
Abstract
Purpose
To describe the visual outcomes and morbidity of newly referred uveitis patients.
Methods
Retrospective cohort study of 133 newly referred uveitis patients with active uveitis who required care in a tertiary center for at least 1 year. Main outcomes were best-corrected visual acuity (BCVA) at referral and 1 year after referral, duration of visual impairment, systemic medications used, as well as all complications and surgeries during the first year of follow-up. Generalized estimating equation models was used to assess prognosticators for poor BCVA.
Results
The mean age at onset of uveitis was 43 years. The proportion of patients with at least one eye with BCVA ≤0.3 decreased from 35% at referral to 26% (P=0.45) at 1-year follow-up. The mean duration of visual impairment in the first year after referral was 4 months per affected eye. At 1-year follow-up, bilateral visual impairment was observed in 4% but at least one ocular complication developed in 66% and 30% of patients required at least one intraocular surgery. Systemic immunosuppressive treatment was required in 35% of patients and the mean number of visits to ophthalmologist was 11 per year, while 8% of patients required hospital admission. Prognosticators for poor visual outcome included surgery undergone before referral (odds ratio (OR), 3; 95% CI, 1–11; P=0.047), visual impairment at referral (OR, 21; 95% CI, 8–54; P<0.001), and glaucoma before referral (OR, 7; 95% CI, 2–28; P=0.007).
Conclusions
Patients with severe uveitis had a favorable BCVA 1 year after referral with only 4% of patients having bilateral visual impairment. This, in contrast to the prolonged duration of visual impairment during the first year of follow-up and the demanding care.
Similar content being viewed by others
Introduction
The visual burden of patients suffering from uveitis is essentially unknown. There is a lack of systematic data assessing visual outcomes in large series of patients with uveitis and the data published so far are based on cohort studies commonly without standardized follow-up.1, 2
The optimal best-corrected visual acuities (BCVA) in the statistics addressing the visual impairment are commonly indicated in incidence and prevalence numbers, and most reports are based on the prevalence of low vision or blindness at one time point, such as the presenting vision used by the World Health Organization or BCVA in the first year or after treatment used in clinical settings.1, 2, 3 The course of disease in uveitis patients is extremely variable and visual performance changes according to the development of exacerbations and/or chronic disease. Although the optimal BCVA may remain useful and can reach a good level after the inflammation subsides, the degree and impact of low vision during the active (sometimes prolonged disease episodes) remains essentially unknown. These periods of disease activity associated with (temporary) decreased vision together with multiple treatments and surgical interventions represent a real disease burden.
The aim of this study is to describe the visual prognosis and the associated risk factors of a poor visual prognosis in patients with active uveitis newly referred to a tertiary Ophthalmology Department and treated there for at least 1 year with respect to the degree, duration, and causes of visual impairment during the first year after referral.
Materials and methods
Study population
We conducted a retrospective cohort study at the Department of Ophthalmology of the Erasmus Medical Center (Rotterdam, The Netherlands), which is a tertiary referral center. The local Medical Ethics Committee reviewed this study and concluded that approval was not required. All data were extracted out of medical records of patients and the research has followed the Tenets of the Declaration of Helsinki Principles. The Strengthening the Reporting of Observational studies in Epidemiology guidelines were used to ensure the reporting of this observational study.4
From January 2010 to January 2013, all newly referred uveitis patients were identified by a coding system of the referred patients. Out of this population, we identified eligible participants according to the following inclusion criteria: (1) presence of active uveitis referred for diagnostic investigations and/or treatment; (2) follow-up in our center for at least 12 months after referral. We excluded patients with inactive uveitis or patients referred for other eye conditions than primarily uveitis, non-medical referral reasons. Patients with visual loss due to other causes than uveitis (eg, amblyopia) were excluded in the final evaluation.
Assessment of determinants and outcomes
At the first visit, all patients underwent a comprehensive ocular examination including the notation of the activity of uveitis, BCVA, pupillary reactions, slit lamp examination, intraocular pressure (IOP) measurement, and fundoscopy, as well as notation of type and modality of treatment. Poor visual prognosis was defined as having visual impairment (moderate and severe) at 1-year follow-up. At follow-up visits, at least the current treatment and results of a routine ophthalmological examination were noted. Uveitis was considered active if anterior chamber cells ≥1+ or vitreous haze ≥1+.5 In posterior uveitis, active chorioretinal lesions were defined as lesions with indistinct borders associated with vitreous cellular reaction of leakage on fluorescein angiography or presence of active vasculitis on fundoscopy or angiography.
