
Abstract
OBJECTIVES: The optimal method for epinephrine administration during neonatal resuscitation is not known. We hypothesized that epinephrine will be delivered more efficiently when administered via a feeding catheter inserted into the endotracheal tube (C-ETT) vs when administered directly into the ETT (D-ETT). Our objectives were to (1) compare the delivery of epinephrine to the distal end of the ETT when administered via D-ETT vs C-ETT; (2) measure the retention of epinephrine within the ETT vs the feeding catheter used for the drug delivery; and (3) compare the delivery of the drug with and without an air flush after administration via C-ETT.
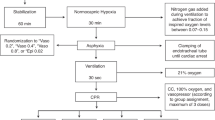
METHODS: All experiments were performed in vitro, simulating epinephrine administration during neonatal resuscitation, according to the standard guidelines. Radiolabeled epinephrine, diluted to 1 μCi/ml, was used and experiments were repeated at least 4 times. Epinephrine administration via D-ETT was followed by one manual breath via a self-inflating bag attached to the ETT. Epinephrine delivery via C-ETT was followed by 1 ml saline flush, and in some experiments, this was also followed by a 1 cm3 air flush. Epinephrine delivery and retention were assessed by measuring the radioactive content of the effluent fluid and that of the ETT or of the feeding catheter used for drug delivery.
RESULTS: Significantly higher dosage of the drug was delivered when administered via D-ETT vs C-ETT, if air flush following C-ETT method was not used. However, with an air flush following the saline flush after the drug instillation, there was no difference in the amount of epinephrine delivered between the two methods. Retention in the ETT wall or the catheter was <7.5% of the administered dose with either method.
CONCLUSIONS: Without an air flush following C-ETT method of epinephrine delivery, higher dosage of the drug is delivered via D-ETT vs C-ETT method. An air flush following the saline flush during C-ETT method improves drug delivery. Given that the C-ETT method is more cumbersome and time consuming, and does not improve drug delivery, D-ETT administration should be the method of choice for epinephrine delivery during neonatal resuscitation.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout





Similar content being viewed by others

References
Kattwinkel J, editor. Textbook of Neonatal Resuscitation. 4th Ed. Elk Grove Village, IL: American Academy of Pediatrics and American Heart Association; 2000, p 6-4–6-7.
McCrirrick A, Kestin I . Hemodynamic effects of tracheal compared with intravenous adrenaline. Lancet 1992;340:868–870.
Quinton DN, O'Byrne G, Aitkenhead AR . Comparison of endotracheal and peripheral intravenous adrenaline in cardiac arrest. Lancet 1987;1:828–829.
Burchfield DJ, Preziosi MP, Lucas VW, et al. Medication use in neonatal resuscitation: epinephrine, sodium bicarbonate. Neonatal Pharmacol 1993;Q 2:2.
Kleinman ME, Oh W, Stonestreet BS . Comparison of intravenous and endotracheal epinephrine during cardiopulmonary resuscitation in newborn piglets. Crit Care Med 1999;27:2748–2754.
Mielke LL, Lanzinger MJ, Entholzner EK, Hargasser SR, Hipp RFJ . The time required to perform different methods for endotracheal administration during CPR. Resuscitation 1999;40:165–169.
Jasani MS, Nadkarni VM, Finkelstein MS, et al. Effects of different techniques of endotracheal epinephrine administration in pediatric porcine hypoxic-hypercarbic cardiopulmonary arrest. Crit Care Med 1994;22:1174–1180.
Hörnchen U, Schüttler J, Stoeckel H, et al. Pharmakokinetick and Dynamik von endogen freigesetztem und therapeutisch appliziertem Adrenalin unter Reanimationsbedingungen. Anaesthesist 1988;37:615–619.
Roberts JR, Greenberg MI, Baskin SI . Endotracheal epinephrine in cardiorespiratory collapse. JACEP 1979;8:515–519.
Perlman JM, Risser R . Cardiopulmonary resuscitation in the newborn: associated clinical events. Arch Pediatr Adolesc Med 1995;149:20–25.
Redding JS . Effective route of drug administration during cardiac arrest. Anesthes Analg 1967;46:253–258.
Lindemann R . Resuscitation of the newborn. Endotracheal administration of epinephrine. Acta Pediatr Scand 1984;73:210–212.
Zaritsky A . Endotracheal epinephrine in cardiac arrest. Crit Care Med 1994;22:1071–1072.
Paret G, Vaknin Z, Ezra D, et al. Epinephrine pharmacokinetics and pharmacodynamics following endotracheal administration in dogs: the role of volume diluents. Resuscitation 1997;35:77–82.
Lucas VW, Preziosi MP, Burchfield DJ . Epinephrine absorption following endotracheal administration: effects of hypoxia-induced low pulmonary blood flow. Resuscitation 1994;27:31–34.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Rehan, V., Garcia, M., Kao, J. et al. Epinephrine Delivery during Neonatal Resuscitation: Comparison of Direct Endotracheal Tube vs Catheter Inserted into Endotracheal Tube Administration. J Perinatol 24, 686–690 (2004). https://doi.org/10.1038/sj.jp.7211172
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jp.7211172
