
Abstract
Design
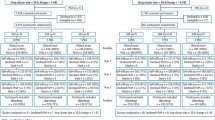
A patient-randomised controlled trial (RCT) and a cluster RCT of the same intervention were conducted independently of each other.
Intervention
The evidence-based intervention (a powered toothbrush and behavioural advice on timing, method and duration of toothbrushing) was framed to target oral hygiene self-efficacy (Social Cognitive Theory) and action plans (Implementation Intention Theory) to influence oral hygiene behaviour and therefore clinical outcomes. The content and the delivery of the intervention were standardised as a series of steps-altogether taking approximately 5 min. The control groups received routine care, even if that included oral hygiene advice.
Outcome measure
The primary outcome measures were behavioural (timing, duration and method of toothbrushing) matching the advice given in the intervention. Secondary outcomes were cognitive measures of self-efficacy and planning, and clinical measures of plaque and gingival bleeding.
Results
The study included 87 dental practices and 778 patients (patient RCT, 37 dentists and 300 patients; cluster RCT, 50 dentists and 478 patients). Controlled for baseline differences, pooled results showed that trial participants who experienced the intervention had better behavioural (timing, duration, method), cognitive (confidence, planning), and clinical (plaque, gingival bleeding) outcomes. Clinical outcomes were only significantly better in the cluster RCT, however.
Conclusions
A simple, theory-based intervention delivered within the constraints of a primary care environment was more effective than routine care in influencing patients' oral hygiene cognitions, behaviour and health. As clinical outcomes were significantly better only in the cluster RCT, the impact of trial design on results needs to be further explored.
Similar content being viewed by others

Commentary
In the UK, the majority of the National Health Service resources devoted to dental treatment are expended in the primary care arena of general dental practice. Successive governments and dental academics have all pointed out that the two common oral health problems of dental caries and periodontal disease are amenable to control through preventive health advice.1, 2, 3 There appears to be a reluctance, however, by many general practitioners to focus on offering dental health education advice, and many training institutions place greater emphasis on surgical rather than preventive interventions. One of the problems is that the evidence base for preventive advice and dental health education in general is weak.4 In particular, the value of primary care dentists offering preventive advice has not been assessed in a scientifically appropriate manner.
It has been difficult to undertake RCT in general dental practice because there are economic issues, in that research takes clinical time and has the potential to reduce a practitioner's income. Paying nonsalaried dentists to undertake research adds dramatically to the research revenue required and it is difficult to persuade research funding agencies to meet such a cost.
Clarkson et al. are to be congratulated on utilising the skills and time of newly qualified general dental practitioners in their 1-year intern programme following graduation. These individuals are paid a salary, so undertaking research is not a financial disincentive and costs will not escalate. The research design is elegant and will encourage other researchers to undertake RCT in what many academics had classified as the 'too difficult box'. I would rate this important paper as a demonstration study of how to undertake randomised controls in general dental practice.
As to whether the results should inform policy is much more complicated. Most authorities examining health education programmes want longer term studies, monitoring interventions over time.5 This study is short term and cannot answer the problem of 'behaviour-change fade' and whether the programme has an impact over time. The reader is therefore advised to focus on the methodological issues rather than the results of the intervention, which will require a longer term evaluation to assess its merit in terms of improving oral health.
References
Spencer AJ . An evidence-based approach to the prevention of oral diseases. Med Princ Pract 2003; 12 (suppl. 1): S3–S11.
Wentraub J . Dental public health research in action: population and community based research. J Calif Dent Assoc 2005; 33: 548–552.
Toolkit for Producing Patient Information. London: Department of Health; 2003.
Watt RG . Emerging theories into the social determinants of health: implications for oral health promotion. Community Dent Oral Epidemiol 2002; 30: 241–247.
Nutbeam D . Evaluating health promotion — progress, problems and solutions. Health Promot Int 1998; 13: 27–44.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Dr D Bonetti, Dental Health Services Research Unit, University of Dundee, MacKenzie Building, Kirsty Semple Way, Dundee DD2 4BF, Scotland, UK. E-mail: d.bonetti@chs.dundee.ac.uk
Clarkson JE, Young L, Ramsay CR, Bonner BC, Bonetti D. How to influence patient oral hygiene behavior effectively. J Dent Res 2009; 88: 933–937
Rights and permissions
About this article
Cite this article
Blinkhorn, A. Influencing patients' oral hygiene behaviour. Evid Based Dent 11, 41 (2010). https://doi.org/10.1038/sj.ebd.6400716
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400716