All patients underwent a standardized diagnostic investigation protocol according to the localization of the inflammation. This protocol included erythrocyte sedimentation rate, blood counts, serum angiotensin-converting enzyme levels, serology for syphilis, and Lyme disease, as well as interferon-γ release assay (IGRA) test (QuantiFERON–TB Gold In-Tube test) and in those with anterior and panuveitis Human Leukocyte Antigen B27 testing. Radiologic chest imaging was also performed. According to the clinical manifestations, additional examinations were performed (tailored approach). The accepted international criteria were used to diagnose Behçet’s disease and ocular sarcoidosis.6, 7 In short, the diagnosis of definitive ocular sarcoidosis was given to patients that had histologically confirmed diagnosis and presumed sarcoidosis was diagnosed in patients with chest imaging suggestive for the diagnosis of sarcoidosis and no other explanation for the uveitis, but without available histological proof. The diagnosis of ocular toxoplasmosis was always confirmed by intraocular fluid assessment.8, 9, 10, 11 Diagnosis of presumed ocular toxoplasmosis was based on typical clinical features of unilateral focal necrotizing retinitis sometimes associated with typical old pigmented scars. All other specific diagnoses were performed according to current diagnostic criteria. Definitive anatomical classification was performed (eg, localization and laterality of uveitis) according to the Standardization of Uveitis Nomenclature Working Group,5 by reviewing the whole follow-up period.
Diagnoses were grouped into infectious and non-infectious diseases and in established clinical ocular syndromes (eg, pars planitis, birdshot chorioretinopathy). Patients with established ocular syndromes and identified cause or association with systemic disorder (eg, multiple sclerosis with intermediate uveitis or documented rubella virus infection in Fuchs heterochromic uveitis syndrome) were classified according to the cause of their uveitis and not according to their ocular syndrome. Patients with a positive IGRA test in the presence of otherwise unexplained uveitis were classified as of unknown origin and further specified as latent tuberculosis-associated uveitis.
The following patient characteristics were extracted at the time of referral: gender, race, age at onset of uveitis, age at referral to our center, duration of interval from onset of uveitis to referral to our tertiary center, as well as already established causes of uveitis and/or associated systemic diseases, BCVA at referral and results of full ocular examination, ocular co-morbidities, and all complications of uveitis present upon referral. The main cause of visual loss during the follow-up was attributed to the first complication, which caused the visual impairment. Also, type, frequencies and duration of treatment modalities, complications, and surgical interventions were registered.
During the first year of follow-up, we assessed the degree and duration of visual impairment and how often the patients visited our department (only uveitis-related visits were counted). Visual impairment was classified into the following categories: (1) no visual impairment (BCVA >0.3); (2) moderate visual impairment (BCVA 0.16–0.33); and (3) severe visual impairment (BCVA ≤0.1).12 The duration of each category of BCVA was measured as follows: the BCVA at visit 1 was taken and assumed constant until the next visit and the time between the two visits was the duration of the measured BCVA.
The following outcomes were measured at 1-year follow-up: BCVA, activity of uveitis and all other ophthalmological findings, and the newly established causes of uveitis and/or associated systemic disorders. If a patient had a planned ocular surgery within the first year after referral, but the surgery was actually performed at the end of the first year, the BCVA after that ocular surgery was taken. In our retrospective data, no reliable distinction could be made between ocular hypertension and glaucoma. Glaucoma was defined as an IOP of >24 mm Hg measured at least at two subsequent visits, which was combined with glaucomatous opticopathy.5 Epiretinal membrane (ERM) and cystoid macular edema (CME) were diagnosed when proven on optical coherence tomography (OCT).
