
Abstract
Purpose
Malignant melanoma of the eye is an uncommon condition that is important to recognise. We describe three cases in which ocular foreign bodies have masqueraded as ocular malignant melanoma.
Methods
Interventional case reports.
Results
Case 1 describes diathermy-induced carbon particle implantation, during plaque therapy for the treatment of uveal melanoma, mimicking recurrence with extra-scleral invasion. Case 2 shows a foreign body called ‘mullite’ mimicking conjunctival melanoma. Case 3 demonstrates a conjunctival foreign body called ‘illite’ that mimicked a limbal melanocytic lesion, clinically thought to be either melanocytoma or melanoma.
Conclusion
This report highlights the importance of careful history taking, examination, and appropriate biopsy in cases of suspected malignant melanoma, to prevent unnecessary and potentially radical treatment.
Similar content being viewed by others


Introduction
Ocular malignant melanoma is an uncommon malignancy, which affects uveal tissue (predominantly choroid) and conjunctiva of the eye. Once diagnosed, treatment is instigated immediately to achieve local control and reduce risk of metastasis, which carries poor prognosis. Particularly in choroidal cases, where acquiring biopsy tissue can be difficult, diagnosis is often purely clinical before treatment. This report describes three novel cases from an ocular oncology centre in which ocular foreign bodies have mimicked malignant melanoma.
Case series
Case 1
A 48-year-old man, who underwent ruthenium plaque brachytherapy 15 years earlier for choroidal malignant melanoma, re-attended clinic with suspicious inferotemporal subconjunctival pigmentation (Figure 1a). Episcleral biopsy showed black, non-refractile, carbon-like particles lined up along collagen fibres, and around blood vessels, as well as in a dendritic or spider configuration mimicking dendritic melanocytes (Figure 1b). Mostly these were definite exogenous carbon particles, but immunohistochemistry was performed on bleached specimens to exclude the presence of a melanocytic lesion or malignancy. This failed to demonstrate melanocytes. It was felt that the most likely explanation was carbon deposition caused by diathermy during plaque surgery.


