
Abstract
Data sources
PubMed, Scopus, Medline and Cochrane Oral Health Group's Trials Register, CENTRAL. Limited to English language.
Study selection
Randomised control trials comparing preoperative steroids (in any formulation, dose or route) with placebo or no treatment in patients of any age, having extraction of one or more impacted third molars (under local or general anaesthesia or with intravenous sedation).
Data extraction and synthesis
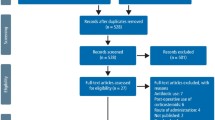
Two authors reviewed titles and abstracts of all articles to select those that met the inclusion criteria. The studies were classified by active principles, doses and treatment administration route. No meta-analysis was conducted and a tabular descriptive summary was presented.
Results
There were 28 studies (one meta-analysis and 27 randomised control trials) included in the descriptive account and from which conclusions were drawn.
Conclusions
The use of corticosteroids in third molar extractions reduces the degree of trismus and inflammation. Parenteral administration seems to be more effective than oral administration as does taking the corticosteroids before rather than after surgery. Further comparative studies using different corticosteroids, doses and administration routes are needed to establish the most effective regime for reducing pain, trismus and inflammation after extraction of third molars.
Similar content being viewed by others

Commentary
This systematic review started out appropriately. However, after completing an extensive and comprehensive search of the literature, the review changed from a ‘systematic’ review to a ‘narrative review’. Because of the heterogeneity of the study designs, outcome measures, and routes of drug administration, it was correct not to do a meta-analysis of the data. However, instead of examining all 28 studies for consistent effects of corticosteroids on pain, facial swelling and trismus, the investigators selected a small number of studies from the 28 reports to support their conclusions.
For example, the investigators chose only two studies to ascertain the impact of the proximity of the administration of the corticosteroid to the site of the third molar extraction. Mico-Llorens et al1 administered 40 mg of methylprednisolone into the gluteus muscle of one group of patients and Vega-Bustamante et al2 administered the same dose of methylprednisolone into the masseter muscle of another group of patients in a separate clinical trial. The p-values in the study evaluating administration of methylprednisolone in the masseter are much smaller than in the study evaluating administration in the gluteus muscle. However, the magnitude of the differences in pain, facial swelling, and trismus were similar in both studies. The differences in mouth opening between control groups and treatment groups were less than 5 mm. The goal of each of the studies was to establish the efficacy of methylprednisolone and neither study compared the efficacy of administration into the masseter muscle with administration into the gluteus muscle.
A second example of selecting two unrelated clinical trials to support their conclusions involved evaluating the timing of drug administration. Two unrelated clinical trials from the same institution were compared.3, One study evaluated the efficacy of intramuscular betamethasone4 and the other study evaluated the efficacy of administering betamethasone 3 hours following removal of the teeth.3 Both studies showed that betamethasone decreased pain, trismus, and pain. However, neither study was designed to compare the timing of drug administration.
The conclusions that parenteral rather than oral administration and preoperative rather than postoperative administration of corticosteroids give superior outcomes are not supported by the analysis of the outcomes of the 28 studies identified for detailed review. The well controlled clinical trials showed that corticosteroids statistically decrease pain, swelling and trismus. However, the outcomes of the 28 studies especially concerning pain relief are variable and it is not clear that the magnitude of the decrease in these surrogate measures has a favourable statistically or clinically significant effect on the patients' quality of life. Further studies examining patients' quality of life outcomes as well as route, dose, and timing of drug administration are needed to establish the efficacy of corticosteroids.
References
Mico-Llorens N, Satorres-Nieto M, Gargallo-Albiol J, Arnabat-Dominguez J, Berini-Aytes L, Gay-Escoda C . Efficacy of methylprednisolone in controlling complications after impacted lower third molar surgical extraction. Eur J Clin Pharmacol 2006; 62: 693–698.
Vegas-Bustamante E, Mico-Llorens J, Gargallo-Albiol J, Satorres-Nieto M, Berini-Aytes L, Gay-Escoda C . Efficacy of methylprednisolone injected into the masseter muscle following the surgical extraction of impacted lower third molars. Int J Oral Maxillofac Surg 2008; 37: 260–263.
Skjelbred P, Lakken P . Reduction of pain and swelling by a corticosteroid injected 3 hours after surgery. Eur J Clin Pharmacol 1982; 23: 141–146.
Skjelbred P, Lakken P . Post-operative pain and inflammatory reaction reduced by injection of a corticosteroid: A controlled trial in bilateral oral surgery. Eur J Clin Pharmacol 1982; 21: 391–396.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Francisco Javier Herrera-Briones, Oral Surgery and Implantology, University of Granada, C/José Palanca 22, local, 29003 Málaga, Spain. E-mail: fjherrerabriones@hotmail.com
Herrera-Briones FJ, Prados Sánchez E, Reyes Botella C, Vallecillo Capilla M. Update on the use of corticosteroids in third molar surgery: systematic review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol 2013; 116: e342-51. doi: 10.1016/j.oooo.2012.02.027. Epub 2012 Aug 17. PubMed PMID: 22902498.
Rights and permissions
About this article
Cite this article
Beirne, O. Corticosteroids decrease pain, swelling and trismus. Evid Based Dent 14, 111 (2013). https://doi.org/10.1038/sj.ebd.6400968
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400968
This article is cited by
-
Clinical evaluation of two dexamethasone regimens in the extractions of impacted third molars—a randomized clinical trial
Oral and Maxillofacial Surgery (2018)
-
Do Corticosteroids Still Have a Role in the Management of Third Molar Surgery?
Advances in Therapy (2016)
