
Abstract
Background:
As breast cancer and its treatment are likely to interfere with traditional expectations of womanhood, it may affect marital stability.
Methods:
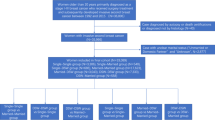
The risk of marital dissolution was analysed with respect to diagnosis of early-stage (T1–4N0–3M0) breast cancer in a cohort of 134 435 married Finnish women followed for a median of 17.0 married years. Age, socioeconomic status, education, number of children, duration of marriage and earlier marriages were taken into account and the effects of surgery, chemotherapy, radiotherapy and endocrine therapy were analysed separately.
Results:
Women with a diagnosis of early-stage breast cancer did not show increase in marital dissolution (hazard ratio=0.96, 95% confidence interval=0.79–1.17). Neither the type of surgical procedure nor any of the oncologic treatments was associated with an increase in the risk of divorce.
Conclusions:
Any evidence of excess risk of marital breakdown after the diagnosis of early-stage breast cancer and its treatment was not demonstrated.
Similar content being viewed by others


Main
An early-stage breast cancer and its treatment create an individual set of stress for women (Senkus et al, 2013; von Heymann-Horan et al, 2013). Menopausal symptoms, depression and fatigue are found to be common soon after breast cancer adjuvant treatment (Penttinen et al, 2011) and may persist for years. However, the earlier diagnosis of an early-stage breast cancer because of increased coverage of mammography screening programmes and improvement of adjuvant therapies have led to better prognosis (Yalcin, 2013) that may reduce the stress associated with breast cancer.
Concurrent with the improvement of its prognosis, an increasing number of couples are affected by early-stage breast cancer. At the same time, marriages in Europe and in North America have become less stable (Jalovaara, 2013). This also raises interest towards breast cancer in terms of family relations and marital stability. We analysed the effect of an early-stage breast cancer and its modern treatment on long-term marital stability while taking into account a comprehensive set of cancer-related and socioeconomic variables.
Materials and methods
Study population and follow-up
The women of this study were selected from the Finnish population register that contains detailed sociodemographic information of the whole Finnish population. An 11% random sample of women who were at least 18 years, married either at the beginning of the study or later during the follow-up and permanently residing in Finland at the end of any of the years between 1987 and 2007 was used.
The study population was followed from the beginning of 1996, that is, a year after national information on each individual’s medicine purchases was available, until divorce or until the end of the year 2012, yielding the median follow-up of 17.0 married years. The follow-up time started at the beginning of 1996 for all women who were married at that time and not previously diagnosed with breast cancer. For those who were married later, the follow-up time started when they married. Censoring occurred if the person died, was widowed or diagnosed with a metastatic breast cancer. Age at the beginning of follow-up, occupational-based socioeconomic status (SES), education, number of children under 18 years of age living in the same household, duration of marriage and the number of earlier marriages were used as confounding variables. Those who divorced before diagnosis (N=210) were included in the reference group.
Three other nation-wide registers that are explained below were linked with the data extracted from the population register. The study protocol was approved by the Ethics Committee of Statistics Finland (permission TK-53-1783-96).
Breast cancer and treatment
The incidence of breast cancer was derived from the Finnish Cancer Registry that contains a nation-wide database based on structured notifications required from all cancer cases that come to attention in Finland (Finnish Cancer Registry, 2014). Only women with primary diagnosis of an early-stage breast cancer, that is, breast cancers without distant metastasis (only local breast cancers and those with metastasis in regional lymph nodes only, i.e., T1–4N0–3M0) during follow-up were included. If a person faced more than one early-stage breast cancer during the study period, the first was chosen as a reference.
Information on adjuvant chemotherapy and radiotherapy was derived from the Finnish Cancer Registry records. As the use of antioestrogens and aromatase inhibitors in the treatment of breast cancer is fully reimbursable in Finland, the use of endocrine therapy was derived from the National Social Insurance Institution that compiles comprehensive data of each individual’s medicine purchases.
