
Abstract
Researchers and clinicians refer to outcomes of genomic testing that extend beyond clinical utility as ‘personal utility’. No systematic delineation of personal utility exists, making it challenging to appreciate its scope. Identifying empirical elements of personal utility reported in the literature offers an inventory that can be subsequently ranked for its relative value by those who have undergone genomic testing. A systematic review was conducted of the peer-reviewed literature reporting non-health-related outcomes of genomic testing from 1 January 2003 to 5 August 2016. Inclusion criteria specified English language, date of publication, and presence of empirical evidence. Identified outcomes were iteratively coded into unique domains. The search returned 551 abstracts from which 31 studies met the inclusion criteria. Study populations and type of genomic testing varied. Coding resulted in 15 distinct elements of personal utility, organized into three domains related to personal outcomes: affective, cognitive, and behavioral; and one domain related to social outcomes. The domains of personal utility may inform pre-test counseling by helping patients anticipate potential value of test results beyond clinical utility. Identified elements may also inform investigations into the prevalence and importance of personal utility to future test users.
Similar content being viewed by others


Introduction
As genomic testing has become rapidly integrated into research and clinical care, the need to determine its overall utility to patients is imperative. Evaluative measures for introducing new tests or procedures into practice are primarily clinical, assessing end points and characteristics related to health and medical management such as decreased morbidity and mortality, pursuit of follow-up screening recommendations, and health-related quality of life.1 Yet individuals undergoing genomic testing report interest in receiving results for reasons that extend beyond these health parameters.2, 3, 4, 5 These reasons are often described in the literature as ‘personal utility’. Personal utility is the broad category of outcomes that includes subjective, non-health-related uses of genome sequencing such as increasing feelings of control, enhancing self-knowledge, feeling altruistic, and planning for the future.4, 6, 7, 8, 9, 10
Personal utility is not a novel concept in genome sequencing. Components of personal utility such as enhancing perceptions of personal control have long accompanied genetic testing,11 but until recently were overshadowed by pronounced clinical utility. Evaluation of genomic tests traditionally focused on three characteristics: analytical validity (the ability of the test to identify a given genotype), clinical validity (the reliability of a predicted phenotype based on the identified genotype), and clinical utility (the usefulness of that information to improve medical outcomes). Personal benefits of genomic testing have been discussed in early literature, and their empiric evaluation accelerated with the expansion of clinical genetic testing.2, 3, 5, 6, 12, 13, 14, 15, 16 Elements of personal utility are indirectly related to health outcomes and of overall importance to individuals undergoing testing; perceived as having an effect on their overall well-being.
Psychological well-being outcomes have inconsistently been classified in the literature as clinical utility17 or as outcomes separate from health status related.18 Distinct from personal utility (as described in the preceding paragraphs), measures of psychological well-being have long been assessed alongside clinical outcomes in genetic testing assessment.19 However, they do not encompass the complete spectrum of outcomes experienced by test users. For the purpose of our study we were interested in assessing an emerging concept of personal utility that predominantly consists of outcomes not health related.
Medicine is undergoing a shift toward more ‘personalized healthcare’ that integrates personalized medicine and individual preferences.20 The aim of personalized healthcare is to engage individuals in attaining and maintaining physical health and psychological well-being. To practice personalized healthcare, clinicians consider individuals’ personal values and preferences in conjunction with their clinical needs. When genomic testing is offered, an array of potential consequences from receiving results – clinical and non-clinical – should be deliberated in making informed decisions about testing and in establishing practice guidelines. A more complete understanding of perceived personal utility can inform both endeavors.
Theoretical and practical discussions of personal utility appear in the literature accompanied by studies that assess certain elements of personal utility as outcomes. Absent from this literature is a clear and consistent delineation of what constitutes personal utility and which non-medical benefits of genomic testing are most valued by those undergoing testing. Delineation of the elements of personal utility is useful to understanding the full scope of outcomes of genomic testing that lie in the context of personal utility. Characterizing the concept is a key step to amassing evidence for the role of personal utility in the overall utility of genomic testing.
We conducted a systematic review to synthesize elements of personal utility that have been reported in the empirical literature, focusing on the concept as defined by participants or patients, spanning a spectrum of genetic conditions and genomic tests. Delineating personal utility is a first step to assessing its role in decisions to undergo genomic testing.
