
Abstract
Data sources
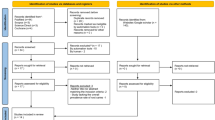
PubMed, Scopus and Embase were searched from 2000 to 2016.
Study selection
A search strategy was developed to identify randomised clinical trials, cross-sectional studies, cohort studies, comparative studies, validation studies and evaluation studies that tested standardised caries risk assessment (CRA) models. There was no restriction with respect to patients' age, but caries data should have been recorded using the Decayed, Missing, Filled Tooth/Surface (DMFT/S) or the International Caries Detection and Assessment System (ICDAS) indices.
Data extraction and synthesis
Two authors independently assessed the papers for inclusion, carried out data extraction and the papers' methodological quality using a customised quality assessment tool developed by the National Heart, Lung and Blood Institute and Research Triangle Institute International for Observational Cohort and Cross-Sectional Studies. For comparison between studies, the caries values were organised in two-by-two tables from which sensitivity, specificity values and their 95% confidence intervals were calculated.
Results
A total of 1239 papers were retrieved of which 32 were included. The most frequent CRA model investigated was the Cariogram. Sixteen studies were carried out on children and 12 on adults. The results showed an association between the risk determined by the model and the actual caries status and/or the development of new carious lesions, this association being statistically significant. With respect to the quality of the studies included in the review, 19 were classified as of good quality, while eight and five were judged as of fair and poor, respectively. On the basis of seven studies, it was observed that Cariogram sensibility varied from 41.0 to 75.0, while its specificity ranged from 65.8 to 88.0.
Conclusions
There is insufficient evidence to assert that CRA models are effective in determining patients' actual caries risk or in predicting their probability of developing new carious lesions. Moreover, the validity of standardised CRA models is still limited.
Similar content being viewed by others
Commentary
To be able to predict whether new carious lesions will occur in the future would have a positive impact on the professional's decision-making process, in particular with regard to preventive measures. Moreover, it would greatly assist him/her in establishing individualised recall intervals, considering the needs of each patient. On the basis of these assumptions, different Caries Risk Assessment (CRA) models have been proposed over the past decades.1, 2, 3 These models vary in many aspects, from the age group to which they can be applied, to the risk and protective factors that are included in each model. Therefore, the aim of this systematic review was to evaluate whether standardised CRA models are able to evaluate the risk according to the actual caries status and/or the future caries increment.
The search strategy included three databases. Only papers in English were assessed. Considering the type of question raised by the authors, it was expected that no randomised clinical trials would be retrieved and this was confirmed by their results. Of the 32 studies included in the review, 15 were prospective cohorts, while the other 17 followed a retrospective (patients' dental charts analysis) or a cross-sectional design. This is important information as the predictive value of the CRA models tested in each study can only be determined by means of a longitudinal assessment. It means that the majority of the studies included in the review were restricted to the assessment of whether the CRA models were able to identify the risk according to individual's actual risk status. This leads us to ponder to what extent an individual who presents with active carious lesions, for example, is at risk; this person already has the disease. In this context, the use of a CRA model can be considered a tool for patient health education by identifying the risk factors that are involved in the onset of the disease.
In terms of predicting new carious lesions, two points need to be taken into consideration. Firstly, of the 15 prospective studies included in this review, 13 tested the Cariogram,1 highlighting the scarcity of studies that assessed other CRA models, which in turn is related to the lack of validation of these models. Secondly, even for Cariogram the results were not consistent. While some studies demonstrated its ability in predicting new lesions,4, 5 others failed.6 This might be explained by the multifactorial nature of dental caries, in which certain risk factors that are not included in the model (eg socioeconomic status or ethnicity) may play an important role for the onset of the disease in a certain population and are not so relevant for another one. Thus, based on the analysis of the papers included, the authors concluded that the evidence related to the effectiveness of standardised CRA models is still limited.
References
Bratthall D, Petersson G . Cariogram - a multifactorial risk assessment model for a multifactorial disease. Community Dent Oral Epidemiol 2005; 33: 256–264.
Featherstone JD, Adair SM, Anderson MH, et al. Caries management by risk assessment: consensus statement, April 2002. J Calif Dent Assoc 2003; 31: 257–269.
Gao XL, Hsu CY, Xu Y, Hwarng HB, Loh T, Koh D . Building caries risk assessment models for children. J Dent Res 2010; 89: 637–643.
Celik EU, Gokay N, Ates M . Efficiency of caries risk assessment in young adults using Cariogram. Eur J Dent 2012; 6: 270–279.
Hänsel Petersson G, Fure S, Bratthall D . Evaluation of a computer-based caries risk assessment program in an elderly group of individuals. Acta Odontol Scand 2003; 61: 164–171.
Petersson GH, Twetman S . Caries risk assessment in young adults: a 3 year validation of the Cariogram model. BMC Oral Health 2015; 15: 17.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Maria Cagetti, Department of Biomedical, Surgical and Dental Sciences, University of Milan, Via Beldiletto 1, 20142 Milan, Italy. E-mail: maria.cagetti@unimi.it
Cagetti MG, Bontà G, Cocco F, Lingstrom P, Strohmenger L, Campus G. Are standardized caries risk assessment models effective in assessing actual caries status and future caries increment? A systematic review. BMC Oral Health 2018; 18: 123. doi: 10.1186/s12903-018-0585-4. PubMed PMID: 30012136; PubMed Central PMCID: PMC6048716.
Rights and permissions
About this article

Cite this article
Leal, S. Are standardised caries risk assessment models effective?. Evid Based Dent 19, 102–103 (2018). https://doi.org/10.1038/sj.ebd.6401338
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401338
This article is cited by
-
Might one simple question indicate a child's caries risk and guide preventive advice?
British Dental Journal (2019)
