
Abstract
Background/aims
Finding all retinal breaks is a critical step in rhegmatogenous retinal detachment (RRD) surgery in order to prevent persistent/recurrent retinal detachment (RD). We describe a technique of trans-scleral dye injection into the subretinal fluid under the detached retina in the context of recurrent/persistent RD in vitrectomized eyes, in order to determine the location of clinically unidentified (occult) retinal breaks causing RD.
Methods
Retrospective consecutive single-surgeon case-series analysis of patients presenting with a repeat RRD after having been treated with pars plana vitrectomy (PPV) as the method of primary RRD repair. Trans-scleral injection of subretinal vision blue (TSVB) was used to help identify retinal breaks during repeat vitrectomy. Outcome measures: successful detection of a break; location of breaks; persistent retinal attachment; final visual acuity (VA); complications.
Results
There were 395 cases of RRD during the 3-year period reviewed. TSVB was used for eight instances in seven eyes. All eight instances were repeat RRD. TSVB facilitated occult break detection in 7/8 instances of use. Breaks were at or adjacent to the previous cryo site in three instances. Persistent retinal attachment was achieved in 5/7 cases. Final VA increased in 5/7 cases. There was no evidence of complications as a result of TSVB injection.
Conclusions
TSVB coupled with indentation to vent a plume of dye through an occult break during vitreous surgery is a relatively simple technique that may facilitate the identification of occult retinal breaks and help achieve anatomical success and functional success.
Similar content being viewed by others


Introduction
Identification of all retinal breaks is a critical step in rhegmatogenous retinal detachment (RRD) repair. An unsealed break will allow trans-retinal fluid flow into the subretinal space and cause a re-detachment. Despite a thorough pre- and intra-operative search, a break may remain elusive. We describe the result of a single-surgeon series to identify clinically undetected retinal breaks by trans-scleral injection of Vision Blue (0.006% version of Trypan blue, DORC, Zuidland, The Netherlands) during vitreous surgery for persistent/recurrent retinal detachment (RD).
Materials and methods
The vitreo-retinal surgery records of the senior author (RLB) were reviewed for the past 3 years (from beginning of 2007 to end of 2009) at the Norfolk and Norwich University Hospital, UK (university teaching hospital). There were 395 cases of retinal detachment from 1 January 2007 to 31 December 2009. All patients had undergone a standard 3-port pars plana vitrectomy (PPV) as the primary technique to repair RRD.
Seven patients presented with repeat RRD in which the site of the break causing the RD could not be clinically identified. Trans-scleral vision blue (TSVB) was used to aid occult break detection. The case notes of these patients were reviewed retrospectively. Case histories are summarized in Table 1.
In these cases, patients were carefully examined using indentation with 20D lens pre-operatively but a break could not be found. Intra-operatively, during repeat vitreous surgery, a microscope-mounted binocular indirect viewing system fitted with a stereoscopic inverter (BIOM, Germany) was used combined with repeat indentation to identify the break.
Technique
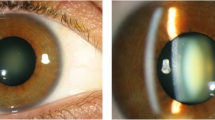
When a break was not found, VB was injected trans-sclerally using a 30-guage needle mounted on an 1-ml syringe. The tip of the needle was applied to the globe tangentially (bevel-away-from-sclera so that when the needle is in the subretinal space, the bevel is away from the retina) and used in a manner similar to an indenter. Pressure was exerted, under observation using the microscope, until internal distortion of the globe was visible. The needle was positioned where the depth of the subretinal fluid (SRF) was greatest (most bullous RD). Pressure was exerted on the globe using the needle until the needle tip penetrated the globe. Once the tip of the needle was just visible intra-ocularly, the dye was injected carefully into the subretinal space (Figure 1). Sufficient volume of dye was injected such that the SRF was stained. The needle was then removed. Dynamic scleral depression (DSD) using an indenter with endo-illumination was performed to encourage the dye to vent out of the undetected break. When successful, a plume of dye was visible in the vitreous infusate (Figure 2). If no plume was seen then the heavy oil (perfluorodecalin) could be used, in conjunction with globe rotation, to encourage expression of dye. Once it was determined that there were no other breaks, the dye was drained through the break site. A drainage retinotomy was required on one occasion where no break was identified (see case 6). Cryotherapy (cryo) was applied to the new-found break and surgery was then completed in a standard manner.

