
Abstract
Elevated serum urate levels lead to gout and are associated with hypertension, metabolic syndrome, type 2 diabetes and cardiovascular diseases. The purpose of this study was to identify evidence for genetic linkage with serum urate and to determine whether variation within positional candidate genes is associated with serum urate levels in a non-European population. Genetic linkage analysis and single nucleotide polymorphism (SNP) genotyping was performed in a large family pedigree cohort from Mauritius. We assessed associations between serum urate levels and 97 SNPs in a positional candidate gene, SLC2A9. A genome-wide scan identified a new region with evidence for linkage for serum urate at 4p15.3. SNP genotyping identified significant association between six SNP variants in SLC2A9 and serum urate levels. Allelic and gender-based effects were noted for several SNPs. Significant correlations were also observed between serum urate levels and individual components of metabolic syndrome. Our study results implicate genetic variation in SLC2A9 in influencing levels of serum urate over a broad range of values in a large Mauritian family cohort.
Similar content being viewed by others


Introduction
Hyperuricemia is associated with, and often precedes, several cardiovascular disease (CVD) risk factors including hypertension, inflammation, dyslipidemia, kidney disease, obesity, insulin resistance and metabolic syndrome.1 Furthermore, increased serum urate has been shown to be an independent risk factor for CVD in high-risk individuals.2
Urate (uric acid) is the end product of purine metabolism in humans due to the evolutionary loss of hepatic urate oxidase (uricase) activity. This loss of enzymatic function has led to uniquely high serum urate levels compared with other mammals.3 In humans, several factors can lead to increased levels of serum urate (hyperuricemia) as a result of elevated generation and decreased excretion. These include high dietary intake of purines, high fructose intake, alcohol consumption, impaired renal excretion of urate and defective purine metabolism due to genetic disorders, such as hypoxanthine guanine phosphoribosyltransferase deficiency.4
Given the significant health consequences of variation in serum urate, we sought to understand the mechanisms controlling its levels. In this article, we present the results of our genetic linkage analysis that has identified a novel quantitative trait locus influencing serum urate levels at 4p15.3. Notably, recent genome-wide association studies have identified a strong positional candidate gene, SLC2A9, in this region.5, 6, 7 In this study, we aim to characterize the genetic variation contributing to the linkage signal observed at 4p15.3 by single nucleotide polymorphism (SNP) genotyping the positional candidate SLC2A9 in the Mauritius Family Study population. The Mauritius Family Study focuses on large family pedigrees from a subset of the Mauritian population to minimize heterogeneity and environmental effects.
Materials and methods
Ethics statement
The project was submitted to and approved by the International Diabetes Institute Ethics Committee and the SSR Centre for Medical Studies and Research Ethics Committee in Mauritius.
Subjects and genotyping
The Mauritian Family Study consisted of a cohort of 399 individuals in 20 large extended pedigrees.8 Descriptive statistics of the Mauritius Family Study participants in the genome-wide scan are shown in Table 1. The participants in this study were genotyped for an autosomal genome-wide scan that incorporated up to 762 microsatellite markers per individual with an average spacing across the genome of 4.5 cM. The markers were genotyped on an ABI 3100 Genetic Analyzer (Applied Biosystems, Foster City, CA, USA) according to standard protocols and analyzed with GeneMapper version 2.0 software. The average heterozygosity of these markers was 0.75. SNP genotyping was carried out using the MassARRAY system (Sequenom, San Diego, CA, USA) according to the manufacturer's protocol.
