
Key Points
In this part, we will discuss:
-
The integral aspects of the trial denture visit
-
The integral aspects of the insertion visit
-
What to do at the review appointments
Abstract
In this section, checklists are described to assist the practitioner in verifying the acceptability/ non-acceptability of complete dentures at trial insertion and insertion visits. The relative roles of clinician, technician and patient are discussed.
Similar content being viewed by others


Main
This chapter will be divided into three sections: one devoted to clinical aspects of the delivery of trial dentures, another to the delivery of the processed dentures, and the third section will deal with the review appointment.
Trial insertion of complete dentures
By definition, a trial denture is the arrangement of teeth in wax, for trial, prior to completion of the denture.1
By convention, this stage typically occupies one clinical visit, unless the trial denture has errors which are of clinical and/or technical origin! The temporal constraints of prosthodontic practice under NHS Regulations have often perceived this visit to be transient by nature. We would seek to redress this scenario and offer the suggestion that two trial visits may be considered as being both sensible and practical.
In the same way that the trial visit is often labelled a dress rehearsal, the analogy to our thespian counterparts is worth closer investigation. The role of a dress rehearsal for a theatre company is threefold. First of all, it enables actors to verify that they are all word-perfect. Secondly, it enables the wardrobe manager to confirm that the costumes and props are appropriate, both from a point of fit and also for verifying the temporal continuity of the costumes to the historical period reflected in the play. Finally, it enables the director to establish that all lighting changes and stage scenery are acceptable.
It is therefore perhaps appropriate to specify the role of the trial denture stage(s). Again, three aspects must be considered.
-
The functional and aesthetic acceptability of the dentures, according to the dentist (dentist's role).
-
The functional and aesthetic acceptability of the dentures, according to the patient (patient's role).
-
The competence of the technical delivery (technician's role).
These components are summarised in Table 1.
The dentist's role
On receipt of the articulated trial dentures, the clinician should perform more than a cursory examination of them prior to their placement in the mouth. The first stage is to ensure that the maxillary and mandibular trial dentures are well adapted to the respective master casts and that both bases are stable. The technician is responsible for ensuring the accuracy of fit of bases to casts while the ultimate responsibility for the accuracy of reproduction of the oral tissues rests with the clinician who recorded the definitive impression.
The next stage is to remove the mandibular trial denture from the articulator and to assess the relationship of the maxillary posterior teeth to the mandibular ridge. As a general guide to (lower) complete denture stability, the palatal cusps of the maxillary premolar and molar teeth should lie over the mandibular ridge (Fig. 1).

It is recommended that these cusps are placed over the lower ridge crest and thus occlude with the central fossae of the mandibular posterior teeth
With the mandibular denture still off the articulated mandibular casts, there is much merit in assessing the position of the posterior teeth by holding a straight-edged instrument on the ridge-section of the mandibular denture (Fig. 2); the central fossae of the lower posterior teeth should overlie the straight edge (this represents the zone occupied by the palatal cusps of the maxillary posterior teeth in retruded contact position [RCP]).

A wax knife is placed over the 'ridge space' of a trial denture to help relate the accurate placement of the mandibular posterior teeth
When both trial dentures have been removed from the articulator, the clinician should inspect the intermaxillary space to ensure no unplanned increase or decrease in dimension has occurred. If an intra-oral tracing method was used, the intermaxillary space may be verified by examining the central-bearing apparatus that should still be in the work tray. This provides a good guide to the distances between the upper and lower ridges. The clinician should also examine the casts to ensure that no laboratory-induced defects have been induced on the denture-bearing areas.
If both dentures are replaced on their respective casts, the clinician may then examine the occlusal relationships of both dentures, to establish that balanced occlusion is present and, if requested, that balanced articulation has been realised.
With the patient present, and following infection control procedures,2 the mandibular denture may be inserted in the patient's mouth. There are several reasons why there is merit in inserting the mandibular denture first.
-
If the maxillary denture is inserted first, the two buccinator muscles are, ideally, restored to their functional width and subsequent insertion of the mandibular denture may stretch the oral commissures; this may be a source of discomfort for many long-term edentulous patients.