The type of surgical treatment, that is, breast-conserving surgery (BCS) vs mastectomy, was derived from the Finnish Hospital Discharge Register (FHDR) provided by the National Institute for Health and Welfare that contains nation-wide information on all inpatient hospital discharges since 1969. Considering the universal health-care system in Finland, FHDR is likely to cover virtually all oncologic surgery cases in Finland.
Statistical methods
Cox proportional hazards regression models were used to assess how a diagnosis of an early-stage breast cancer was associated with the risk of divorce measured as hazard ratios (HRs). Breast cancer diagnosis was treated as a time-dependent variable, that is, women were allowed to have different hazard for divorce before and after the breast cancer diagnosis. First, the effect of each sociodemographic variable was analysed separately. Second, the risk of divorce among women with an early-stage breast cancer was analysed with respect to each treatment. Age at the beginning of follow-up was divided in the 5-year categories and used as a strata variable allowing own baseline hazard in each category and also included as a continuous covariate taking into account any linear age effects within the strata. Stata/SE 9.2 statistical software was used for all analyses (StataCorp LP, College Station, TX, USA).
Results
The characteristics of the whole study population at the beginning of follow-up are shown in Table 1. The median duration of marriage from the beginning of marriage until the end of follow-up or divorce was 31 years and its lower and upper quartiles were 14 and 47 years. A total of 2.4% of women were diagnosed with an early-stage breast cancer. The type of surgery followed by breast cancer diagnosis and oncologic treatments are summarised in Table 2.
Among the whole study population, women who were living with children were less likely to divorce during the follow-up (HR=0.98, 95% CI=0.93–1.03 for those who had one child, HR=0.82, 95% CI=0.78–0.86 for those who had two or three children, HR=0.96, 95% CI=0.89–1.02 for those who had three to five children and HR 0.46, 95% CI=0.39–0.55 for those who had more than 5 children) when adjusted for age. Higher SES (HR=1.12, 95% CI-1.07–1.18 for lower nonmanual workers compared with higher) and higher education (HR=1.12, 95% CI=1.08–1.16 for primary and HR=1.40, 95% CI=1.34–1.45 for secondary education compared with those who had tertiary education) were both associated with higher marital stability. Each year of marital duration decreased the risk of divorce (HR=0.98, 95% CI=0.98–0.99). A higher risk of divorce was observed among those who were married for the second (HR=1.86, 95% CI=1.77–1.95) or the third or more time (HR=2.85, 95% CI=2.49–3.25) compared those who were married for the first time.
Women with an early-stage breast cancer did not show any increase in the risk of divorce in general when compared with women without breast cancer (HR=0.98 95% CI=0.80–1.18) when adjusted for age at baseline. This finding remained when adjusted for SES, education, duration of marriage at baseline, number of children and number of previous marriages (HR=0.96, 95% CI=0.79–1.17).
Surgical procedure or any oncologic treatment was not associated significantly with the risk of divorce (Table 3). In addition, breast reconstructive surgery did not show a significant effect on the risk of divorce. With the purpose of investigating the effect of the heaviest adjuvant therapy, the risk of women who received chemotherapy, radiotherapy and endocrine therapy was analysed separately (HR=1.01, 95% CI=0.66–1.55) as compared with women without breast cancer. Finally, HRs with 95% CIs of divorce in relation to time were calculated with the purpose to investigate whether there was any time period associated with a special vulnerability for marital dissolution after diagnosis of early-stage breast cancer. However, supportive evidence was not demonstrated (Figure 1).

Hazard ratio and 95% confidence interval of divorce in relation to time after diagnosis of early-stage breast cancer among married Finnish women. Adjusted for age, SES, education and having any children.