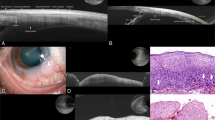
(a, case 1) Clinical photograph of right eye showing inferotemporal subconjunctival pigmentation (white arrow) and, above this, conjunctival granuloma in association with Dacron suture. (b, case 1) Haematoxylin and eosin (H&E)-stained section demonstrating the particulate black carbon-like material, arranged in linear and dendritic configurations, between collagen fibres. (c, case 2) Clinical photograph of left eye showing inferior bulbar conjunctival brown pigmentation. (d, case 2) H&E-stained section with arrow pointing to a foreign body-type giant cell adjacent to brown-black foreign body material. (e, case 2) H&E showing a higher-power view of the foreign material. (f) Transmission electron micrograph showing the black electron-dense material, some of which is spiculate/needle-like. (g) The EDAX spectra from areas of pigmentation showing strong peaks of Al, Si, and O, which are considerably greater than those found from nearby pigment-free areas of the sample (not shown). The composition mix is consistent with ‘mullite’ mineral. (h) Case 3 clinical photo. (i) Case 3, higher-power clinical photo. (j) B-scan showing the mass at the limbus. (k) H&E-stained section showing black particulate material in the stroma, with overlying hyperplastic conjunctival epithelium. (l) Higher-power view of black material. (m) Transmission electron micrograph showing rhomboid-like crystalline material. (n) EDAX readout showing peaks in Al, Si, Mg, and K, with the compositional mix consistent with ‘illite’ mineral.
Case 2
A 31-year-old woman, with a history of previous severe road traffic accident requiring eyelid reconstruction, was referred to the ocular oncology service with areas of increasing pigmentation affecting predominantly the inferior bulbar conjunctiva of the left eye (Figure 1c). Biopsies showed normal conjunctival epithelium and evidence of brown to black, refractile foreign body material in the substantia propria with associated giant cell reaction (Figures 1d and e). Transmission electron microscopy demonstrated electron-dense crystalline material, with spicules up to 140 nm in length and 14 nm in diameter (Figure 1f). Occasional macrophages and fibroblasts contained similar material. Energy-dispersive analysis of X-rays (EDAX) revealed the chemical composition to be an aluminium silicate material, most likely a synthetically produced polycrystalline form of ‘mullite’ (Figure 1g), which presumably became embedded at the time of her accident.
Case 3
A 51-year-old Nigerian woman was referred with an enlarging, deeply pigmented lesion at the temporal limbus of the left eye, present for 30 years and suspected to be melanocytoma or melanoma (Figures 1h–j). Pathology report following excision revealed a black crystalline foreign material in the substantia propria, with no melanocytes (Figures 1k–m). EDAX identified silicon, aluminium, magnesium, potassium, and a small amount of iron, all compatible with a clay mineral called ‘illite’ (Figure 1n).
Discussion
This report describes three cases of ocular surface foreign body mimicking pigmentation of ocular surface tissues suspicious of malignant melanoma.
In case 1, retained carbon particles after diathermy use raised the suspicion of extra-ocular recurrence of choroidal malignant melanoma. Histopathology demonstrated some particles, arranged similarly to melanocytes, which necessitated immunohistochemistry to exclude malignancy. A previous description of foreign body mimicking extra-scleral extension of choroidal melanoma was caused by scleral explant for retinal detachment with associated haemorrhage.1 In our case, biopsy dictated the management plan, as recurrent choroidal melanoma with extra-scleral extension would be treated with enucleation of the eye. Before biopsy, however, particularly in the context of previous brachytherapy, scleral thinning or traumatic uveal ectasia must be excluded as the cause of apparent pigmentation, as biopsy of this may prove devastating. Fortunately, this is usually possible on clinical examination, but can be definitively excluded using ultrasound biomicroscopy.
Cases 2 and 3 presented with increased conjunctival pigmentation, suspicious for primary acquired melanosis or conjunctival malignant melanoma. Initial histopathology report identified an exogenous substance embedded in the conjunctiva in both cases, and EDAX was used to elucidate the chemical composition.
The foreign body in case 2 was identified as ‘mullite’, a rare silicate material of post-clay genesis, produced by melting and firing processes. It is mixed with magnesia and silica to produce industrial emery, which when crushed can be used to make asphalt and tarmac mixtures,2 which became embedded during a road traffic accident 4 years previously.
The foreign body in case 3 was identified as ‘illite’, a naturally occurring clay mineral found in West Africa, to where the patient belonged. It is used in structural clay products, such as brick and tile. The patient mentions no specific history of how this may have become embedded.
Previous descriptions of foreign bodies masquerading as conjunctival malignant melanoma include mascara deposits,3 graphite from injury with a pencil,4 airgun pellet injury,5 suture reactions,6 and pathology such as conjunctival mycosis.7 Historically also, adrenochrome deposits from adrenalin analogues used for the treatment of glaucoma caused similar pigmentation.8
These cases demonstrate novel ocular foreign bodies that mimicked malignant melanoma. Biopsy of suspicious ocular lesions outside ocular oncology centres is generally discouraged, as it is felt that the best opportunity for complete excision is the first attempt. Hence, if suspicion of malignancy is raised, we would recommend careful history taking and early referral, followed by biopsy in expert hands to ensure the correct treatment pathway is instigated.

References
Scott JA, Damato BE, Smith PA, Gurney PW . Scleral explant mimicking malignant melanoma. Eye 1994; 8: 606–608.
Austin GT . Abrasive materials. Minerals Yearbook 1987; 71–84.
Shields JA, Marr BP, Shields CL, Eagle RC Jr . Conjunctival mascaroma masquerading as melanoma. Cornea 2005; 24 (4): 496–497.
Guy JR, Rao N . Graphite foreign body of conjunctiva simulating melanoma. Cornea 1986; 4: 263–266.
Gelston CD, Mandava N, Durairaj VD . Orbital foreign body masquerading as conjunctival melanoma 60 years after injury. Clin Experiment Ophthalmol 2005; 33 (6): 661–663.
Chung HS, Feder RS, Weston BC, Bryar PJ . Suture reaction masquerading as conjunctival malignancy. Can J Ophthalmol 2006; 41 (2): 207–209.
Laquis SJ, Wilson MK, Haik BG, Fleming JC, Baber W . Conjunctival mycosis masquerading as melanoma. Am J Ophthalmol 2002; 134 (1): 117–118.
Reinecke RD, Kuwabara T . Corneal deposits secondary to topical epinephrine. Arch Ophthalmol 1963; 70: 170–172.
Acknowledgements
We are indebted to Dr Gary Burdett, Principal Scientist, Analytical Sciences, Inorganics and Fibres Section, Health and Safety Laboratory, Buxton, Derbyshire, UK for performing the EDAX analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Maudgil, A., Wagner, B., Rundle, P. et al. Ocular surface foreign bodies: novel findings mimicking ocular malignant melanoma. Eye 28, 1370–1374 (2014). https://doi.org/10.1038/eye.2014.177
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2014.177