-
If the maxillary denture is inserted first, insertion of the mandibular trial denture may dislodge the upper denture and this may alarm the patient unnecessarily.
-
The verification of a stable denture base and, further, of a peripheral seal in a lower denture is a source of relief and a confidence builder for patients who have a history of lower denture problems.
-
The patient may be shown how to use the tongue to control or 'weigh down' the mandibular denture. Careful instruction, at this stage may assist the patient to establish good circum-denture muscle balance which will enhance denture stability (Fig. 3).
Figure 3 
The lower trial denture is controlled by the circum-denture musculature to enhance stability and improve patient confidence

When the mandibular denture has been inserted, it should be checked for stability. If the base is stable on the master cast and unstable in the mouth, the possibility of a faulty definitive impression must be considered; if this is the case, a new definitive impression is indicated.
The extension of the mandibular denture base should also be assessed, bucco-labially and lingually. Over-extension should be removed and under-extension corrected; if the latter is a consequence of lack of extension into the master cast, the deficiency may be resolved by addition. If, however, the master cast is under-extended, problems of support and stability may arise (see Part 10), and a new definitive impression is indicated – the importance of educating the patient on how to control the lower denture has already been referred to. These factors should, of course, have been identified and corrected at the registration stage, but the thoroughness of double-checking at this stage should reduce post-insertion problems.
The maxillary trial denture is then assessed for stability and for over-/under-extension. The same guidelines for under-/over-extension of the lower denture base apply for the upper denture.
When both trial dentures are in the mouth, the following four aspects of the dentures may be assessed in turn.
-
Occlusal relations.
-
Occlusal planes.
-
Appearance of teeth and gums (gingival matrix).
-
Speech — should not be adversely affected by dentures.
Occlusal relations
As has been pointed out in Part 6, there are three intermaxillary relations to consider. These are the vertical, antero-posterior or sagittal and coronal intermaxillary relations.
The vertical relation is the occlusal vertical dimension (OVD) and the clinician should ensure that this has been reproduced faithfully from the registration sent to the technician. Figure 1, Part 6 illustrates how resting vertical dimension (RVD) and OVD may be measured to determine if the FWS is appropriate and the significance of this cannot be understated. As will be detailed later, vertical relations may also be assessed phonetically.
The sagittal or antero-posterior relation, at the established OVD should, in the complete denture patient, incorporate the retruded contact position (RCP) which is coincident with intercuspal position (ICP).3
The coronal relation relates the mandibular arch to the maxillary arch in a relationship generally observed from the frontal aspect.
The minimal requirement of all complete dentures is that all posterior teeth of both dentures (including canines) meet simultaneously and evenly in RCP. If balanced articulation is required, this should also be present in right and left working and protrusive movements. Verification of balanced articulation at the trial denture stage is recommended but should be done cautiously as the teeth are set in wax and may be dislodged if the patient is over-vigorous — even in the absence of occlusal interferences.
If the occlusal relation on the articulator is not matched in the mouth, especially RCP, the clinician should consider re-registering the occlusion. Only if there is a slight slide from RCP to ICP (ie less than 0.5 mm) can the clinician justify not re-registering the intermaxillary relationships.
If the occlusal relations are acceptable, the clinician should then confirm the acceptability of the occlusal planes.
Occlusal planes
In this category, four planes may be considered, namely the incisal plane, left and right posterior occlusal planes and the plane of the mandibular teeth.
Incisal plane: The inter-pupillary line is an acceptable guideline for this plane and the clinician, and the patient, should confirm its acceptability.
Right and left occlusal planes: Standard guidelines for these planes are that they should be parallel to the alar-tragus line and instruments such as Fox's occlusal plane guide may be used to confirm these planes (the right may not equal the left). Inappropriately formed planes may result in occlusal errors that may result in pathognomonic signs and symptoms (see Part 10).
Plane of the mandibular teeth: Ideally, the resting tongue should overlie the lingual aspects of the lower teeth and this may be demonstrated to good effect at the trial denture stage to augment (lower) denture stability vide supra.
