
Abstract
Study design: Single case report.
Objective: To report a case of urethral obstruction because of calculus in a subject with spinal cord injury (SCI).
Setting: Bangalore, India.
Case report: A 25-year-old man sustained complete SCI at C6 level following a road traffic accident. After 14 months, while on self-intermittent catheterization he noticed difficulty in introducing catheter and acute retention of urine. X-ray examination revealed a calculus in the penile urethra at the level of the glans penis.
Conclusion: Impaction of calculi in penile urethra, although rare, can manifest with acute painless urinary retention in patients with SCI.
Similar content being viewed by others


Introduction
Genitourinary complications are frequent among individuals with spinal cord injury (SCI).1 Incidence of urinary calculi in SCI varies from 2.3 to 9.5% depending on duration of injury.2 Residual urine, urinary tract infection (UTI) and chronic indwelling catheter are important predisposing factors for calculi formation. In the genitourinary tract, the urethra is the least common location for calculi. Overall, the incidence of urethral calculi among urolithiasis is only 1%.3 Urethral calculi result in pain, dysuria, haematuria and urinary retention. However, sensory deficits in SCI may modify these clinical manifestations. This communication reports a subject with tetraplegia who had difficulty in negotiating the catheter during intermittent self-catheterization following impaction of a calculus in penile urethra.
Case report
A 25-year-old man with tetraplegia following a road traffic accident underwent operative reduction and fixation of spine. He was admitted for rehabilitation 14 months after the injury. He had persistent loss of all sensory and motor function (ASIA-A)4 below C6 level with retention of urine. He had an indwelling urethral catheter for 1 year. His urine culture showed significant bacteriuria with Proteus mirabilis and Escheria coli. Both organisms were sensitive to amikacin. The urinary tract infection was treated and urine microscopy and culture done after 7 days of amikacin were normal. His cystometrogram with simultaneous sphincter EMG showed detrusor hyperreflexia with nonrelaxing sphincters. He was started on clean intermittent self-catheterization (CISC) and oxybutinin 5 mg three times a day. Ultrasound examination of the kidney and bladder were not done at this point. We did not attempt to manipulate urinary pH or start antibiotics as prophylaxis against UTI.
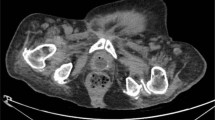
After 2 months, he presented with inability to pass his catheter and painless retention of urine. He did not have dysuria, haematuria or suprapubic pain. On palpation, an oval solid mass was detected at the level of the glans penis. An impacted urethral calculus was suspected. X-ray of the genital region revealed an oval calculus of 2 cm × 3 cm in size in fossa navicularis of the penile urethra (Figure 1). Ultrasound examination of kidneys, ureters and bladder was normal. Urinary microscopy showed pus cells and culture revealed significant bacteriuria because of P. mirabilis, sensitive to amikacin. The calculus was crushed transurethrally and removed. The UTI was treated with amikacin. He was able to perform CISC after the procedure.

X-ray showing ovoid calculus impacted in the fossa naviculasis of penile urethra
Discussion
Urinary calculi is often a late complication of SCI. Its incidence increases with duration after injury.2 Although calculi have also been reported in patients performing clean intermittent catheterization,5 the incidence was significantly reduced.6 As many as 98% of SCI patients with calculi had evidence of UTI, particularly with urea splitting organisms like Proteus.5 Our subject also had UTI because of P. mirabilis. Prompt treatment of UTI, especially those involving Proteus, may help to reduce urolothiasis among subjects with SCI. Manipulation of urinary pH and prophylaxis with antibiotics are other measures that will help to reduce UTI and stone formation in this population. Early cystoscopy to rule out urolithiasis may be considered in patients with SCI and recurrent UTI.
Urethral calculi are rare in Western countries but are common in developing countries.3 These calculi may become lodged at various levels in the urethra such as prostatic part, perineal part, fossa navicularis and external meatus. In our subject, the site of impaction was the fossa navicularis. Urethral calculi are frequently secondary to expelled vesical calculi. Primary urethral calculi are associated with urethral stricture or diverticulum.3 In this subject, ultrasound examination did not show calculi at any other part of the genitourinary tract and there was no obstruction of urethra after removal of the calculus. Thus, the exact site of origin of calculus in this patient is not certain.
Expulsion of urinary calculi through the urethra results in severe pain and only small calculi are expelled spontaneously. SCI patients may have loss of sensation, patulous Urethra and destrusor hyperreflexia enabling even large calculi to be expelled spontaneously.7 Our patient did not have any pain and his only symptoms were difficulty in negotiating his catheter and painless retention of urine. Symptomatic calculi that fail to expel spontaneously require management by methods such as flush back treatment and retrograde manipulation, ultrasonic fragmentation and extra corporeal shock wave lithotripsy or by surgical methods.8 Our patient was managed nonoperatively by intraurethral crushing and removal of calculus.
Conclusion
While urolithisasis is frequent among subjects with SCI, urethral calculi are rare. Our subject presented with difficulty in negotiating his urethral catheter during CISC and acute painless retention of urine because of impaction of calculus in penile urethra. Associated neurological deficits like absence of pain alters clinical features of urethral calculi in SCI. A high index of suspicion and periodic monitoring of genitourinary tract by imaging are necessary for early detection and prompt treatment to prevent complications.
References
Frankel HL et al. Long term survival in spinal cord injury: a fifty-year investigation. Spinal Cord 1998; 36: 266–274.
McKinkley WO, Jackson AB, Cardenas DD, Devivo MJ . Long term medical complications after traumatic spinal injury. Arch Phys Med Rehabil 1999; 80: 1402–1410.
Hemal AK, Sharma SK . Male urethral calculi. Urol Int 1991; 46: 334–337.
Ditunno Jr JF, Young W, Donovan WH, Creasey G . The International Standards Booklet for Neurological and Functional Classification of spinal cord injury. Paraplegia 1994; 32: 70–80.
Vaidyanathan S et al. Recurrent bilateral renal calculi in a tetraplegic patient. Spinal Cord 1998; 36: 454–462.
Perrouin-Verbe et al. Clean intermittent catheterization: long term evaluation of urethral and genital tolerance. Paraplegia 1995; 33: 619–624.
Anand J, Sivaraman Nair KP, Taly AB, Murali T . Spontaneous expulsion of large vesicle calculi in a woman with paraparesis. Spinal Cord 1999; 37: 737–738.
El-Sherif AF, El-Hafi R . Proposed new method for non-operative treatment of urethral stones. J Urol 1991; 146: 1546–1547.
Acknowledgements
We thank Ms Manjula Sharman for secretarial assistance and photography section for reproduction of the X-ray.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Syam, U., Taly, A., Sivaraman Nair, K. et al. Penile urethral obstruction in a subject with spinal cord injury. Spinal Cord 41, 367–368 (2003). https://doi.org/10.1038/sj.sc.3101448
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101448
