
Abstract
Invasion of prostatic adenocarcinoma into the seminal vesicles (SV) is generally accepted as an index of poor prognosis. The pre-operative identification of SV invasion is an important element in staging since it may alter subsequent treatment decisions. We studied the possibility of diagnosing SV invasion with two biopsies from the junction between the prostate and seminal vesicles. Also we studied the correlation of several prognostic factors with the risk of clinical stage T1,2,3 prostate cancer patients of having cancer growth into the seminal vesicles.
Consecutive patients referred for transrectal ultrasound (TRUS) and biopsy because of clinical suspicion of prostate cancer were examined. This staging procedure was evaluated in patients who underwent a pelvic lymphadenectomy and radical retropubic prostatectomy (RRP).
In 83 out of 138 patients prostate cancer was detected whereas 55 patients had benign disease. In 44% of prostate cancer patients a positive SV biopsy was found. The accuracy of the biopsies adjacent to the junction of the SV and the prostate was 91%. The best predictors for SV invasion were tumor grade of the biopsy sample (P<0.001), serum prostate-specific antigen (PSA) (P<0.0005), PSA density (P<0.0005) and clinical stage (P<0.0005). No significance was found in the relation to seminal vesicle involvement with free/total (f/t) PSA ratio (P=0.588) for the prostate cancer group (SV+ and SV−).
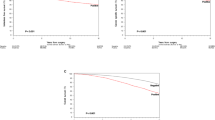
In a receiver operating characteristic curves analysis, PSA density was significantly more accurate for prediction of SV invasion than PSA or f/t PSA ratio. In five prostatectomized patients (and negative SV biopsy) no SV invasion was found in the final pathologic examination either.
SV biopsy at the junction of the SV and prostate is accurate for staging with high efficacy and low morbidity. To predict SV invasion in prostate cancer patients, PSA density was more accurate than PSA or f/t PSA ratio. The determination of the f/t PSA ratio in patients with low and intermediate PSA levels (eg <15 μg/L) is not useful to estimation of the risk of seminal vesicle involvement. The combination of serum PSA concentration, PSA density, tumor grade from the biopsy specimens ad clinical stage provides the best prediction of SV invasion. These parameters are identical to the conventional predictors of pathology after RRP. SV biopsies may provide additional information; if one or both basal biopsies are positive, a clinical T1,2 disease is altered to T3. Hence SV biopsy is useful for selection of patients who might obtain good results from RRP for prostate cancer.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others


Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Wymenga, L., Duisterwinkel, F., Groenier, K. et al. Ultrasound-guided seminal vesicle biopsies in prostate cancer. Prostate Cancer Prostatic Dis 3, 100–106 (2000). https://doi.org/10.1038/sj.pcan.4500407
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.pcan.4500407