Appearance of teeth and gums (gingival matrix)
This aspect of the trial denture visit(s) is of considerable importance to the patient and the acceptance of the dentures by the patient reflects the acceptability of tooth positioning, tooth selection and colour selection by the clinician plus the technical competence of the technician. Given the complexity of occlusal and aesthetic factors, we recommend that two trial visits, as a minimum, be allocated. This is especially valid when patients have a history of denture-related problems or where difficulties are anticipated.
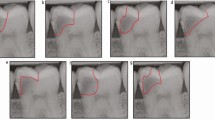
It is easy to be confused, if not discouraged, when there is a need to adjust twelve or fourteen teeth per denture. There is, therefore, merit in asking the technician to set-up only the six anterior teeth in each denture for an initial trial insertion. The appearance of only six teeth per denture may be seen, altered and agreed upon easily. In addition the vertical and antero-posterior intermaxillary relations of the trial dentures can be verified (Fig. 4).

This allows the clinician to determine that the occlusal parameters are acceptable and that the patient and the clinician may judge the appearance of the anterior set-up
When the form and arrangement of the upper and lower anterior teeth have been agreed upon, the second trial denture visit could be arranged, at which the posterior teeth are positioned and occlusal relations could be checked.
It must not be overlooked, however, that the technician's skills lie not only with tooth placement and angulation; in addition to these factors related to appearance is the contour of the waxwork equivalent to the gingival architecture. Here, the interdental papillae should be convex, the papillary lengths varied and the tissue heights formed appropriately to create a natural appearance (Fig. 4).
Speech
Speech is an important function that in general often receives scant attention from the dental profession. Most dentists are aware of the importance of clarity of sibilant sounds, in particular the test for the 'closest' speaking space, ie ask the patient to say 'Mississippi'.
Other phonetic tests which may be used relate to other consonant sounds, namely fricatives or labio-dental sounds (eg 'f' or 'v'). By asking a patient to say a sentence such as 'fish and vinegar' the clinician can determine if the fricative sounds are clear and this will help verify the appropriate placement of the upper central incisors antero-posteriorly.
When all of these tests have been performed by the clinician, we would recommend that the clinician leave the patient for a short time with their trial dentures, preferably in the company of a friend. Then allow the patient to converse and, in general, acclimatise to the proposed form of the replacement denture. Thereafter any additional modifications may be made to the dentures.
When the patient and the clinician are both satisfied with the trial dentures, the dentures may be sent for processing. Prior to returning the trial dentures to the laboratory for processing, thought should also be given to determining the shade of the denture base. This may be translucent in the palate, pink or veined or may be modified to conform to the gingivae of the patient.
The patient's role
The successful provision of replacement dentures owes much to patient co-operation and adaptation. Neither of these factors can be defined with clarity nor can they be easily quantified. For this reason, patient consent to form and appearance is paramount. As has been mentioned previously, we recommend that two trial denture visits be arranged, partly to facilitate any alterations to be performed at chairside by the clinician but also, of equal importance, to enable the patient to adjust and to consent to the form and appearance of the replacement dentures.
The technician's role
Although Part 9 will address technical considerations in the prescription of complete dentures, it is important to stress the importance of close, unambiguous communications between clinicians and technicians. The aims and objectives of a quality complete denture service should be common to both parties if the patient is to have any chance of adapting to replacement dentures. For these reasons, casts of acceptable quality require that impressions of acceptable quality are delivered. Similarly, technicians who spend a considerable time placing teeth in wax rims and then contouring the wax are understandably aggrieved when a reset is demanded because 'the bite is wrong'. The role of the technician is clearly that of a skilled team member who is wholly reliant on the clinician performing maximally.
Insertion of processed dentures
In essence, the clinical procedures of this stage mirror those of the trial denture stage, the exception being, hopefully, that the patient takes the replacement dentures home. Some technicians process dentures on the master casts and return the polished, processed dentures to the clinician in a plastic bag or some other receptacle. Many quality laboratories, however, practice a more ideal technique of having the dentures processed on duplicated master casts, so that the dentures are returned on casts and on the articulator.
The advantage of some articulator systems, of which the Denar system is a good example, is that the laboratory work may be sent on the mounting platforms and the technician and the dentist may retain their own articulators, yet both may be confident of the accuracy of the mounting.
