
Abstract
Purpose
To ascertain ophthalmology trainee confidence in managing posterior capsule rupture (PCR) and vitreous loss.
Methods
An electronic survey was distributed to ophthalmology trainees in a single UK postgraduate training Deanery. Data collected included the stage of training, number of completed cataract operations, cumulative PCR rate, number of PCRs personally managed by the trainee, previous vitrectomy experience during vitreoretinal rotations, and attendance at advanced phacoemulsification courses. Trainees self-evaluated their confidence in managing PCR with vitreous loss, including the management of specific aspects of the procedure.
Results
Across training grades, only 9.1% (2/22) felt confident managing PCR without senior support. Respondents were most confident with fluidic parameters and IOL considerations, but 77.3% (17/22) lacked confidence in avoiding a dropped nucleus. Eleven respondents had completed >350 cases (mean 576; range 383–1087). In this subgroup, mean cumulative PCR rate was 2.1% (range 0.9–4.9%), and trainees personally managed a mean 3.5 cases of PCR (range 1–7). Only 18.2% felt they could manage PCR and vitreous loss without senior support, and 45.5% stated they were not confident in avoiding a dropped nucleus. The most experienced trainee (1087 cases) had personally managed PCR just six times, and three trainees with >350 cases had only managed PCR once each.
Conclusions
The Royal College of Ophthalmologists’ requirement of 350 completed cases appears insufficient for independent cataract surgery, as opportunities to manage complications as a trainee are scarce. A competency-based assessment framework may be preferable, with a more targeted approach to training incorporating surgical simulation within the formal curriculum.
Similar content being viewed by others


Introduction
Rupture of the posterior lens capsule is a feared but common adverse event during cataract surgery. Posterior capsule rupture (PCR) increases the risk of poor anatomical and functional outcome due to complications including postoperative uveitis, raised intraocular pressure, cystoid macular oedema, retinal detachment, and endophthalmitis.1, 2 Sparrow et al3 concluded that PCR was powerfully associated with visual loss (OR=5.74). In a study by Ti et al,2 significantly fewer patients achieved Snellen BCVA of 20/40 (6/12) or better when their surgery was complicated by PCR (93.8% vs 98.5%, P<0.001). Importantly, cases complicated by PCR and dropped nucleus had significantly worse visual outcomes than those complicated by PCR alone (83.1% vs 94.8% achieving BCVA 20/40, P<0.001).2 Thus, it is essential that cataract surgeons operating independently can manage PCR confidently and competently, as early recognition and effective management increases the likelihood of a successful patient outcome.
In order to be eligible for the certificate of completion of training (CCT), alongside criteria unrelated to cataract surgery, the Royal College of Ophthalmologists (RCOphth) states that UK-based ophthalmic specialist trainees (specialty registrars; StR) must complete at least 350 cataract operations.4 The UK rate of PCR, including all grades of surgeon, with or without vitreous loss, has been estimated as 1.95%.1 Inverse correlation exists between PCR rate and grade of surgeon.5 While PCR is relatively common, trainees may have limited opportunity to manage it themselves. In the event of PCR, the supervising surgeon will usually take over from an inexperienced trainee, meaning the junior may observe but not gain hands-on experience. As trainees progress and become more proficient, the risk of complications reduces.5 By the end of ophthalmic specialist training, trainees may only have dealt with a small number of cataract-related complications. This raises the concern that senior trainees may be inadequately prepared for independent practice as consultants performing cataract surgery.
The aim of this study was to ascertain how confident ophthalmic trainees feel regarding managing PCR, with reference to stage of training and number of completed cases. We were also interested in whether formal courses in advanced phacoemulsification or hands-on experience with vitreoretinal (VR) surgery helped trainees feel more confident.
Subjects and methods
An electronic, anonymised survey was distributed via Survey Monkey in April 2015 to all ophthalmic specialty registrars within the Health Education Wessex Local Education and Training Board (‘Deanery’). Survey completion was voluntary and non-incentivised. Only one survey response per StR was permitted. The survey was divided into three sections (Table 1), with space after each question for free text comments. Survey results were collated via Survey Monkey and extracted for further statistical analysis using IBM SPSS version 21 (IBM Corporation, New York, NY, USA).
