clinically significant distal 2q deletion could be misinterpreted as a polymorphism or normal variant.
This report in combination with the other previously reported large study22 indicates that clinically significant subtelomeric aberrations are present in 3% to 5% of patients with unexplained mental retardation or developmental delay with dysmorphic features. This frequency is lower than that reported by Knight et al.18 in an earlier large study. However, all these studies have clearly shown that FISH with multiple subtelomeric probes is a valuable tool for a definitive diagnosis for some patients who had undergone many other types of clinical and genetic tests without a clear answer for their developmental problems.
It appears that a large proportion of subtelomeric aberrations are inherited from familial cryptic translocations.18,27 However, these families may not have a history of recurrent miscarriages or stillbirths due to small material size of rearrangement, for example, the Cases 1 and 2 in this study. For such families, the detection of a subtelomeric aberration in an abnormal child is the only means of identifying a carrier parent and enabling prenatal diagnosis for future pregnancies. This method also allows determination of the carrier status for the cryptic rearrangement in other family members.
In a previous study, we estimated the sensitivity of SKY to be within the range of 1 to 2 Mb in detecting interchromosomal rearrangements.26 In the current study, we also performed SKY analysis for the four cases with unbalanced rearrangements. In each case, SKY was successfully used to visualize the submicroscopic rearrangement, as well as the full cryptic translocation in the parent when available for analysis. Based on the level of resolution of chromosome banding and the sensitivity of SKY, it is estimated that the small segments involved in these cryptic translocations are in the range of 1 to 3 Mb in size (assuming 5 Mb/band at the level of 600 bands and rearrangement of a half band may not be visible with G-banding but detectable by SKY).
This and three other large studies18,22,27 have shown that in 3% to 7% of patients subtelomeric aberrations can be the cause of unexplained moderate to severe mental retardation or developmental delay with dysmorphism. Therefore, we consider FISH with multiple subtelomeric probes to be a valuable diagnostic tool that should be implemented in all clinical cytogenetics laboratories. Our study has also demonstrated the sensitivity of SKY in detecting submicroscopic rearrangements and its utility in family studies. Although subtelomeric deletions are not detectable, SKY may pick up other submicroscopic interchromosomal rearrangements such as insertions throughout the genome. Finally, we also stress the importance of using specific clinical criteria to select appropriate patients for these new techniques to be best used as diagnostic tools.30
References
Nora JJ, Fraser FC, Bear J, Greenberg CR, Paterson D, Warburton D . editors. Medical genetics, 4th ed. Malvern: Lea & Febiger, 1994.
Daniel A, Hook EB, Wulf G . Risks of unbalanced progeny at amniocentesis to carriers of chromosome rearrangements: data from United States and Canadian laboratories. Am J Med Genet 1989; 31: 14–53.
Saccone S, De Sario A, Della Valle G, Bernardi G . The highest gene concentrations in the human genome are in telomeric bands of metaphase chromosomes. Proc Natl Acad Sci USA 1992; 89: 4913–4917.
Altherr MR, Bengtsson U, Elder FF, Ledbetter DH, Wasmuth JJ, McDonald ME, Gusella JF, Greenberg F . Molecular confirmation of Wolf-Hirschhorn syndrome with a subtle translocation of chromosome 4. Am J Hum Genet 1991; 49: 1235–1242.
Kuwano A, Ledbetter SA, Dobyns WB, Emanuel BS, Ledbetter DH . Detection of deletions and cryptic translocations in Miller-Dieker syndrome by in situ hybridization. Am J Hum Genet 1991; 49: 707–714.
Wilkie AO . Detection of cryptic chromosomal abnormalities in unexplained mental retardation: a general strategy using hypervariable subtelomeric DNA polymorphisms. Am J Hum Genet 1993; 53: 688–700.
Ning Y, Rosenberg M, Biesecker LG, Ledbetter DH . Isolation of the human chromosome 22q telomere and its application to detection of cryptic chromosomal abnormalities. Hum Genet 1996; 97: 756–769.
Shapira SK, McCaskill C, Northrup H, Spikes AS, Elder FFB, Sutton VR, Korenberg JR, Greenberg F, Shaffer LG . Chromosome 1p36 deletion: the clinical phenotype and molecular characterization of a common newly delineated syndrome. Am J Hum Genet 1997; 61: 642–650.
Delneste D, Vamos E, Pierquin G, Hayez-Delatte F, Van Regemorter N . Need for search for cryptic translocation in parents with several children affected with MCA: report of a cryptic translocation (10;14) detected by FISH. Genet Couns 1998; 9: 97–102.
Ghaffari SR, Boyd E, Tolmie JL, Crow YJ, Trainer AH, Connor JM . A new strategy for cryptic telomeric translocation screening in patients with idiopathic mental retardation. J Med Genet 1998; 35: 225–233.
Precht KS, Lese CM, Spiro RP, Huttenlocher PR, Johnston KM, Baker JC, Christian SL, Kittikamron K, Ledbetter DH . Two 22q telomere deletions serendipitously detected by FISH. J Med Genet 1998; 35: 939–942.
Bacino CA, Kashork CD, Davino NA, Shaffer LG . Detection of a cryptic translocation in a family with mental retardation using FISH and telomere region-specific probes. Am J Med Genet 2000; 92: 250–255.
Speleman F, Callens B, Logghe K, Van Roy N, Horsley SW, Jauch A, Verschraegen-Spae MR, Leroy JG . Subtelomeric familial translocation t(2;7)(q37;q35) leading to partial trisomy 7q35->qter: molecular cytogenetic analysis and clinical phenotype in two generations. Am J Med Genet 2000; 93: 349–354.