Statistical analysis
Continuous data are presented as mean±SD, whereas categorical data are presented as proportions. The effect of the exposure variables on low BCVA was analyzed using multivariate logistic regression analyses in which all exposure variables were included and stepwise regression was utilized. Generalized estimating equation was applied to account for the correlation between both eyes of the same patient. Next, odds ratios (ORs) with corresponding 95% confidence interval (CI) were calculated. All statistical analyses were performed using SPSS software (version 22.0, Chicago, IL, USA). A P-value of <0.05 was considered statistically significant.
Patients with missing data on BCVA were excluded from the analysis. For all calculations with BCVA data, we converted decimal Snellen BCVA to the logarithm of the minimum angle of resolution (logMAR). For easier understanding, the logMAR results were converted back to decimal Snellen VA and only Snellen VA were reported.
Results
A total of 401 patients with uveitis were referred to our center in the specified time window. Among those, 133 patients (219 affected eyes) met the inclusion criteria and formed the final study population and 268 patients were excluded (Table 1). For the analysis of duration of visual impairment, we excluded one eye of a patient who underwent an enucleation (not related to uveitis).
Patient characteristics
The demographics and specific diagnoses are given in Table 1. The duration of interval from onset to referral was 2.5 years (±0.2 years).
In 65% of the cases, the inflammation of uveitis was bilateral. The percentage of those with anterior uveitis was 26%. Our study included one patient positive for HIV.
Patient characteristics and changes during follow-up
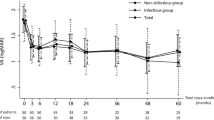
The ocular patient characteristics at referral and 1 year after referral are depicted in Tables 2 and 3. The proportion of patients with visual impairment in at least one eye decreased from 47/133 (35%) to 34/133 (26%; P=0.45; Table 2). In this visually impaired group, severe visual impairment decreased from 24/133 (18%) to 21/133 (16%) at 1 year of follow-up.
At 1-year follow-up, 4% had bilateral visual impairment, and 22% had unilateral impairment (out of which 14% severe; 18 patients). Active uveitis at 1-year follow-up was still present in 32%. Systemic treatment at referral was given to 16% of patients, which increased to 35% (P<0.001) after 1 year. Non-steroidal immunomodulatory drugs were most commonly used (25%) at 1-year follow-up (in patients who needed systemic treatment), while at referral systemic corticosteroids were mostly prescribed (8%).
The development of new complications during 1-year of follow-up was noted in 66% of patients (Table 3); the most frequent new complication was cataract and CME. All, except for two patients, with new-onset CME had non-anterior uveitis. The characteristics of ocular surgery performed during follow-up are illustrated in Table 3. Ocular surgery during the first year of follow-up was indicated in 18% of the affected eyes.
Combined, 59% of the ocular surgeries involved a cataract extraction, which shows that cataract extraction was the most required surgery in affected eyes. The mean duration of visual impairment during the first year after referral was 4 months (range 0.25–12 months) per uveitis eye. Severe visual impairment was present in 41 of 219 (19%) affected eyes and the mean duration of visual loss was 6 months (±2.7 months) per uveitis eye during the first year after referral. A total of 70 uveitis eyes had moderate visual impairment (70/219; 32%) during the first year after referral and the mean duration of visual loss in this group was 4 months (±3.1 months). During follow-up, the mean number of visits to ophthalmologist per patient was 11 (range 2–23) per year and 8% of patients required hospital admission for systemic treatment of their uveitis.
Causes of visual impairment
Table 4 shows the most common causes of visual impairment. The main causes of visual impairment were CME, retinal scars and glaucoma, for both severe and moderate visual impairment.
Risk factors for poor visual outcome
In the multivariate analysis, the poor visual outcome at 1-year follow-up was associated with visual impairment at referral (OR, 21; 95% CI, 8–54; P<0.001) and glaucoma before referral (OR, 7; 95% CI, 2–28; P=0.007), and we found a borderline association with surgery undergone before referral (OR, 3; 95% CI, 1–11; P=0.047), while non-anterior uveitis, age, race, gender, having systemic disease, use of systemic treatment, and CME were not associated with the visual outcomes at 1 year.
