
Abstract
Data sources
The resources searched included: Medline, PubMed, Embase, CINAHL, CAB Abstracts, the Cochrane Library and Google Scholar. The PRISMA guidelines for reporting systematic reviews were followed. Study selection was limited to the English language. Hand searching for additional references was performed. An intensive search was conducted for published articles describing the use of hilotherapy following oral and maxillofacial surgery.
Study selection
Inclusion criteria involved patients using hilotherapy after oral and maxillofacial surgery. Non-human studies were excluded. All articles were evaluated for study design, perioperative data, ethical suitability, follow-up data and surgical data reporting.
Data extraction and synthesis
Two authors independently judged articles for suitability for the review. A kappa statistic test was used to calculate and to measure concordance in the author's final decisions to include studies. The agreement was 83% and considered moderate. Following data extraction a meta-analysis was conducted. Heterogeneity was calculated due to the variability among the studies (different number of surgical procedures, patient age, duration of the device application, different methods of postoperative pain measurement and analgesics protocol). Standard mean differences (SMD) with 95% confidence interval (CI) were calculated for the continuous measurements. The studies were assessed and rated using the Oxford Centre for Evidence-Based Medicine Levels of Evidence criteria (all studies were rated as 2b). Publication bias was assessed.
Results
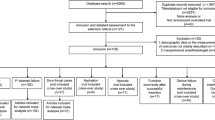
The initial search identified 552 results. Twelve papers were included in the review, and five with a total of 206 patients were used for the meta-analysis. The studies analysed were prospective comparative studies of patients undergoing oral maxillofacial surgery. Hilotherapy reduced pain (ten point visual analogue scale) at 48 hrs (P <0.010) and 72 hrs (P<0.050) as well as postoperative facial oedema (P <0.010) compared to ice-cooling treatment. Trismus and facial neurological scores were also improved (P<0.08). Patients preferred hilotherapy to other cooling methods (P< 0.010).
Conclusions
Hilotherapy appears to be effective in reducing postoperative facial pain, oedema and trismus and in improving patient-reported outcomes.
Similar content being viewed by others


Commentary
The systematic review published in the International Journal of Oral Maxillofacial Surgery had the purpose of evaluating the use of hilotherapy compared to conventional facial cooling techniques such as cool compress or ice packs.
Postoperative ice packs (cryotherapy) to relieve pain and swelling after different surgical strategies have been used in medicine for many years. The rationale of the cooling technique is that the ice applied in the area reduces the blood circulation, creates vasoconstriction and reduces metabolism.1
What is known is that prolonged application of cold to the area may produce unwanted side effects such as iatrogenic cold injury and patient discomfort.
However, the effectiveness of ice pack use in oral surgery seems controversial due to the claim that the technique requires an optimal delivery method, an appropriate interval for application and total duration of treatment to attain the outcome desired for swelling and pain reduction.2
This new therapy uses a machine that delivers water at the right temperature via tubes in an adaptable facemask that can be applied to the area and deliver a controlled constant temperature, thus reducing the risk associated with the conventional cryotherapy. The cooling devices use ‘chilled water’ instead of ice to decrease the temperature of the area to which is applied.
The review included only studies that used a motorised unit known as Heliotherm.3 The website has information available about the product, the benefits of its use, the research supporting the use of the system (most of the studies are included in this review) and recommendations on how to use it for professionals and patients. The products are available for purchase for providers and clinics as well for patients for home use. The devices can be rented or purchased.
The review reported and analysed five randomised clinical trials with an unclear risk of bias. Some of the methodological limitations of the studies were described, such as blinding of the clinicians, blinding of the outcome assessors and reporting of power calculation (an important step and prerequisite in the methodology of randomised clinical trials to detect statistically significant results and with that detect a statistical difference among the groups). The meta-analysis performed shows a statistically significant result favouring the hilotherapy technique, especially for pain and swelling. The surgical procedures undertaken in each study included orthognathic surgeries, osteosynthesis for treatment of mandibular fracture, treatment for zygomatic bone fracture and third molar extraction with osteotomy.
In medicine, especially in orthopedic medicine, other similar products are available for the same purpose of continuous controlled cooling therapy. The evidence in general is still debatable.4 In spite of this the overall claim is that the therapy is generally safe and not associated with any serious adverse events (such as can be present with pharmacological therapies such as corticosteroids and anti-inflammatory drugs).
Another systematic review using the same articles concluded that hilotherapy was associated with significant reduction in facial pain on postoperative day two and oedema on days two and three.5
A newly published randomised clinical trial which was not included in the review concluded that the system is effective for controlling postoperative edema and pain in patients undergoing surgery for displaced unifocal fracture of the mandible.6
Despite some limitations of the review, the evidence supports the use of hilotherapy to reduce postoperative pain and swelling in patients undergoing more complicated orofacial surgeries. The price and availability of the machine is still something for consideration.
References
Sortino F, Cicciù M . Strategies used to inhibit postoperative swelling following removal of impacted lower third molar. Dent Res J 2011; 8:162–171. doi:10.4103/1735-3327.86031.
Greenstein G . Therapeutic efficacy of cold therapy after intraoral surgical procedures: a literature review. J Periodontol 2007; 78:790–800.
http://www.hilotherapy.com/en/. [Accessed 19 August 2016]
Adie S, Kwan A, Naylor JM, Harris IA, Mittal R . Cryotherapy following total knee replacement. Cochrane Database Syst Rev 2012; 9: Art. No.: CD007911. DOI: 10.1002/14651858.CD007911.pub2.
Glass GE, Waterhouse N, Shakib K . Hilotherapy for the management of perioperative pain and swelling in facial surgery: a systematic review and meta-analysis. Br J Oral Maxillofac Surg 2016; pii: S0266-4356(16)30174-7. doi:10.1016/j.bjoms.2016.07.003. [Epub ahead of print]
Barca I, Colangeli W, Cristofaro MG, et al. Effects of cold therapy in the treatment of mandibular angle fractures: hilotherm system vs ice bag. Ann Ital Chir 2016; 87: pii: S0003469X16025227.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Anthony Bates, Department of Cancer Studies, University of Leicester, Leicester UK. E-mail: anthony.simon.bates@gmail.com
Bates AS, Knepil GJ. Systematic review and meta-analysis of the efficacy of hilotherapy following oral and maxillofacial surgery. Int J Oral Maxillofac Surg 2016; 45: 110–117.
Rights and permissions
About this article

Cite this article
Veitz-Keenan, A. Continuous cooling mask devices reduce patient discomfort and postoperative pain and swelling in patients undergoing orofacial surgery. Evid Based Dent 17, 121–122 (2016). https://doi.org/10.1038/sj.ebd.6401208
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401208