Linkage and association analysis
The Sequential Oligogenic Linkage Analysis Routines (SOLAR) software package9 was used for all statistical analysis on related individuals using the variance component-based approach. Heritability analysis, allele sharing, multipoint analysis and linkage analysis were performed on the full data set. Maximum likelihood techniques that account for pedigree structure were used to estimate allele frequencies for SLC2A9. Similarly, SOLAR was used to perform tests of Hardy–Weinberg equilibrium allowing for non-independence among pedigree members. Multivariant methods generally require that individuals with missing data be excluded from the analysis, which can result in a significant decrease in sample size. To minimize this issue, we use likelihood-based imputation with the Merlin computer package (Ann Arbor, MI, USA),10 which uses an adaptation of the method by Burdick et al11 to impute SNP data in pedigrees rapidly. The association model that we have used represents a simple extension of the classical variance component model described more fully elsewhere12, 13 to correct for the effect of multiple testing for a given phenotype, we estimated the effective number of SNPs using the method of Li and Ji.14
Results
Genome-wide scan identifies strong evidence for linkage to chromosome 4p15. 3
Pedigree-based variance components linkage analysis using the computer package Solar (San Antonio, TX, USA)9 was used to search the genome for quantitative trait loci (QTLs) influencing the quantitative trait underlying serum urate. Covariate effects such as sex, age and smoking history were simultaneously evaluated with genetic effects.
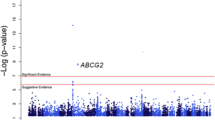
Significant evidence for linkage with serum urate was observed at the cytogenetic location 4p15.3, with a logarithm of odds (LOD) score of 3.7 at 31.3 Mb. The nearest marker for this peak was D4S2912. Figure 1a depicts two other regions that showed suggestive linkage at 1q24 (LOD=2.0 at 145.7 Mb) and 7q36 (LOD=2.1 at 149.8 Mb) according to the definitions determined by Lander and Kruglyak.15 Figure 1b shows the detailed linkage analysis results for chromosome 4. A strong gender effect was observed in the linkage study (covariate gender P-value=1.36 × 10−6).

(a) String plot showing linkage peaks and logarithm of odds (LOD) scores for serum urate. (b) Genome-wide linkage scan. LOD peak for serum urate and position of candidate gene SLC2A9 in chromosome 4.
Previous studies have shown association between variants in SLC2A9 and serum urate levels in European populations.6 SLC2A9 lies within a 2 LOD confidence interval of our QTL peak. Therefore, SLC2A9 was selected as the strongest positional candidate gene and was characterized further using genetic variation analysis in the Mauritius Family Study cohort. We observed heritability at 38% for serum urate (data not shown).
Genotyping of SNPs within the positional candidate gene SLC2A9
A total of 97 annotated SNPs were selected in SLC2A9 for genotyping based on the relative position of the variant to the gene's structure and hence its potential for conferring a functional consequence. Out of 97 SNPs, 56 were found to be polymorphic in the founder (n=92) population. This result is not unusual as NCBI and HapMap databases are generally skewed toward European and Asian populations which do not reflect the ethnic background of Mauritius. The pattern of linkage disequilibrium (LD) measured by the absolute correlation (ρ) of polymorphic SNPs in SLC2A9 (Supplementary Figure 1) appears to be mostly random. On the basis of evaluation of the eigenstructure of the correlation matrix among markers,16 we calculated the effective number of independent SNPs to be 29.1.
Six SNPs showed a significant nominal association with serum urate levels in the founder population and were genotyped in the full cohort (n=399). Of these, rs6449213 showed the strongest association with serum urate (P=0.0013) that remained significant after adjustment for multiple testing with target α at 0.002 (Table 2a). Other SNPs showing nominal association with serum urate are shown in Table 2a. These six SNPs account for ∼4% of the total variation in urate levels. The associations remained significant and changed only marginally after adjustment for BMI (Table 2b), suggesting that the relationships are independent of BMI and are consistent with a lack of correlation to BMI (Supplementary Table 1). To test this, we performed conditional linkage analysis with these SNPs. Consistent with previous studies,5 we also observed a strong gender-specific effect of allelic variation for the association with serum urate in rs6449213 when adjusted for age and BMI (Table 2b).
Incorporation of the rs6449213 variant into the linkage model marginally affected the linkage peak, however it retained statistical significance, suggesting there is another variant or variants in this region contributing to the observed linkage peak and altering serum urate levels (data not shown).
Correlation coefficients between serum urate levels and components of metabolic syndrome were significant at the P<0.01 level using traits from the WHO definition and National Cholesterol Education Program – Adult Treatment Panel III (NCEP-ATPIII) including abdominal obesity, plasma glucose, waist/hip ratio, systolic and diastolic blood pressure, HDL-cholesterol and triglycerides (Supplementary Table 1). No correlation was observed between serum urate and BMI.