Trans-scleral vision-blue injected into subretinal space, staining the sub-retinal fluid.

Dynamic scleral depression venting a plume of vision blue through a previously undetectable break.
Illustrative cases
Case 4
A 45-year-old high-myope presented with a RRD with a visual acuity (VA) of 6/12. He underwent a standard 3-port PPV with cryo and 18% C2F6 injection. He had uncomplicated cataract extraction and intra-ocular lens implant 4 months later. After 3 months he represented with a shallow macula-on RRD. Despite a thorough pre-operative and intra-operative search using indentation, the break could not be identified. TSVB injection identified a new break infero-temporally. He underwent a repeat PPV+cryo+18% C2F6 injection. He was discharged 2 months later with a flat retina. VA at discharge was 6/6.
Case 5
A 74-year-old man presented with a macula-off RRD and VA of 6/36. Surgery with PPV+cryo+18% C2F6 injection was performed. The retina was flat at the post-operative review. After 2 weeks peripheral SRF was noted and he underwent further PPV+cryo+C2F6 22%, again with a flat retina the following day. After 2 weeks he re-represented with a macula-off RRD. PPV+cryo and C2F6 18% was performed, with a flat retina noted at the 2-week follow-up. Persistent SRF was noted 1-month later, with no obvious break. TSVB was used and identified a break. He had PPV + silicone oil tamponade with a flat retina after surgery. After 4 months oil removal was performed with endolaser and encircling band, with 20% C2F6. On follow-up, a sub-total RD was noted and a causative break could not be clinically identified. Patient declined further surgery. The final VA was 6/60. In this case, either a new break was responsible for the repeat RD or the original break identified with VB was not responsible for the preceding RD.
Results
Case summaries with visual outcomes are presented in Table 1. There were no instances of undetected breaks in primary repair. There were eight instances of sub-retinal vision blue use in seven eyes in that time period. The use of VB was successful in 7/8 instances for the purposes of locating the clinically unidentified retinal break. All cases that required VB were retinal re-detachments. One case was macula on; the remainder were macula off. Four of our patients were pseudophakic. Clinically undetectable breaks were at or adjacent to the previous cryo site in three instances. At final review, five patients had an increase in VA. Persistent retinal attachment was achieved in five out of seven cases; one case had a subtotal persistent detachment. Silicone oil was used in three cases and SB in one. Final VA increased by two Snellen lines in 4/7 cases. There was no evidence of complications as a result of TSVB injection.
Discussion
The identification of all retinal breaks is an important step in the management of RRD. Estimates regarding unidentifed breaks complicating RRDs vary from 6–13%.1, 2, 3
A meticulous pre-operative examination must be performed using binocular indirect ophthalmoscopy with indentation, regardless of whether PPV or SB is planned.
An internal search for retinal breaks using indentation microsurgery was first described by McLeod, using PPV.4 This has been further elaborated to a dye extrusion technique,5, 6 involving injection of sub retinal trypan blue, using a 41-guage needle, into the SRF. Extrusion of the dye is encouraged through the presumed break using perfluorocarbon liquid to fill the eye and systematic rotation of the globe, with the aim of seeing a plume of dye venting out of the break. The use of a dye provides color contrast that aids detection and is an advantage over the use of heavy liquid alone. In some instances, the dye stains the devitalized tissue of the break itself. This was reported in the context of both primary and repeat RD repair.5, 6
Our technique of trans-scleral injection of VB was successful in 7/8 attempts to identify the clinically undetected retinal breaks in the setting of retinal re-detachments. Persistent retinal attachment was achieved in five out of seven cases. Final VA increased by two Snellen lines in 4/7 cases. We experienced no complications related to the dye use. The advantage of this technique over trans-retinal injection is that iatrogenic break creation is avoided. For posterior breaks, the technique can still be employed: the dye is injected and an air exchange carried out encouraging the dye posteriorly.