Discussion
We report on satisfactory 1-year follow-up visual outcomes in patients with active and chronic uveitis who were newly referred to a tertiary center and who required tertiary care during the first year after follow-up. Despite the favorable visual outcomes, the prevalence of complications and the intensity of ophthalmological care were enormously high. While severe bilateral visual impairment occurred in only 2% of patients, the majority of patients suffered from visual impairment during their first year after referral (51%), severe and multiple ocular complications needed frequent visits to an ophthalmologist and commonly required intraocular surgery. The above findings emphasize that the care for patients with chronic uveitis in tertiary centers is demanding and requires huge ophthalmological investments in the form of time and resource utilization.
Previous studies on visual prognosis of uveitis differ in terms of included population and time at which the VA is measured. These studies are mostly cross-sectional and include all patients ever seen in the tertiary centers (Table 5) and consequently indicate VA in various stages of uveitis and have no standardized point of measurement. In addition, usually a total population with uveitis from a tertiary center was studied, including the cases with long-term follow-up (and frequently compromised VA) creating a bias for more severe patients (since tertiary centers will keep the patients with poor VA, while patients with satisfactory outcomes will be referred back to their ophthalmologists). The percentage of the patients with anterior uveitis is being commonly used as an indicator of the severity of included uveitis population: while studies from peripheral ophthalmologic centers are characterized by a majority (~80%) of patients with anterior uveitis, the reports from tertiary centers include mostly lower percentages (Table 5), which is in accordance with our findings.1, 2, 13
Our study included patients with active uveitis who required treatment in a tertiary center and a high proportion of subjects was excluded (67%) because the follow-up was <1 year. It is highly probable that the visual outcomes for the whole uveitis population will even be better than in our population of severe and chronic cases (Table 2).
In the previous studies, the proportion of patients with visual impairment (VA ≤0.3) in at least one eye varied from 25 to 35%,1, 2, 13, 14 which is in concordance with 26% in the present series. Our findings on satisfactory visual outcomes are in agreement with the recent study of Tomkins-Netzer et al.1 In the study of Durrani et al,2 a much higher proportion of visual impaired patients (VA ≤0.3) was found (reaching 70%), which is explained by the fact that the authors included the whole uveitis population and included all moments of visual loss during the follow-up period reaching from 1 month to 30 years. Bodaghi et al13 included only patients with severe chronic uveitis who had a poor BCVA at presentation, giving also rise to selection bias. Our findings on visual outcomes are better than the results of the study performed in The Netherlands almost 20 years ago with the similar inclusion criteria (the number of patients with bilateral VA ≤0.3 in the present series being 5/133 patients vs 57/582 patients in previous series, P=0.026).14 In addition, the former study had a higher percentage of patients (42%) with anterior uveitis than 26% in our present series. The improvement in visual outcomes over time might be explained by the change and development of treatment approaches.
The duration of visual impairment due to uveitis was to our knowledge examined only in the study of Durrani et al.2 The authors reported the duration of ~66% of the follow-up time, which is roughly consistent with our results (4 months/eye/year). The difference can be most likely explained by the different inclusion criteria and follow-up duration (in the present study being 1 year after referral to a tertiary center). The VA measured at one time point is not an accurate measure and our study indicates that the duration of visual impairment could be a more accurate measure in terms of the burden of these patients. Similar to the findings of previous studies, the mean age at presentation in our series was 43 years.1, 2, 13, 14 Together with the duration of visual impairment of 4 months/eye/year in our series; this group is likely associated with a significant socioeconomic burden. Little is known about the exact costs of uveitis patients. A previous study estimated the average monthly costs of treated patients with non-infectious uveitis in 2009 ranging from US$ 1144 to US$ 2689, depending on the treatment regimens, which indicates that monthly healthcare costs are similar to those with diabetes mellitus and cancer patients.15, 16, 17 Moreover, the costs associated with uveitis care measured only costs of medications and did not include the costs associated with hospital visits and intraocular surgeries.
