
Abstract
Purpose
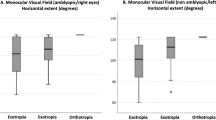
To analyse the difference between measurement of A and V pattern strabismus at 25° and extreme gaze position in esotropia (ET) and exotropia (XT).
Methods
This prospective cross-section study included 27 patients with basic horizontal strabismus associated to any deviation pattern. Mean age was 11.88±9.17 (6–44) years. Exclusion criteria were amblyopia, intermittent XT, noncollaboration with the exam, previous strabismus surgery, craniofacial, or spinal abnormalities. The deviations were measured with prism cover test at 6 m. Measurements were carried out in primary position, upgaze (neck flexion of 25° and maximum flexion) and downgaze (neck extension of 25° and maximum extension). A goniometer with a bubble level controlled the neck position.
Results
The most significant changes were in downgaze. The pattern size increased 4 prism dioptres (PD) or more in 56.25% of the V- and in 87.5% of the A-patterns. The mean increase was 8.00±6.04 PD (0–17 PD) for the A-pattern ET, 4.80±3.70 PD (0–10 PD) for the V-pattern XT, and 6.50±5.58 PD (0–15 PD) for the V-pattern XT. The only case of A-pattern XT increased 8 PD.
Conclusion
Our results suggest that measurements in extreme up and downgazes may uncover increased deviations in a significant proportion of cases. Further studies remain necessary to determine the relevance of these findings for strabismus correction.
Similar content being viewed by others

Introduction
Deviation pattern is the change of the horizontal deviation measured in upgaze, primary position, and downgaze.1 It is usually associated with an oblique muscle dysfunction. Inferior oblique overaction causes a V-pattern and the superior oblique overaction an A-pattern.
The coexistence of an A- or a V-pattern with horizontal strabismus is seen in 12.5–50% of cases.2 The present recommendation is to operate a V-pattern of 15 prism dioptres (PD) or greater and an A-pattern of 10 PD or greater. The surgical planning for oblique muscle weakening varies depending on the degree of overaction of the muscles and the magnitude of the incomitances.3, 4, 5, 6, 7, 8, 9
According to Burian's report, strabismus evaluation in up and downgazes was first suggested by Urrets-Zavalia, in 1948.10 Albert used the terms A- and V-pattern, which have become the most commonly used notations.2
In 1958, Costenbader11 recommended diagnosing the A- and V-patterns based on measurements at 25–30° in up- and downgaze. In the next year, Knapp12 suggested that evaluations over 25° were extreme and could show artificial deviations, recommending the exam at 25°.
In 1964, at the American Academy of Ophthalmology and Othorrinolaringology Meeting, an agreement was made to study the strabismus deviations in up- and downgaze only at 25°.10
In 1965, von Noorden and Olson13 studied, in 60 patients, the implications of the A- and V-pattern measurement in different angles (from 45 up to 55° downgaze) at 33 cm. This study had a limited methodology description, but was the only to look for what actually happens to the A- and V-pattern measurement in extreme positions. They suggested that only the downgaze should be measured at an angle greater than 25°.
In 1971, Jampolsky14 suggested the diagnosis of A- and V-patterns based on the extreme position measurement, aiming not to underestimate the real size of the patterns. This idea was not followed by any publication comparing the different measures.
Based on the knowledge that surgical planning depends on the size of the pattern, considering that surgery aims for fusion in all gaze positions (including over 25°, specially in downgaze) and being the measurement at 25° consecrated without a scientific evidence, it is important to verify the frequency of significant changes in the deviation size with extreme gaze position measures.
The objectives of this study are threefold: (1) to quantify the alphabet pattern size changes with the measurement in extreme gaze positions compared with 25°, (2) to verify the prevalence of significant pattern size changes measured in extreme gaze compared with 25°, (3) and to analyse the measurement changes in esotropia (ET) and exotropia (XT) separately.
Patients and methods
We designed a prospective cross-sectional pilot study. The sample included 27 consecutive patients with horizontal deviation associated with any alphabet pattern. They were seen at Hospital de Clínicas de Porto Alegre from March 2004 to June 2005.
