
Key Points
-
The incidence of tuberculosis is on the increase in the UK
-
Tuberculosis should be considered in the differential diagnosis of chronic joint disease
-
The clinical appearance of tuberculosis of the temporomandibular joint is similar to that of ordinary arthritis of this joint and is unlikely to be diagnosed
-
Granulomas are encountered in relatively few pathologic states, tuberculosis being the archetypal granulomatous disease
Abstract
Primary tuberculosis is symptomless in the great majority of individuals. The clinical appearance of tuberculosis (TB) of the temporomandibular joint is similar to that of ordinary arthritis of this joint and so, is unlikely to be diagnosed early in non-destructive disease, especially when there are no symptoms and signs of TB elsewhere in the body. The role of Mycobacterium tuberculosis and other opportunistic organisms should not be overlooked in complicated head and neck infections as this is an ever increasing problem today, especially due to the emergence of multi-drug resistant strains of tuberculosis in some urban areas.
Similar content being viewed by others
Main
One third of the world's population is affected by tuberculosis. The incidence of this disease in Western countries is increasing alarmingly every year. Primary infection is usually in the lungs with secondary infection spreading to other organs and tissues. Rare secondary oral manifestations are seen such as a single chronic ulcer usually on the dorsum of the tongue associated with pulmonary infection. Lesions can also appear on the gingiva, palate, lips, buccal mucosa, frenulum and in the jaw bones.
Primary infection may occur in other organs of the body including the bones and joints but it usually involves a major joint. Tuberculosis of the facial bones has been reported occasionally but tuberculosis of the temporomandibular joint has been reported only once in the English literature. Tuberculosis of the temporomandibular joint should be considered in the differential diagnosis in patients presenting with pain and stiffness of the temporomandibular joint.1
Case report
A 37-year-old Caucasian female was referred to the Oral & Maxillofacial Surgery Department of the Chesterfield and North Derbyshire Royal Hospital by her general dental practitioner with a complaint of pain and stiffness in the left temporomandibular joint. The pain also radiated to her forehead and temple region.
She first started to experience recurrent episodes of pain and clicking in her left temporomandibular joint 4 years previously and decided to seek help as the pain had increased and became worse during mastication. Apart from some episodes of asthma during winter, she was generally fit and well. She was a heavy smoker and user of alcohol for which she was on antabuse. The patient denied any history of fever, malaise or recent trauma. No physical symptoms of tiredness and weight loss was reported. She also gave no history of any recent or recurrent ear infections.
On examination, she had slight trismus. There was no pre-auricular swelling and no palpable mass. Her vital signs were normal and there was no lymphadenopathy. An initial diagnosis of stress related facial arthromyalgia with a tender and enlarged left masseter muscle associated with a poorly moving disc within the joint was made. Non steroidal anti-inflammatory drugs were given without much improvement. Anti-depressants were subsequently prescribed but these also did not provide any relief. As the occlusion of her teeth was deranged and she was occluding heavily on her posterior teeth, a bite raising appliance was provided.
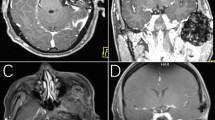
Radiographic examination of the chest and all other joints revealed no abnormality. An OPT of the mandible revealed a small round calcified lesion in the head of the left condyle. The blood tests were normal apart from a raised ESR, with a value of 37 mm/hr and an increased WBC count of 16×109/l. Due to several months of unsuccessful treatment and in view of the OPG findings, she was admitted for surgical exploration of her left temporomandibular joint. On exploration, it was seen that there was no obvious problem with the disc although there was some thickening of the meniscus. A high condylar shave was performed and this specimen was sent for routine histopathological examination. As the surgery did not relieve her pain, she was subjected to several sessions of ultrasound therapy to her joint. This also proved unsuccessful. The histology report showed that there were minor degenerative changes. The bone marrow showed unnatural foci of lymphoid infiltration, epithelioid macrophages and multi-nucleated giant cells associated with granulomas. Although there were no specific identifying features to demonstrate tuberculosis, it was suggested in the report that TB should not be excluded as a diagnosis and could be the cause of the patient's symptoms. As TB was not suspected at the time the condylar shave was performed, a suitable specimen was not available for Ziehl Nielsens staining. Sputum culture was negative, indicating no infection of TB in the lungs. Heaf test showed a strong reaction (Grade 3) and Mantoux test proved positive. The patient was referred to the consultant physician at the Chesterfield Royal Hospital for treatment with anti-tuberculosis medication. Her condition rapidly improved with reduction in the pain and clicking of her temporomandibular joint.
Discussion
Tuberculosis is an infectious granulomatous disease caused by the acid fast bacillus Mycobacterium tuberculosis and rarely Mycobacterium bovis. In most people, the primary infection heals, leaving some surviving tubercle bacilli. With a lowering of resistance, these are reactivated, producing local spread as well as haematogenous spread to all other organs of the body. About half the patients do not have pulmonary disease. Alcoholism and chronic debilitating disease may predispose reactivation. Hence tuberculosis should therefore be considered in the differential diagnosis of chronic joint diseases.2
Diagnosis is usually made by imaging, staining, biopsy and culture. Culture results for mycobacterium take as long as 4–8 weeks to be completed and cultures to determine the antibiotic sensitivity takes a further 3–4 weeks.2,3 Histologic evidence of granulomatous changes in bone or joint tissue in such patients provides an added insight into atypical infection, prompting the clinician to consider a mycobacterial process and begin appropriate investigations and treatment at an early stage.3,4
In this case, tuberculosis of the TMJ was suspected based on the histopathology, raised ESR & WBC count, a strong reaction to Heaf test and a positive Mantoux test. After a course of anti-tuberculous treatment the patient fully recovered and her ESR and WBC count had reduced to a normal level.

Calcified lesion, left condylar head
References
Hang WU, Qi Zheng Wang, Yan Jin . Tuberculosis of the temporomandibular joint. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998; 85: 243
Kumar P, Clark M . Infectious diseases, tropical medicine and sexually transmitted diseases In Kumar and Clark's Clinical Medicine. 4th ed pp 40 101–806 UK: WB Saunder's Company 1998
Ruggiero SL, Hilton E, Braun TW . Trismus and preauricular swelling in a 20 year old black women. J Oral Maxillofac Surg 1996; 54: 1234–1239
Resnick D, Niwayama G . Osteomyelitis, septic arthritis and soft tissue infection: organisms In Resnick's Diagnosis of Bone and Joint disorders. 4th edn pp 2478–2484 USA: WB Saunder's Company 1995
Scully C Handbook of oral disease; Diagnosis and management pp 2277–2286 UK: Martin Dunitz Publishers 1999
Neville BW, Damn DD, White DK Colour atlas of clinical oral pathology 2nd edn pp 118. USA: Lippincott, Williams and Wilkins 2000
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Soman, D., Davies, S. A suspected case of tuberculosis of the temporomandibular joint. Br Dent J 194, 23–24 (2003). https://doi.org/10.1038/sj.bdj.4802406
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4802406
This article is cited by
-
Rare Presentation of Tuberculous Osteomyelitis of Mandibular Condyle Mimicking as Parotid Tumor: A Case Report
Indian Journal of Otolaryngology and Head & Neck Surgery (2023)
-
Case series of extra pulmonary tuberculosis presenting as facial swelling
British Dental Journal (2015)