The most common new complications in the present series were cataract, CME, and ERM, which is slightly different from the previous studies in which glaucoma took the third place.13, 14 This may be related to the early detection of mild ERM by the introduction of the OCT scanning technique or by different registration of complications. Glaucoma occurred in 6% of all new complications within the first year, which is similar to previous findings.13
Our study points out CME, retinal scars, and glaucoma as major causes of visual impairment in uveitis, which is consistent with previously published reports.1, 2, 13, 14 One of the previous studies reported corneal opacities (mostly band keratopathy) as a cause of visual impairment, something we did not encounter in our present population.14 The better treatment over time and our inclusion criteria might explain this discrepancy. The previous studies indicate that poor visual outcomes were associated with having non-anterior uveitis. In the present series, the visual prognosis at the first year after referral did not differ for patients with anterior and non-anterior uveitis. This might be explained by the fact that the present study included solely patients with severe anterior uveitis requiring a follow-up of more than 1 year in a tertiary center. Although CME was the most common cause of visual impairment, having new-onset CME was not associated with poor visual outcome. CME was a common complication in our series (38% at referral and/or during 1 year follow-up) and included also cases in which VA was not compromised. It is probable that the early detection of CME by the routine use of the OCT scanning technique and more vigorous therapy in the early stages explain the higher prevalence of mild new-onset CME and a lower impact on VA in our series.
The favorable visual outcome probably reflects the intensive treatment of our patients. While in the past corticosteroids were the most common drugs used, our patients received predominantly non-steroidal immunomodulatory drugs. Still, 48% of the patients did not receive any systemic immunosuppressive treatment during the first year after referral. These patients received various local treatment modalities (including periocular and intraocular injections of predominantly of corticosteroids) and/or antibiotic treatment used for various infectious disorders and/or acetazolamide for macular edema. However, the design of our study does not allow any comparisons on treatment modalities over time and the causes of better visual outcomes are not yet identified. The percentage of patients with intraocular surgeries in our series is similar to that of previous studies.1, 2, 13, 14 The most frequent procedure was cataract extraction, which is also consistent with the previous reports.1, 2, 13, 14
VA is not the only indication for the outcome in all uveitis entities, particularly in conditions such as birdshot chorioretinopathy in which the central VA may remain uncompromised during long time. Retrospective study design prevents the systematic evaluation of visual fields in our patients. In addition, given that uveitis is a chronic condition, 1 year is not a long enough time period to follow visual outcomes and longer follow-up studies are needed. Another possible limitation of our study is the heterogeneity of diverse uveitis entities included. However, we did not aim to report on visual prognosis of specific uveitic entities, but report on an overall burden of uveitis treated in tertiary center. We attempted to select a more homogenous population of patients than previous studies and did not include all patients who were followed in a tertiary center.
Our study includes newly referred patients to the tertiary center of patients with a namely Caucasian ancestry. Because of reference bias, our results cannot be used for the general population of uveitis patients outside a tertiary referral center. However, our study population is similar to previous studies, which were predominantly performed in tertiary centers. The biases inherent to retrospective study design such as misclassification, treatment bias, and confounding also apply. Misclassification of the duration of visual impairment could be an issue due to the retrospective design, as patients VAs were more frequently measured when they had visual impairment. Thus, the duration of impairment is related to how precise the fluctuation in VA is measured, resulting in a more precise measurement for more severe uveitis cases.
In conclusion, we present results from a cohort of newly referred patients with active uveitis to a tertiary center and illustrate that a majority of patients develops ocular complications and (temporary) decreased vision during the first year after referral, and show that a substantial part of patients requires systemic treatment and intraocular surgery. However, the visual results at the end of the first year were favorable with only 4% of patients having bilateral visual impairment. Our findings show that the tertiary care for patients with uveitis is complex, time-consuming, and requires vigilant follow-up of patients by ophthalmologists taking care of this population.

References
Tomkins-Netzer O, Talat L, Bar A, Lula A, Taylor SR, Joshi L et al. Long-term clinical outcome and causes of vision loss in patients with uveitis. Ophthalmology 2014; 121 (12): 2387–2392.
Durrani OM, Tehrani N, Marr JE, Moradi P, Stavrou P, Murray PI . Degree, duration, and causes of visual loss in uveitis. Br J Ophthalmol 2004; 88 (9): 1159–1162.
Pascolini D, Mariotti SP . Global estimates of visual impairment: 2010. Br J Ophthalmol 2012; 96 (5): 614–618.
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP . STROBE initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 2008; 61 (4): 344–349.