Materials and methods
Search methods
A preplanned, comprehensive electronic literature search was conducted for all English language articles using PubMed, Scopus, Web of Science, and EMBASE from January 2003 to August 2016. Key terms included ‘genetic testing,’ ‘genome testing,’ ‘genomic testing,’ ‘genetic sequencing,’ ‘genomic sequencing,’ ‘exome sequencing,’ and synonyms combined with ‘personal utility,’ ‘patient utility,’ ‘personal meaning,’ ‘personal value,’ ‘personal outcomes,’ ‘non-clinical benefits,’ ‘non-clinical harms,’ ‘non-medical benefits,’ ‘non-medical harms,’ and synonyms. An example search strategy for PubMed is: ('genetic testing'[majr] OR 'genetic testing'[tiab] OR 'genetics testing'[tiab] OR 'genome testing'[tiab] OR 'genomic testing'[tiab] OR 'genomics testing'[tiab] OR 'genetic sequencing'[tiab] OR 'genetics sequencing'[tiab] OR 'genome sequencing'[tiab] OR 'genomic sequencing'[tiab] OR 'genomics sequencing'[tiab] OR 'exome sequencing'[tiab] OR 'exomic sequencing'[tiab] OR 'sequence analysis, dna'[majr] OR 'genetic profiling'[tiab] OR 'genome profiling'[tiab] OR 'genomic profiling'[tiab] OR 'genomics profiling'[tiab] OR 'direct to consumer testing'[tiab] OR 'direct to consumer genetic'[tiab] OR 'direct to consumer genetics'[tiab] OR 'direct to consumer genome'[tiab] OR 'direct to consumer genomic'[tiab] OR 'direct to consumer genomics'[tiab] OR 'personal genetic'[tiab] OR 'personal genetics'[tiab] OR 'personal genome'[tiab] OR 'personal genomic'[tiab] OR 'personal genomics'[tiab] OR 'individual genetic'[tiab] OR 'individual genetics'[tiab] OR 'individual genome'[tiab] OR 'individual genomic'[tiab] OR 'individual genomics'[tiab] OR 'genetic susceptibility testing'[tiab] OR 'genomic risk profiling'[tiab] OR 'genome based testing'[tiab]) AND ('personal utility'[tiab] OR 'patient utility'[tiab] OR 'individual utility'[tiab] OR 'participant utility'[tiab] OR 'consumer utility'[tiab] OR 'public utility'[tiab] OR 'health utility'[tiab] OR 'health-related utility'[tiab] OR 'clinical utility'[ti] OR 'medical utility'[ti] OR 'personal meaning'[tiab] OR 'patient meaning'[tiab] OR 'individual meaning'[tiab] OR 'participant meaning'[tiab] OR 'consumer meaning'[tiab] OR 'public meaning'[tiab] OR 'clinical meaning'[ti] OR 'medical meaning'[ti] OR 'personal value'[tiab] OR 'patient value'[tiab] OR 'individual value'[tiab] OR 'participant value'[tiab] OR 'consumer value'[tiab] OR 'public value'[tiab] OR 'clinical value'[ti] OR 'medical value'[ti] OR 'personal benefit'[tiab] OR 'personal benefits'[tiab] OR 'personal harm'[tiab] OR 'personal harms'[tiab] OR 'personal outcome'[tiab] OR 'personal outcomes'[tiab] OR 'non-clinical benefit'[tiab] OR 'non-clinical benefits'[tiab] OR 'nonclinical benefit'[tiab] OR 'nonclinical benefits'[tiab] OR 'non-medical benefit'[tiab] OR 'non-medical benefits'[tiab] OR 'nonmedical benefit'[tiab] OR 'nonmedical benefits'[tiab]). The first author supplemented this search by hand-searching bibliographies and publications using key words.
Study criteria
Study definitions
In this review, ‘personal’ was defined as non-health related or non-medical, and ‘utility’ was defined as subjective use, meaning, or value. Existing frameworks for evaluation of utility consist largely of economic or medical outcomes, missing many outcomes that are experienced by test users.6, 7, 9 As such, this review does not limit ‘utility’ as it is defined in existing frameworks but rather extends it to outcomes providing meaning and practical use to individuals beyond health status. This definition parallels that of most studies and is more narrow than the broad definition of personal utility invoked by the Institute of Medicine: ‘the meaning and worth a genomic test brings to an individual from that individual's perspective’.21 Our search extended ‘outcomes’ broadly beyond clinical utility to include both benefits and harms that may result from genomic testing. ‘Genomic testing’ included the full spectrum of testing from direct-to-consumer and single-gene testing to whole-exome and whole-genome sequencing.
Inclusion criteria
Studies were selected for inclusion if they (1) were written in English language; (2) were published between 1 January 2003 and 5 August 2016, and (3) contained empirical evidence for personal utility. We chose 2003 because it marks the conclusion of the Human Genome Project and a time of rapid increase in genomic test use. No studies referencing personal utility were found prior to that date. There were no limitations imposed on study design, genomic test type, study population, method of data collection or country of publication.
Exclusion criteria
Studies were excluded if they (1) did not meet inclusion criteria, (2) were opinion or workgroup papers, or (3) were reported in non-peer-review publications (gray literature).
Study selection method
Two authors performed the study selection using the following approach: (1) removing clearly irrelevant titles; (2) reviewing remaining abstracts and rejecting those that did not meet the inclusion criteria; (3) reading full articles of potentially relevant studies, and (4) selecting those that strictly met the inclusion criteria.