All patients included in this study had the diagnosis of an alphabet pattern made based on the 25° measurement in up- and downgaze. The V-pattern corresponded to a vertical incomitance of at least 15 PD and the A-pattern, an incomitance of at least 10 PD. Exclusion criteria were amblyopia (for the accuracy of the alternate prism cover test), intermittent XT, non-collaboration with the exam, previous strabismus surgery, and craniofacial or spinal abnormalities.
There were 14 male and 13 female patients, with a mean age of 11.88±9.17 (range 6–44) years. All cases presented with corrected visual acuity of 20/25 or better in both eyes. Except for one patient who was myopic (−3.00 D), all the others were hyperopic. The mean spherical equivalent was +1.50±4.6 D. Characteristics of the deviation patterns are shown in Table 1. The ethics committee of Hospital de Clínicas de Porto Alegre approved this study.
The same investigator examined all patients. The esotropes wore full hyperopic or myopic correction, whereas the exotropes wore full myopic correction and the highest hyperopic correction that would allow them to see 20/20 at the Snellen chart. The deviation was measured with alternate prism cover test at 6 m. The target corresponded to a 20/40 optotype at the Snellen chart, and was positioned at the same height as the patient's eyes in primary position of gaze.
The deviation was first measured at primary position, upgaze (neck flexion of 25°) and downgaze (neck extension of 25°). A manual goniometer was used to measure the neck position. A bubble level was taped at one arm of the goniometer to provide more accurate data. The measurements were then repeated with the maximum flexion and extension of the neck that would still allow the patient to fixate at the target. The frames were adjusted to keep the patients seeing through their glasses during the exam. The data registered for each patient corresponded to findings of two agreeing measures.
The mean size of the incomitances and of the deviation measurements in up- and downgaze were calculated. The examination at 25° was compared with the extreme gaze position. The two-sided t-test was used to verify the significance of the results, considering P-value ≤0.05.
Results
The changes of the alphabet patterns size with the measurement in extreme gaze position and their frequencies are shown in Tables 2 and 3.
The deviation patterns evaluated in extreme gaze position were 4 PD or greater than measured at 25° in 56.25% of the V-patterns and in 87.5% of the A-patterns. The mean difference was 6.80±5.33 PD (range of 0–17 PD) in cases with oblique dysfunction, and 5.14±3.89 PD (0–11 PD) in cases without the oblique muscle involvement.
The increase of pattern size with the different measures was 4 PD or more in 50% of the V-pattern ET, 62.5% of the V-pattern XT, 75% of the A-pattern ET, and in 100% of the A-pattern XT.
The upgaze deviation changed at least 4 PD in 30% of the V-pattern ET, in 37.5% of the V-pattern XT, in 62.5% of the A-pattern ET, and in 0% of the only A-pattern XT. In downgaze, this change happened in 20% of the V-pattern ET, in 37.5% of the V-pattern XT, in 75% of the A-pattern ET, and in 100% of the only A-pattern XT.
The up- and downgaze deviation changes with the different measurements of the alphabet patterns and their frequencies are shown in Tables 4, 5 and 6. The only A-pattern XT changed 2 PD in upgaze and 6 PD in downgaze.
Discussion
This is the first study to compare the A- and V-pattern measurement at the classical 25° with the extreme gaze position using a distance target at 6 m.
Previously, von Noorden and Olson13 compared measurements close to 25° (they used 30°) with a bigger angle position (upgaze of 45° and downgaze of 45 and 55°) at 33 cm.
Those authors found the following mean change of the deviations in downgaze (55°): +12 PD in the V-pattern ET, −12 PD in the A-pattern ET, +2 PD in the V-pattern XT, and −7 PD in the A-pattern XT. In upgaze (45°), they found the mean change to be −5 PD in V-pattern ET, +5 PD in A-pattern ET, −10 PD in V-pattern XT, and +1 PD in A-pattern XT.