Results
The survey was completed by 22 of 28 trainees, a response rate of 78.6%. The mix of training grades is shown in Figure 1. One respondent had recently received their CCT but was still practising as a final year trainee (StR7) prior to leaving the training programme.

Survey respondents by training grade.
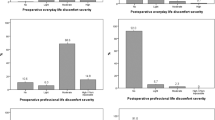
Overall, just 9.1% (2/22) respondents felt that they could complete a case involving PCR without senior support. 40.9% (9/22) could manage the situation with senior advice, scrubbed or unscrubbed. 13.6% (3/22) could only manage with their supervisor scrubbed and assisting, whereas 36.4% (8/22) stated they would need urgent supervisor take over.
Trainees were most comfortable with deciding what fluidic parameters were required, with 59.1% (13/22) feeling quite confident or very confident. 31.8% (7/22) were not that confident and would need considerable senior support, and 9.1% (2/22) were not confident at all.
With decisions regarding IOL placement, 50.0% trainees (11/22) were quite confident or very confident. 40.9% (9/22) were not that confident and would need considerable senior support, and 9.1% (2/22) were not confident at all.
Preventing a dropped nucleus was the most concerning aspect for trainees. Seventeen of 22 (77.3%) stated they were either not confident at all, or not that confident and would need considerable senior support. Only 9.1% (2/22) were very confident, and a further 13.6% (3/22) felt quite confident and could manage with minimal senior support.
Eight respondents (36.4%), all of whom StR5 or above, had attended an advanced phacoemulsification course (RCOphth, n=5; Alcon Academy, n=2; Bausch & Lomb, n=1). Respondents who had not attended a course were generally more junior and reported less confidence in managing PCR and vitreous loss. All eight respondents who had attended an advanced phacoemulsification course reported feeling either quite confident or very confident with fluidics and IOL considerations. In terms of preventing a dropped nucleus, 62.5% (5/8) were either quite confident or very confident, with 37.5% (3/8) stating they were not that confident and would need considerable senior support.
Eighteen of 22 (81.8%) respondents had undertaken at least one training rotation in VR surgery, most commonly between StR3 and StR5. Of these trainees, seven had not performed a vitrectomy under supervision during their VR rotation. Six had performed 1–10 vitrectomies under supervision, and the remaining five had performed a mean of 21.8 supervised cases (range 18–26). There was moderate, statistically significant positive correlation (r (22)=0.60, P=0.003, Spearman’s rho correlation coefficient) between the number of elective vitrectomies performed during supervised VR rotations, and confidence in dealing with PCR and vitreous loss.
Trainees with >350 completed cases
In theory, trainees who have satisfied the RCOphth requirement of completing >350 cases should be sufficiently experienced to practise cataract surgery independently, managing their own complications. Ten pre-CCT trainees had already completed >350 cases (mean 576 cases, range 383–1087). The single post-CCT final year trainee had completed 400 cases. The most junior respondent to achieve >350 cases was a StR4 (n=383). The remainder were StR5 (n=2), StR6 (n=6), and StR7 (n=1). Among these trainees with >350 completed cases, the mean PCR rate was 2.1% (range 1.0–4.9%). The mean number of cases involving PCR managed by the trainee without supervisor take over was 3.5 (range 1–7).
Of the 11 respondents with >350 cases, only two stated they could complete a case involving PCR and vitreous loss without senior support. The remainder could manage but would need senior advice (either scrubbed or unscrubbed). Two trainees reported being very confident in deciding which fluidic parameters to use, and when, where and how to implant an IOL in the event of PCR and vitreous loss. The remainder felt quite confident, except for two who reported being not that confident and would need senior support. Avoiding a dropped nucleus in the presence of PCR and vitreous loss caused more consternation, with 45.5% (5/11) stating they were not that confident and would require considerable senior support. Two respondents were very confident and the remaining four were quite confident.