The benefits of each surgery having a good articulator cannot be over-emphasised, as it enables the clinician to thoroughly examine the trial dentures and processed dentures comprehensively before they are inserted into the patient's mouth. Assuming that the above practices are followed, the suggested sequence of events required at the delivery stage are as follows:
-
1
With the processed dentures on the articulated casts, verify that the dentures are in balanced occlusion, and that the incisal guidance post is in contact with the incisal guidance platform. If the post is off the platform, an occlusal error/disturbance has occurred and this should be identified, using articulating paper, and the premature contacts should be ground to enable the post to contact the platform.
-
2
Check working, balancing and protrusive occlusions. Again the post should remain in contact with the platform during these movements. A different colour of articulating paper is recommended for each excursion. Prematurities should be removed only after they have been identified via the articulating paper. Polish the occlusal surfaces that have been ground.
-
3
Remove the dentures from the casts and ensure there are no sharp ridges or acrylic pearls on the 'impression' surface of the denture.
-
4
After appropriate infection control, place the lower denture in the mouth and assess that no over-extensions occur along the periphery of the denture. Gently press on the occlusal surfaces of the lower premolar teeth and ensure no support problems are evident at this stage.
-
5
Position the upper denture and ensure that no over-extensions are present along the periphery. Similarly, ensure no support problems exist at that stage by pressing gently on the occlusal surfaces of the premolar teeth.
-
6
Confirm the occlusal relationships are acceptable, as per stages 1 and 2.
-
7
Confirm appropriate freeway space exists.
-
8
The patient then be re-instructed how to use the tongue to control the lower denture.
-
9
We further recommend that, at this stage, the patient should be instructed to bite on the tip of a cotton wool roll (or a carrot) between the first premolar and canine teeth of the upper and lower dentures on a preferred biting side. Instruct the patient to keep a grasp of the roll (unless this is painful) and then pull the cotton wool roll away from the patient. Pain indicates either that a support problem exists or that the denture base is unstable. As the latter should have been excluded before, the support problem may be located via pressure-relief paste and the denture base relieved appropriately (see Part 10). An acceptable occlusal result is perceived to have been obtained if the cotton wool roll breaks. The object of this exercise is to instruct the patient how to bite (ie teach the patient to 'caninise' to incise).
-
10
Finally, let the patient inspect the dentures in a mirror and assess speech by asking the patient to repeat their address, etc.
Review procedures
The topic of dentist-organised reviews is prone to variation. It is our practice to arrange a review 4 days after insertion and a second review 1 week after that. Depending on factors as diverse as status of denture-bearing tissues, patient perceptions, etc, patients may request further 'views'. The procedures for dealing with denture problems will be dealt with in Part 10.
Epidemiological data would support the annual review of complete denture wearers to screen for any pathological changes in the oral tissues or associated denture-related problems.
Helpful Hints
-
1
Closely scrutinise the trial dentures on the articulated casts — do they equate to what you prescribed, and are the trial dentures well adapted to the casts?
-
2
Confirm that the position of the anterior and posterior teeth is acceptable.
-
3
Place the lower denture in the mouth before the upper when assessing both dentures as a dental unit.
-
4
The planned usage of two trial visits has much merit. The first concentrates on verifying OVD, RCP and appearance. The second confirms posterior planes, mandibular movements and a refinement of appearance.
References
Nairn R I, Shapiro M M J . Prosthetic Dentistry Glossary in Guidelines. In Prosthetic and Implant Dentistry, 1996. London: Quintessence Publishing Co., pp 29–97.
Control of Cross-Infection in Dentistry. BDA Advisory Services.
Guidelines to Standards in Prosthetic Dentistry — Complete and Partial Denture. In Ogden A (ed) Guidelines in Prosthetic and Implant Dentistry 1996. London: Quintessence Publishing Co. Ltd, pp 7–16.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
McCord, J., Grant, A. Trial dentures, insertion of processed dentures and review of complete dentures. Br Dent J 189, 4–8 (2000). https://doi.org/10.1038/sj.bdj.4800585
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4800585