Discussion
This study was performed in order to investigate the stability of previous marriages after diagnosis of early-stage cancer. The factors constituting marital stability are likely to be many, and cannot be fully controlled in epidemiological studies such as this study. However, our study design enabled us to investigate this association in a large cohort of Finnish women, and took account the most important sociodemographic (Torkild and Jalovaara, 2010) and cancer-related variables that are likely to have a role in this multifactorial interplay. In this study we focussed on women with a local- and regional-stage breast cancer, as their prognosis is good and treatment is widely based on international guidelines in Finland such as in other countries (Senkus et al, 2013). Metastatic breast cancers were not included, as their prognosis is worse and they may cause different kind of stress for each partner and more prominent physical symptoms.
The association between cancer and marital stability has been only little studied. A cautious suggestion is that cancers with a relatively high incidence already in early adulthood and with a potential effect on reproduction such as cervical cancer may more likely have an adverse effect on partnership stability (Carlsen et al, 2007). This risk was found to be even higher among younger women after the diagnosis of cervical cancer (Syse, 2007). However, men who had been diagnosed with a testicular cancer, the incidence of which is also higher already at younger ages, did not show any increase in risk, although they reported more sexual dysfunction and infertility (Rieker et al, 1989; Joly et al, 2002; Carlsen et al, 2007).
There are three previous studies among married women with an early-stage breast cancer diagnosed before 2002. None of them demonstrated a significant increase in the risk of divorce compared with women without breast cancer (Dorval et al, 1999; Carlsen et al, 2007; Syse, 2007). However, the motives for longtime marital stability and the attitudes towards breast cancer are likely to be both time and society dependent, highlighting the importance of later studies. The results of our study support the findings of previous studies. Moreover, they were consistent in all subgroups independent of cancer, treatments, which was not demonstrated earlier. As our data were not large enough to perform these analyses separately among women <30 years of age and none of the earlier studies either did so, the question of whether there could be a risk increase only among the youngest women remains unclear.
The effects of breast surgery and oncologic treatments are likely to be intimate for women. For instance, the toxic effects of chemotherapy and endocrine therapy are likely to interfere with body image and sexuality, and may also compromise one’s reproductive capability at early age. Nevertheless, either type of surgeries or oncologic treatments did not modify the risk of divorce. However, as decision of treatments are usually based on stage of primary tumour and characters of each patient, which we were not able to control fully, these results are more likely to reflect not only the effects of the treatments but also a group of women who were selected to receive them. Thus, we combined those oncologic treatments that are more likely to cause general symptoms (i.e., chemotherapy and/or endocrine treatments) and those who not (i.e., radiotherapy or no adjuvant treatment) and also analysed association in these categories. The risk of divorce was also analysed separately in women who received all three treatment and were also likely to have the most aggressive primary tumours. However, the risk of divorce was not increased even among women who received a combination of all three oncologic treatments.
Information on breast cancer and its oncologic treatment was based on structured notifications made by physicians with an exception of endocrine therapy that was derived from the National Social Insurance Institution. The notifications to Cancer Registry are usually made 1–2 years after diagnosis, when the information of chemotherapy and radiotherapy should be available. Though the coverage of Cancer Registry is likely to be incomplete, the potential lack of information is likely to be nondependent on marital status and given oncologic treatments. Unfortunately, bilateral and hereditary breast cancers could not be identified, though they may cause more marital hardship.
The ratio of divorces to new marriages in Finland corresponds to the average of European Union and is comparable to that in the United States (Statistics Finland, 2014). As the gender equality in Finland in terms of earned income and labor force participation is high (Hausmann et al, 2013), and the public welfare system is aimed at guarantee treatment equality, the economic consequences of potential union dissolution should not be a major for most Finnish women. Indeed, a strong association between women higher education/SES and greater marital stability in Finland and in other countries with strong emphasis on gender equality has been demonstrated (Cooke, 2006; Jalovaara, 2013).