Respondent #4 was the only trainee who reported being ‘very confident’ with fluidics, IOL placement and avoiding a dropped nucleus, and felt they could complete a case complicated by PCR and vitreous loss without senior support. This trainee was in the final year of training (StR7) and had completed 1087 cases, during which time they had personally managed six cases of PCR. They had undertaken a VR rotation in StR3 and StR5, performing 10 vitrectomies, and had also attended an advanced phacoemulsification course.
Respondent #14 stated they could complete a case complicated by PCR and vitreous loss without senior support. However, they reported being not that confident and needing considerable senior support in avoiding a dropped nucleus, and only quite confident with fluidics and IOL considerations. This trainee was StR6 and had completed 701 cases with a cumulative PCR rate of 2.3%, personally managing 6 cases. They had attended an advanced phacoemulsification course but had never performed a vitrectomy during a VR rotation.
Respondent #2 was the most junior trainee (StR4) to have completed >350 cases (n=383). This trainee’s cumulative PC rupture rate was 1.0% (n=4), and only one of these had been managed by the trainee without supervisor take over. This trainee reported being not that confident with fluidics, IOL placement and avoiding a dropped nucleus. They felt they could manage a case complicated by PCR and vitreous loss, but would need senior advice.
Respondent #10, the only post-CCT trainee, had completed 400 cases with a PCR rate of 3%, personally managing three cases. This respondent had performed 25 supervised vitrectomies during two VR rotations. In the event of PCR, they reported being not that confident with fluidics, IOL considerations and avoiding a dropped nucleus.
Discussion
Repeated, deliberate practice and regular reinforcement are required to develop surgical expertise.6 Reduced working hours have limited the amount of time available for deliberate practice for surgical trainees.6 As evidenced by this survey, opportunities to deal with complications as a trainee may be few and far between. Furthermore, in the real-life setting, PCR represents a serious complication and is often accompanied by negative emotions including stress and disappointment, which may impair performance and restrict learning.7
There is a potential argument that all cases of PCR and vitreous loss should be immediately referred to a VR specialist for further management. Grandinetti et al8 emphasised ‘the importance of an integrated and readily available team of retina specialists to manage such complications.’ Although some may feel that immediate VR take over represents the gold standard, VR support is not available in all hospitals. Certainly, early VR involvement is recommended in the case of dropped nuclear fragments, but it is crucial that surgeons undertaking cataract surgery are confident and competent with the basic ‘first aid’ measures for dealing with PCR. Failure to manage these early steps adequately can lead to problems with intraocular pressure, macular oedema and corneal clarity, which may hinder subsequent VR intervention and final visual outcome.
This small survey suggests that simply completing 350 cases is inadequate for full independent practice as a Consultant Ophthalmologist performing cataract surgery. While UK ophthalmic specialist trainees complete a large number of cases, complication rates are low. There is currently no stipulation regarding the case mix required for CCT. Whereas one trainee may have the opportunity to perform many complex cases, another may just perform 350 routine cases.
Two trainees (respondents #4 and #14) felt they could complete a case complicated by PCR and vitreous loss without support. These two trainees had completed 1087 and 701 cases, respectively, representing the highest numbers within this cohort. This suggests that simply raising the numerical target may address the issue of trainees lacking confidence at the culmination of training. However, in the authors’ opinion, a numerical target—regardless of its magnitude—is insufficient to guarantee competence in managing complications. At most, it may be considered a simple interim measure, pending more substantial revisions to the surgical training curriculum. Rather than trainees aiming for a simple numerical threshold, we advocate a more targeted approach to training, where complicated scenarios are discussed and practised. Initially this could be in a simulated environment, but would ultimately need to be transferred to the real environment of the operating theatre while the trainee is still under supervision.
Our view is that a competency-based assessment framework, including the management of common complications such as PCR, would be preferable to a simple numerical target. Opportunities to tackle complicated cases in real-life are scarce and unpredictable. Therefore, a trainee would be unlikely to complete a competency-based assessment framework by just attending regular supervised theatre lists. In this study, the trainee with the highest number of cases (n=1087) had only personally managed PCR on six occasions, and three trainees with >350 completed cases had only managed PCR once each. The final year respondent who had just received their CCT had only managed PCR three times. This suggests improvements are needed in surgical training away from the real-life learning environment of the operating theatre, employing surgical simulation and other innovative strategies to increase experience in managing complications.