Discussion
Serum urate is a predictor of cardiovascular disease. Increased serum urate has been shown to be an independent risk factor for CVD in high-risk individuals.2 To better understand the mechanisms that control serum urate levels, we undertook a genome-wide linkage scan identifying three novel loci at 4p15, 1q24 and 7q36. As a result of the genetic background of Mauritius, our study results do not overlap with a recent genome-wide linkage scan in Mexican Americans that identified a QTL regulating serum urate at 3p2617 and therefore identify additional genetic factors influencing serum urate.
Within the 4p15 QTL lies SLC2A9, a strong positional candidate identified by literature database mining and previously published association by genome-wide association studies. We typed 97 SNPs in SLC2A9 in the Mauitius Family Study cohort and found six SNPs strongly associated with serum urate levels after adjustment for multiple testing. Several of these associations are consistent with previously published genome-wide association studies. Brandstatter et al5 report strong associations with serum urate for rs6855911, rs644921 and rs7442295 in Bruneck study. Associations were reported for rs6855911 and rs7442295 in SardiNIA and InCHIANTI cohorts6 and Wallace et al7 reported an association for rs7442295 in the GRAPHIC, BRIGHT and TwinsUK cohorts. In each of these studies, consistent with our study results, the direction of the effect showed decreased serum urate levels with each copy of the minor allele and P-values for association with urate ranged from 10−9 to 10−13. Our work shows that these SNPs are associated with serum urate across a range of genetic backgrounds including Mauritius.
We observed a strong allele effect for several SNPs associated with serum urate in SLC2A9. In the SNPs rs6449213, rs6855911, rs16890979, rs938552 and rs938554, serum urate was significantly reduced in individuals homozygous for the minor allele by up to 30% when compared with serum urate levels in individuals homozygous for the major allele. For rs7442295, serum urate was raised significantly with the minor allele.
A strong gender-based effect was noted for rs6449213. For this SNP, females account for the majority of variation in serum urate with up to 38% reduction in serum urate for individual females carrying the minor allele. Interestingly, 10 out of 13 (77%) women in the Mauritius cohort with hyperuricemia, defined as serum urate >365.8 μmol/l, are homozygous for the major allele. The findings of an independent study suggest that the increased serum urate levels noted here would increase the risk of mortality from ischemic heart disease in women by almost 2%.18
Two of the SNPs associated with serum urate, rs938552 and rs938554, are in high LD with each other. These SNPs are not located within the exon structure of SLC2A9 but are found in an internal locus, designated LOC100131256, in intron 7 of the gene. Although these SNPs are associated with serum urate levels, and contribute to the linkage peak in the genome-wide scan, no functional inference can be made as the properties of this locus are currently unknown.
Significant correlations were observed between serum urate levels and individual components of metabolic syndrome (Supplementary Table 1). Components of metabolic syndrome were chosen from the WHO and NCEP-ATPIII definitions and all traits were correlated except BMI. This may be due to the fact that abdominal obesity is more highly correlated with metabolic risk factors than BMI, which is further supported by the observed correlation between abdominal obesity and serum urate levels. Despite the correlation between fasting plasma glucose and serum urate levels, hyperglycemia is unlikely to cause the distinct gender differences noted in this study as HbA1c levels in the study population were almost identical between genders (data not shown).
Our studies describe an association between genetic variants in the SLC2A9 gene and serum urate levels in the Mauritian population. Several of these variants show a distinct gender bias. Although there are clear correlations between serum urate levels and components of metabolic syndrome, a causal role for serum urate is yet to be elucidated.
References
Heinig M, Johnson RJ : Role of uric acid in hypertension, renal disease, and metabolic syndrome. Cleve Clin J Med 2006; 73: 1059–1064.
Nakagawa T, Kang DH, Feig D et al: Unearthing uric acid: an ancient factor with recently found significance in renal and cardiovascular disease. Kidney Int 2006; 69: 1722–1725.