In summary, according to this study, there is no increase in the risk of divorce after the diagnosis of an early-stage breast cancer even among women receiving an adjuvant treatment with the most unpleasant side effects. In addition, the type of breast surgery does not seem to modify the risk of divorce. Thus, from the optimistic point of view, an early-stage breast cancer can be considered as a transient stressor for individual and partnership well-being. This can be considered encouraging for women with a current diagnosis of breast cancer and health-care professionals supporting them along the adjuvant treatment and follow-up.
Change history
28 July 2015
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Carlsen K, Dalton SO, Frederiksen K, Diderichsen F, Johansen C (2007) Are cancer survivors at an increased risk for divorce? A Danish cohort study. Eur J Cancer 43: 2093–2099.
Cooke LP (2006) Household bargaining and the risk of divorce in Germany and the United States. Am J Sociol 112: 442–472.
Dorval M, Maunsell E, Taylor-Brown J, Kilpatrick M (1999) Marital stability after breast cancer. J Natl Cancer Inst 91: 54–59.
Finnish Cancer Registry (2014) Notification to the Finnish cancer Registry. Available at http://www.cancer.fi/@Bin/100897742/2014lomakekleng+unionin.pdf.
Hausmann R, Tyson LD, Bekhouche Y, Zahidi S (2013) The Global Gender Gap Report 2013. World Economic Forum 49–57, Available at http://www3.weforum.org/docs/WEF_GenderGap_Report_2013.pdf.
Jalovaara M (2013) Socioeconomic resources and the dissolution of cohabitations and marriages. Eur J Population 29: 167–193.
Joly F, Heron JF, Kalusinski L, Bottet P, Brune D, Allouache N, Mace-Lesec'h J, Couette JE, Peny J, Henry-Amar M (2002) Quality of life in long-term survivors of testicular cancer: a population-based case-control study. J Clin Oncol 20: 73–80.
Penttinen HM, Saarto T, Kellokumpu-Lehtinen P, Blomqvist C, Huovinen R, Kautiainen H, Jarvenpaa S, Nikander R, Idman I, Luoto R, Sievanen H, Utriainen M, Vehmanen L, Jaaskelainen AS, Elme A, Ruohola J, Luoma M, Hakamies-Blomqvist L (2011) Quality of life and physical performance and activity of breast cancer patients after adjuvant treatments. Psychooncology 20: 1211–1220.
Rieker PP, Fitzgerald EM, Kalish LA, Richie JP, Lederman GS, Edbril SD, Garnick MB (1989) Psychosocial factors, curative therapies, and behavioral outcomes. A comparison of testis cancer survivors and a control group of healthy men. Cancer 64: 2399–2407.
Senkus E, Kyriakides S, Penault-Llorca F, Poortmans P, Thompson A, Zackrisson S, Cardoso F ESMO Guidelines Working Group (2013) Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 24: 7–23.
Statistics Finland (2014) Marriages and Divorces in 1965–2013. Available at http://www.stat.fi/til/ssaaty/2013/ssaaty_2013_2014-04-17_tie_001_en.html.
Syse K (2007) Does cancer affect the divorce rate? Demogr Res 16: 469–492.
Torkild L, Jalovaara M (2010) A review of the antecedents of union dissolution. Demogr Res 23: 257–292.
von Heymann-Horan AB, Dalton SO, Dziekanska A, Christensen J, Andersen I, Mertz BG, Olsen MH, Johansen C, Bidstrup PE (2013) Unmet needs of women with breast cancer during and after primary treatment: a prospective study in Denmark. Acta Oncol 52: 382–390.
Yalcin B (2013) Staging, risk assessment and screening of breast cancer. Exp Oncol 35: 238–245.
Acknowledgements
This study was supported by the Academy of Finland (Grants 255592, 264539 and 25569).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution-NonCommercial-Share Alike 4.0 Unported License.
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 4.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/4.0/
About this article

Cite this article
Laitala, V., Saarto, T., Einiö, E. et al. Early-stage breast cancer is not associated with the risk of marital dissolution in a large prospective study of women. Br J Cancer 113, 543–547 (2015). https://doi.org/10.1038/bjc.2015.216
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2015.216