In this study, trainees who had attended advanced phacoemulsification courses reported higher confidence levels in managing PCR. However, this result was confounded by the fact that these were all more senior trainees (StR5 and above) with higher numbers of completed cases. While the authors do not dispute the value of such courses, there is little published evidence to support their utility in improving future surgical performance.
Several respondents commented that practical training in anterior vitrectomy, in a controlled or simulated environment, would be useful. One StR6 respondent stated that their ‘experience of routine vitrectomy (during a VR rotation) has greatly improved my ability to deal with complications in cataract surgery.’ Another StR6 respondent stated: ‘If I had practical anterior vitrectomy training prior to embarking on my first few anterior vitrectomies for PCR, I would have been less stressed and more confident with the overall management of the situation.’
Although all UK ophthalmology trainees undertake at least one rotation in VR surgery, opportunities for hands-on vitrectomy experience are variable. Our survey demonstrated statistically significant, positive correlation between experience in performing elective vitrectomy and perceived confidence in managing PCR. In our unit, we have now introduced a structured programme of supervised vitrectomy training for all trainees approaching independence in cataract surgery, but who have not benefited from operative experience during a VR rotation. Briefly, this involves background reading, followed by a theoretical ‘walk-through’ of what the trainee would do in the event of PCR—led by the supervising Consultant. The trainee is then supervised performing cataract surgery on a patient who is booked for an elective phaco-vitrectomy, before proceeding to perform a three port pars plana core vitrectomy, with a light pipe and infusion but no binocular indirect ophthalmomicroscope. The supervising VR surgeon completes the remainder of the procedure as indicated.
Although this method fails to fully replicate an unplanned anterior vitrectomy with prolapsing vitreous, lens fragments and chamber instability, it enables trainees to become familiar with the feel of performing bimanual vitrectomy in a controlled, non-complicated setting. This is identical to the opportunities afforded to ophthalmic StRs during a formal VR rotation, thus representing an ethical and readily accessible training opportunity for trainees already competent in routine cataract surgery. While we do not currently have strong evidence that this method improves future performance, it is important that surgical trainers consider innovative ways of enhancing trainee development.
When this study was presented locally, a novel suggestion from the audience was that a strategy analogous to Basic Life Support (BLS) resuscitation training could be implemented to support training in management of PCR and other surgical complications (Mrs K. Bush FRCOphth, Wessex Medical Education Fellow, personal communication). This would involve real-time role play whereby trainees work through standardised scenarios in a simulated environment. Although it would require considerable planning and infrastructure, the authors agree that a regular (ie, annual) exercise such as this would be valuable in developing and maintaining confidence and competence in managing scenarios that are infrequently encountered in everyday practice.
Surgical simulation is a rapidly evolving field in both ophthalmology and other surgical specialties. High-fidelity virtual reality simulators such as the EyeSi (VR Magic, Mannheim, Germany) have an expanding evidence base supporting their utility in both cataract and vitreoretinal surgery,9, 10, 11, 12 and newer simulation devices including the Simulated Ocular Surgery models (Phillips Studio Products, www.simulatedocularsurgery.com/about) also hold great promise. Although the EyeSi offers excellent simulation of routine surgical steps, it does not (at the time of writing) offer modules providing realistic simulation of complications such as vitreous loss. The development of such modules would greatly improve training in this area, enabling repeated practice in a safe setting. It is vital that these devices are utilised adequately, and ideally incorporated into the mandatory ophthalmology training curriculum, rather than being used by a few enthusiastic trainees on an ad hoc basis with limited supervision.
This survey was conducted within a single UK postgraduate training Deanery and is thus limited in its scope and wider applicability. By its nature, the survey is vulnerable to recall bias and relies on trainee self-evaluation, which limit its reliability. It would be useful to conduct a similar survey across the UK, in order to explore inter-regional differences and analyse what factors lead to trainees feeling fully prepared to practise cataract surgery independently, managing sight-threatening complications confidently and competently to achieve successful outcomes for patients. Replication of our results elsewhere would support the need for a competency-based framework of assessment in cataract surgery, instead of the current numerical goal of 350 cases.