Theoretically, possible complications of trans-scleral injection include hypotony, choroidal hemorrhage, retinal hemorrhage,7 and retinal and vitreous incarceration. Iatrogenic break creation is a possibility and would render the technique less effective if it occurs. Retinal toxicity remains a potential complication, especially as some may be left in the subretinal space. Efforts to remove the dye by internal drainage, would only debulk rather than completely protect the tissues. However, VB is a lower concentration of Trypan blue, the use of which has been described safely before in the sub-retinal dye extrusion technique.5, 6 It can be argued that the loss in VA of some of the patients was potentially due to dye toxicity. However, Veekeneer et al,8 investigating toxicity of Trypan blue at various concentrations (0.2 and 0.06%) found that only at 0.2% did Trypan blue show any signs of toxicity, manifest as damaged photoreceptors and marked disorganization with light and electron microscopy and reduced immunohistochemical staining for rhodopsin. At 0.06% concentration of Trypan blue (the concentration of Trypan blue available as VB) was concluded to be harmless. However, VB is licensed for use in cataract surgery by the Food and Drug Administration and not for subretinal dye, at this time. Finally, although controversy remains, one could argue that use of a buckle during the initial or subsequent surgeries would have achieved a better anatomical outcome preventing the need for the use of the dye. Overall, this was a small study and additional larger-scale studies on this technique would be useful.
The technique that the surgeon opts for will depend on their analysis of the literature of various techniques to manage unidentified breaks, their surgical experience, surgical preferences, and patient considerations (age, phakic status, and VA in contralateral eye). Studies analyzing vitreo-retinal surgeons’ current practice would be useful as there does not appear to be a consensus in the literature with respect to the best technique. Our results suggest that trans-scleral injection of dye coupled with DSD is a relatively simple technique that can facilitate the identification of clinically undetectable retinal breaks and can result in anatomical success. In our case series, the technique was applied in the setting of re-detachments; however, the same technique can be used in cases of primary repair if necessary. In this small case series it is not possible to rule out the risk of dye toxicity. An alternative to VB can be used employing the same technique where this particular dye is not licensed for vitreo-retinal use.
The use of trans-scleral VB can be one additional option in vitreo-retinal surgeons’ armamentarium of surgical techniques dealing with unidentified retinal breaks.

References
Lincoff H, Kreissig I . Extraocular repeat surgery for retinal detachment. A minimal approach. Ophthalmology 1996; 103: 1586–1592.
Rachal WF, Burton TC . Changing concepts of failures after retinal detachment surgery. Arch Ophthalmol 1979; 97 (3): 480–483.
Menezo JL, Suarez R, Francés J . Clinical survey of the forms, number and localization of retinal tears in cases of relapses and recurrences in retinal detachment. Ophthalmologica 1977; 174 (4): 210–216.
Rosen PH, Wond HC, McLeod D . Indentation microsurgery: internal searching for retinal breaks. Eye 1989; 3: 277–281.
Jackson TL, Kwan AS, Laidlaw AH, Aylward W . Identification of retinal breaks using subretinal trypan blue injection. Ophthalmology 2007; 114: 587–590.
Wong R, Gupta B, Aylward GW, Laidlaw DA . Dye extrusion technique (DE-TECH): occult retinal break detection with subretinal dye extrusion during vitrectomy for retinal detachment repair. Retina 2009; 29 (4): 492–496.
Kim JH, Bertram KM, Quirk MT, Arroyo JG . Modified external needle drainage of subretinal fluid in primary rhegmatogenous retinal detachment: a prospective, consecutive, interventional, single-surgeon study. Retina 2007; 27 (9): 1231–1237.
Veckeneer M, van Overdam K, Monzer J, Kobuch K, van Marle W, Spekreijse H et al. Ocular toxicity study of typan blue injected into the vitreous cavity of rabbit eyes. Graefes Arch Clin Exp Ophthalmol 2001; 239: 698–704.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Presented at BEAVRS 2010.
Rights and permissions
About this article
Cite this article
Gupta, D., Ong, J. & Burton, R. Trans-scleral dye injection during vitreous surgery to identify clinically undetectable retinal breaks causing retinal detachment. Eye 25, 1045–1049 (2011). https://doi.org/10.1038/eye.2011.117
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2011.117
Keywords
This article is cited by
-
Modified subretinal dye extrusion technique (MORE-DETECH): subretinal diluted trypan blue for detecting occult retinal breaks in retinal detachment after endotamponade removal
International Ophthalmology (2013)
-
Dye toxicity in the context of recurrent retinal detachment repair
Eye (2012)
-
Potential damage to a potential space
Eye (2012)