Leppig KA, Ball S, Au K, Opheim KE, Norwood T . Familial cryptic (20;21) translocation identified by in situ hybridization technologies. Am J Med Genet 2000; 93: 273–277.
National Institutes of Health, Institute of Molecular Medicine Collaboration, Ning Y, Roschke A, Smith AC, Macha M, Precht K, et al A complete set of human telomeric probes and their clinical applications. Nat Genet 1996; 14: 86–89.
Knight SJL, Horsley SW, Regan R, Lawrie NM, Maher EJ, Cardy DLN, Flint J, Kearney L . Development and clinical application of an innovative fluorescence in situ hybridization technique which detects submicroscopic rearrangements involving telomeres. Eur J Hum Genet 1997; 5: 1–8.
Knight SJL, Lese CM, Precht KS, Kuc J, Ning Y, Lucas S, Regan R, Brenan M, Nicod A, Lawrie NM, Cardy DLN, Nguyen H, Hudson TJ, Riethman HC, Ledbetter DH, Flint J . An optimized set of human telomere clones for studying telomere integrity and architecture. Am J Hum Genet 2000; 67: 320–332.
Knight SJL, Regan R, Nicod A, Horsley SW, Kearney L, Homfray T, Winter RM, Bolton P, Flint J . Subtle chromosomal rearrangements in children with unexplained mental retardation. Lancet 1999; 354: 1676–1681.
Anderlid B, Anneren G, Blennow E, Nordenskjold M . Subtelomeric rearrangements detected by FISH in patients with idiopathic mental retardation. Am J Hum Genet 1999; 65( suppl): A67.
Joyce CA, Hart HH, Fisher AM, Browne CE . Use of subtelomeric probes to detect abnormalities in patients with idiopathic mental retardation and characterize rearrangements at the limit of cytogenetic resolution. J Med Genet 1999; 36( suppl): S16.
Lamb AN, Lytle CH, Aylsworth AS, Powell CM, Rao KW, Hendrickson M, Carey JC, Opitz JM, Viskochil DH, Leonard CO, et al. Low proportion of subtelomeric rearrangements in a population of patients with mental retardation and dysmorphic features. Am J Hum Genet 1999; 65( suppl): A169.
Vorsanova SG, Koloti D, Sharonin VO, Sloviev V, Yurov YB . FISH analysis of microaberrations at telomeric and subtelomeric regions in chromosomes of children with mental retardation. Am J Hum Genet 1998; 63( suppl): A154.
Viot G, Gosset P, Fert S, Prieur M, Turleau C, Raoul O, De Blois MC, Lyonnet S, Munnich A, Vekemans M . Cryptic subtelomeric rearrangements detected by FISH in mentally retarded and dysmorphic patients. Am J Hum Genet 1998; 63( suppl): A10.
Jalal SM, Harwood A, Anderson M, Lorentz C, Law M, Lindor N, Karnes P, Kulharya A, Sekhon G, Michels V . Screening for subtle structural anomalies by use of subtelomere specific FISH probe set. Am J Hum Genet 2000; 67( suppl): A770.
Huang XL, Wyandt HE, Milansky JM . Subtelomeric testing for cryptic chromosomal rearrangements in 68 patients with idiopathic mental retardation and dysmorphology. Am J Hum Genet 2000; 67( suppl): A853.
Fan YS, Siu VM, Jung JH, Xu J . Sensitivity of multiple color spectral karyotyping in detecting small interchromosomal rearrangements. Genet Test 2000; 4: 9–14.
Ballif BC, Kashork CD, Shaffer LG . The promise and pitfalls of telomere region-specific probes. Am J Hum Genet 2000; 67: 1356–1359.
Knight SJL, Flint J . Perfect endings: a review of subtelomeric probes and their use in clinical diagnosis. J Med Genet 2000; 37: 401–409.
Macina RA, Negorev DG, Spais C, Ruthig LA, Hu XL, Riethman HC . Sequence organization of the human chromosome 2q telomere. Hum Mol Genet 1994; 3: 1847–1853.
de Vries BB, White SM, Knight SJ, Regan R, Homfray T, Young ID, Super M, McKeown C, Splitt M, Quarrell OW, Trainer AH, Niermeijer MF, Malcolm S, Flint J, Hurst JA, Winter RM . Clinical studies on submicroscopic subtelomeric rearrangements: a checklist. J Med Genet 2001; 38: 145–150.
Acknowledgements
This work was partially supported by London Health Sciences Center Internal Research Fund (grant IRF-046-00) and Internal Research Grant Fund of the Child Health Research Institute, University of Western Ontario (grant R3098A01). The Department of Pathology, University of Western Ontario, also provided partial support for research fellow Dr. Y. Zhang.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Fan, YS., Zhang, Y., Speevak, M. et al. Detection of submicroscopic aberrations in patients with unexplained mental retardation by fluorescence in situ hybridization using multiple subtelomeric probes. Genet Med 3, 416–421 (2001). https://doi.org/10.1097/00125817-200111000-00007
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1097/00125817-200111000-00007
Keywords
This article is cited by
-
The 2q37-deletion syndrome: an update of the clinical spectrum including overweight, brachydactyly and behavioural features in 14 new patients
European Journal of Human Genetics (2013)
-
"Familial" versus "sporadic" intellectual disability: contribution of subtelomeric rearrangements
Molecular Cytogenetics (2012)
-
Subtelomeric rearrangements in Polish subjects with intellectual disability and dysmorphic features
Journal of Applied Genetics (2010)
-
Subtelomeric rearrangements in idiopathic mental retardation
The Indian Journal of Pediatrics (2005)
-
A 4q35.2 subtelomeric deletion identified in a screen of patients with co-morbid psychiatric illness and mental retardation
BMC Medical Genetics (2004)