References
Day AC, Donachie PH, Sparrow JM, Johnston RL . Royal College of Ophthalmologists’ National Ophthalmology Database. The Royal College of Ophthalmologists’ National Ophthalmology Database study of cataract surgery: report 1, visual outcomes and complications. Eye 2015; 29 (4): 552–560.
Ti SE, Yang YN, Lang SS, Chee SP . A 5-year audit of cataract surgery outcomes after posterior capsule rupture and risk factors affecting visual acuity. Am J Ophthalmol 2014; 157 (1): 180–185.e1.
Sparrow JM, Taylor H, Qureshi K, Smith R, Birnie K, Johnston RL et al. The cataract national dataset electronic multi-centre audit of 55,567 operations: risk indicators for monocular visual acuity outcomes. Eye 2012; 26 (6):821–826.
Royal College of Ophthalmologists Ophthalmic Specialist Training Cumulative Data Sheet 2012 Training Committee: Royal College of Ophthalmologists. Available online at https://www.rcophth.ac.uk/training/award-of-the-cct/. accessed 14 May 2015.
Johnston RL, Taylor H, Smith R, Sparrow JM . The Cataract National Dataset electronic multi-centre audit of 55,567 operations: variation in posterior capsule rates between surgeons. Eye 2010; 24 (5): 888–893.
Sadideen H, Kneebone R . Practical skills teaching in contemporary surgical education: how can educational theory be applied to promote effective learning? Am J Surg 2012; 204 (3): 396–401.
Arora S, Sevdalis N, Nestel D, Woloshynowych M, Darzi A, Kneebone R . The impact of stress on surgical performance: a systematic review of the literature. Surgery 2010; 147 (3): 318–330.
Grandinetti A, Suenaga D, Oliveira FM, Cruz KS, Meneguette L, Moreira LB . Results of pars plana vitrectomy after complicated phacoemulsification surgery. Arq Bras Oftalmol 2015; 78 (2): 73–75.
McCannel CA, Reed DC, Goldman DR . Ophthalmic surgery simulator training improves resident performance of capsulorhexis in the operating room. Ophthalmology 2013; 120 (12): 2456–2461.
Pokroy R, Du E, Alzaga A, Khodadadeh S, Steen D, Bachynski B et al. Impact of simulator training on resident cataract surgery. Graefes Arch Clin Exp Ophthalmol 2013; 251 (3):777–781.
Solversen DJ, Mazzoli RA, Raymond WR, Nelson ML, Hansen EA, Torres MF et al. Virtual reality simulation in acquiring and differentiating basic ophthalmic microsurgical skills. Simul Healthc 2009; 4 (2): 98–103.
Pfister MS, Deuchler S, Singh P, Koss M, Krueger H, Koch F . Complete pars plana vitrectomy interventions in the Eyesi Simulator: potentials of virtual reality training in vitreoretinal surgery. Invest Ophthalmol Vis Sci 2011; 52: 543.
Acknowledgements
We thank Dr Nina Attridge PhD for her advice with the statistical analysis, and Mrs Kate Bush FRCOphth for her contribution to the discussion.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
This work is due to be presented at the 2016 Royal College of Ophthalmologists Annual Congress
Rights and permissions
About this article

Cite this article
Turnbull, A., Lash, S. Confidence of ophthalmology specialist trainees in the management of posterior capsule rupture and vitreous loss. Eye 30, 943–948 (2016). https://doi.org/10.1038/eye.2016.55
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2016.55
This article is cited by
-
A model for anterior vitrectomy in real patients: Simulation for practical training
Eye (2024)
-
Non-technical skills simulation-based training model for managing intraoperative posterior capsule rupture during cataract surgery
Eye (2023)
-
Experience gained during vitreoretinal fellowships in the United Kingdom
Eye (2023)
-
Returning to cataract surgery after a hiatus: a UK survey report
Eye (2022)
-
Comparisons between cataract surgery and aviation
Eye (2022)