Jabs DA, Nussenblatt RB, Rosenbaum JT . Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol 2005; 140 (3): 509–516.
Herbort CP, Rao NA, Mochizuki M . International criteria for the diagnosis of ocular sarcoidosis: results of the first International Workshop On Ocular Sarcoidosis (IWOS). Ocul Immunol Inflamm 2009; 17 (3): 160–169.
Okada AA, Stanford M, Tabbara K . Ancillary testing, diagnostic/classification criteria and severity grading in Behçet disease. Ocul Immunol Inflamm 2012; 20 (6): 387–393.
Westeneng AC, Rothova A, de Boer JH, de Groot-Mijnes JD . Infectious uveitis in immunocompromised patients and the diagnostic value of polymerase chain reaction and Goldmann-Witmer coefficient in aqueous analysis. Am J Ophthalmol 2007; 144 (5): 781–785.
De Groot-Mijnes JD, Rothova A, Van Loon AM, Schuller M, Ten Dam-Van Loon NH, De Boer JH et al. Polymerase chain reaction and Goldmann-Witmer coefficient analysis are complimentary for the diagnosis of infectious uveitis. Am J Ophthalmol 2006; 141 (2): 313–318.
Oahalou A, Schellekens PA, de Groot-Mijnes JD, Rothova A . Diagnostic pars plana vitrectomy and aqueous analyses in patients with uveitis of unknown cause. Retina 2014; 34 (1): 108–114.
Errera MH, Goldschmidt P, Batellier L, Degorge S, Héron E, Laroche L et al. Real-time polymerase chain reaction and intraocular antibody production for the diagnosis of viral versus toxoplasmic infectious posterior uveitis. Graefes Arch Clin Exp Ophthalmol 2011; 249 (12): 1837–1846.
Dandona L, Dandona R . Revision of visual impairment definitions in the International Statistical Classification of Diseases. BMC Med 2006; 4: 7.
Bodaghi B, Cassoux N, Wechsler B, Hannouche D, Fardeau C, Papo T et al. Chronic severe uveitis: etiology and visual outcome in 927 patients from a single center. Medicine (Baltimore) 2001; 80 (4): 263–270.
Rothova A, Suttorp-van Schulten MS, Frits Treffers W, Kijlstra A . Causes and frequency of blindness in patients with intraocular inflammatory disease. Br J Ophthalmol 1996; 80 (4): 332–336.
Chu DS, Johnson SJ, Mallya UG, Davis MR, Sorg RA, Duh MS . Healthcare costs and utilization for privately insured patients treated for non-infectious uveitis in the USA. J Ophthalmic Inflamm Infect 2013; 3 (1): 64.
Laliberté F, Bookhart BK, Vekeman F, Corral M, Duh MS, Bailey RA et al. Direct all-cause health care costs associated with chronic kidney disease in patients with diabetes and hypertension: a managed care perspective. J Manag Care Pharm 2009; 15 (4): 312–322.
Chang S, Long SR, Kutikova L, Bowman L, Finley D, Crown WH et al. Estimating the cost of cancer: results on the basis of claims data analyses for cancer patients diagnosed with seven types of cancer during 1999 to 2000. J Clin Oncol 2004; 22 (17): 3524–3530.
Acknowledgements
An abstract of this article has been presented on the National Congress of the Dutch Opthalmological Society on 26 March 2015.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Groen, F., Ramdas, W., de Hoog, J. et al. Visual outcomes and ocular morbidity of patients with uveitis referred to a tertiary center during first year of follow-up. Eye 30, 473–480 (2016). https://doi.org/10.1038/eye.2015.269
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2015.269
This article is cited by
-
Complete blood count parameters and neutrophil-to-lymphocyte ratio values as markers for differentiation between systemic infectious and non-infectious uveitis
International Ophthalmology (2020)
-
Efficacy of glaucoma drainage devices in uveitic glaucoma and a meta-analysis of the literature
Graefe's Archive for Clinical and Experimental Ophthalmology (2019)
-
Relevance of erythrocyte sedimentation rate and C-reactive protein in patients with active uveitis
Graefe's Archive for Clinical and Experimental Ophthalmology (2019)