Our results agree with von Noorden and Olson13 findings of the biggest difference of measurement to be in downgaze and of the smallest difference in downgaze to be in V-pattern XT. In upgaze, our results agree as well, showing the biggest difference in V-pattern XT and the smallest in A-pattern XT. Different from those authors, we found an increased difference of measures in downgaze of the A-pattern ET if compared with the V-pattern ET.
The results of our study were not statistically significant due to the small sample size. It would be necessary to have 99 patients with V-pattern ET, 43 with A-pattern ET, and 21 with V-pattern XT to have a P=0.05 based on this results. The sample size calculation for the A-pattern XT was not reliable as only one case was studied.
von Noorden and Olson,13 based on their results (similar to ours, specially in A-pattern ET), suggested measuring the pattern deviations in a position beyond 25° in downgaze to avoid their underestimation. Despite there being no study proving which angle of measurement is better for the strabismus management, we believe that this idea has a rational basis: if we correct an increasing deviation beyond 25° (angles commonly used in downgaze), we could theoretically provide fusion in more positions of gaze.
In conclusion, our results suggest that measuring the horizontal deviations in extreme up- and downgaze can increase the magnitude of the deviation patterns in a great proportion of cases. However, further studies are needed to prove how much relevance such an increase of measures might mean for the management of patients with A- or V-pattern strabismus.
References
Wright KW . Alphabet patterns and oblique muscle dysfunctions. In: Wright KW, Spiegel PH (eds). Pediatric Ophthalmology and Strabismus. Springer-Verlang: New York, 2003, pp 232–249.
Rosenbaum A, Santiago A . Pattern Strabismus. In: AL Rosenbaum, AP Santiago (eds). Clinical Strabismus Management. WB Saunders Company: Philadelphia, 1999, pp 202–215.
Polati M, Gomi C . Recession and measured graded anterior transposition of the inferior oblique muscles for V pattern strabismus: outcome of 44 procedures in 22 typical patients. Binocul Vis Strab Q 2002; 17 (2): 89–93.
Caldeira JA . V-pattern esotropia: a review; and a study of the outcome after bilateral recession of the inferior oblique muscle: a retrospective study of 78 consecutive patients. Binocul Vis Strab Q 2003; 18 (1): 35–48.
Lee SY, Rosenbaum AL . Surgical results of patients with A pattern horizontal strabismus. J AAPOS 2003; 7 (4): 251–255.
Castanera de Molina A, Fabiani R, Giner MG . Downshoot in infra-adduction following selected superior oblique surgical weakening procedures for A-pattern strabismus. Binocul Vis Strab Q 1998; 13 (1): 17–28.
de Ancos E, Strickler J, Klainguti G . Treatment of alphabetic ‘V’ syndromes. Klin Monatsbl Augenheilkd 1995; 206 (5): 347–350.
Caldeira JA . Graduated recession of the superior oblique muscle. Br J Ophthalmol 1975; 59: 553.
Souza Dias C, Uesugui CF . Efficacy of different techniques of superior oblique weakening in the correction of the ‘A’ anisotropia. J Pediatr Ophthalmol Strab 1986; 23 (2): 82–86.
Burian HM, von Noorden GK . A and V patterns. In: CV Mosby (ed). Binocular Vision and Ocular Motility. The CV Mosby. St Louis, 1974, pp 327–341.
Duke-Elder S, Wybar K . The A, V and X phenomena. In: CV Mosby (ed). Ocular Motility and Strabismus, Vol. 6, The CV Mosby: St Louis, 1973, pp 771–794.
Knapp P . Vertically incomitant horizontal strabismus, the so called A and V syndromes. Trans Am Ophthalmol Soc 1959; 57: 666–699.
von Noorden GK, Olson CL . Diagnosis and surgical management of vertically incomitant horizontal strabismus. Am J Ophth 1965; 60: 434–444.
Jampolsky A . Transactions of the New Orleans Academy of Ophthalmology. The CV Mosby: St Louis, 1971, pp 34–92.
Acknowledgements
There is no financial interest in this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Procianoy, E., Procianoy, L. Prevalence of horizontal deviation pattern changes with measurements in extreme gazes. Eye 22, 229–232 (2008). https://doi.org/10.1038/sj.eye.6702588
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702588