Wu XW, Muzny DM, Lee CC, Caskey CT : Two independent mutational events in the loss of urate oxidase during hominoid evolution. J Mol Evol 1992; 34: 78–84.
Johnson RJ, Kang DH, Feig D et al: Is there a pathogenetic role for uric acid in hypertension and cardiovascular and renal disease? Hypertension 2003; 41: 1183–1190.
Brandstatter A, Kiechl S, Kollerits B et al: Sex-specific association of the putative fructose transporter SLC2A9 variants with uric acid levels is modified by BMI. Diabetes Care 2008; 31: 1662–1667.
Li S, Sanna S, Maschio A et al: The GLUT9 gene is associated with serum uric acid levels in Sardinia and Chianti cohorts. PLoS Genet 2007; 3: e194.
Wallace C, Newhouse SJ, Braund P et al: Genome-wide association study identifies genes for biomarkers of cardiovascular disease: serum urate and dyslipidemia. Am J Hum Genet 2008; 82: 139–149.
Jowett JB, Diego VP, Kotea N et al: Genetic influences on type 2 diabetes and metabolic syndrome related quantitative traits in Mauritius. Twin Res Hum Genet 2009; 12: 44–52.
Almasy L, Blangero J : Multipoint quantitative-trait linkage analysis in general pedigrees. Am J Hum Genet 1998; 62: 1198–1211.
Abecasis GR, Cherny SS, Cookson WO, Cardon LR : Merlin – rapid analysis of dense genetic maps using sparse gene flow trees. Nat Genet 2002; 30: 97–101.
Burdick JT, Chen WM, Abecasis GR, Cheung VG : In silico method for inferring genotypes in pedigrees. Nat Genet 2006; 38: 1002–1004.
Blangero J, Goring HH, Kent Jr JW et al: Quantitative trait nucleotide analysis using Bayesian model selection. Hum Biol 2005; 77: 541–559.
Boerwinkle E, Chakraborty R, Sing CF : The use of measured genotype information in the analysis of quantitative phenotypes in man. I. Models and analytical methods. Ann Hum Genet 1986; 50: 181–194.
Li J, Ji L : Adjusting multiple testing in multilocus analyses using the eigenvalues of a correlation matrix. Heredity 2005; 95: 221–227.
Lander E, Kruglyak L : Genetic dissection of complex traits: guidelines for interpreting and reporting linkage results. Nat Genet 1995; 11: 241–247.
Cheverud JM : A simple correction for multiple comparisons in interval mapping genome scans. Heredity 2001; 87: 52–58.
Voruganti VS, Nath SD, Cole SA et al: Genetics of variation in serum uric acid and cardiovascular risk factors in Mexican Americans. J Clin Endocrinol Metab 2009; 94: 632–638.
Freedman DS, Williamson DF, Gunter EW, Byers T : Relation of serum uric acid to mortality and ischemic heart disease. The NHANES I Epidemiologic Follow-Up Study. Am J Epidemiol 1995; 141: 637–644.
Acknowledgements
We acknowledge the work of Jianmin Wang, Sally Dennis and the Australian Genome Research Facility for their contribution to genotyping data. This study was undertaken with the support and collaboration of the Mauritius Ministry of Health and Quality of Life, their health community workers and staff at the SSR Centre, University of Mauritius without which this study would not have been possible. We also thank the individuals and families who participated in the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on European Journal of Human Genetics website
Supplementary information
Rights and permissions
About this article
Cite this article
Cummings, N., Dyer, T., Kotea, N. et al. Genome-wide scan identifies a quantitative trait locus at 4p15.3 for serum urate. Eur J Hum Genet 18, 1243–1247 (2010). https://doi.org/10.1038/ejhg.2010.97
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejhg.2010.97
Keywords
This article is cited by
-
The association between genetic polymorphisms in ABCG2 and SLC2A9 and urate: an updated systematic review and meta-analysis
BMC Medical Genetics (2020)
-
Genetic variation in SH3-domain GRB2-like (endophilin)-interacting protein 1 has a major impact on fat mass
International Journal of Obesity (2012)