Quality
A quality appraisal tool was used based on Paul et al's apparisal tool22 appraisal tool and QualSyst,23 with the addition of two parameters: diversity of sample and participant having direct experience with genetic testing. Along with these two additional parameters, a total of 12 parameters were assessed including adequate description of study question, design, context, and recruitment; description of participants; appropriateness of data collection, analysis and conclusions; connection to theoretical framework and use of verification procedures. Studies were given a score from 0 to 2 where 0=no, 1=partial, and 2=yes. Qualitative studies and the qualitative portion of mixed-method studies were assessed using the same quality parameters. Parameter scores were summed for each study resulting in a final quality score out of 24. Authors JNK and ET independently evaluated the studies and disagreements were reconciled by discussion. Tabulated quality parameters and scores can be found in additional Supplementary File A1.
Data extraction and synthesis
Data were extracted on individual study characteristics (eg, genomic test type, study population, country of origin) and non-health-related outcomes. Outcomes categorized as psychological well-being (anxiety, depressive symptoms, disease-related worries, and distress) were considered elements of clinical utility as they contribute to health-related quality of life, and excluded from extraction.17
The focus of this literature review was to synthesize elements of personal utility as defined by participants or patients. As such, the primary analysis only included studies where concepts of personal utility arose directly from participants (generally with qualitative methodologies). Studies in which participants were asked to endorse concepts of personal utility posed to them by investigators (generally with quantitative methodologies) were analyzed separately.
Using a constant comparative method,24 a preliminary coding template for all reported non-health-related outcomes of genomic testing was developed. Final codes were selected by collapsing closely related reported outcomes. Authors JNK and ET independently coded the studies. Further review of the final element codes resulted in identification of four thematic domains.
Results
Study selection and characteristics
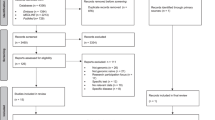
The systematic literature search yielded 551 abstracts after the removal of duplicates. All abstracts were read carefully and 64 articles were identified, which met the inclusion criteria. Thirty-seven were excluded based on lack of empirical results, and/or lack of outcomes that could be considered personal utility. Thirty-one met the inclusion/exclusion criteria and were included in this review (Figure 1).12, 14, 15, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52 Of these 31, 16 were qualitative in design, 11 used mixed methods, and 4 were quantitative in design. The majority (23/31) of the studies were conducted in the USA; other countries of origin included Canada (2), Netherlands (3), Australia (1), UK (1), and Switzerland (1). The types of genomic testing included: single-gene or gene panels (n=13, 42%), whole-exome/whole-genome sequencing (n=11, 35%), SNP-based or chromosomal microarray (n=4, 13%), and nonspecific genetic testing (n=3, 10%). Studies spanned the research, clinical, and consumer contexts. Table 1 summarizes study characteristics.

Systematic literature search flow.
The 31 studies included a total of 6461 participants ranging from 3 to 89 participants per qualitative study, from 40 to 755 per mixed-methods study, and from 202 to 2223 per quantitative study. Participants included affected individuals, unaffected individuals, and family members; individuals who have both had and not had genomic testing were included. The majority of studies involved patients (7/31), and/or family members (13/31) followed by the public (8/31), genome research participants (6/31), and health professionals such as physicians and scientists (4/31) with some involving a combination of different populations. Primary outcomes were similarly broad across studies, encompassing perceptions of and attitudes toward genomic testing; motivations for genomic testing; intentions to receive or use results; the impact of results; and personal experiences after receiving results. Elements of personal utility included in this review were reported as both primary and secondary study outcomes.
Elements of personal utility
Of the 31 studies, 27 included methodologies where concepts of utility arose directly from participants. Using these 27 studies, outcomes of personal utility were inductively coded. Initial coding of the studies resulted in 26 preliminary codes representing the elements of personal utility extracted from the data. These codes were revised and regrouped, resulting in 15 final elements of personal utility (Table 2). A range of 3–12 studies supported identified elements, averaging eight each. After final coding, a thematic analysis of the elements was conducted and elements were grouped into four distinct domains. Three of the domains were specific to personal outcomes: affective, cognitive, and behavioral. One domain encompassed social or societal level outcomes, with implications beyond the individual.
Personal outcomes
Affective
Affective outcomes refer to an individual’s emotional state and have the potential to change how one feels. This domain is comprised of four elements of personal utility: (1) to enhance (emotion-focused) coping, which includes coping with health risks, to feel more in control of oneself and of the situation, and for peace of mind; (2) mental preparation, for oneself, one’s family, to visualize future health and conversely as a false sense of security; (3) feelings of responsibility including both relief of responsibility or increased sense of responsibility; and (4) improved spiritual well-being such as a sense of purpose and appreciating the present. Of the elements identified as affective outcomes, the element most common among the 27 studies was ‘to enhance coping’; identified in 11 (41%) of the studies.
Cognitive
Cognitive outcomes refer to the gain of key information about genomic testing: (1) value of the information, that is, value of the information itself; (2) improved knowledge of condition such as its inheritance, etiology, and natural history; (3) self-knowledge, both of one’s own health as well as that of one’s family, and change in identity as a result of the genomic information; and (4) curiosity for what might be found and what it may mean. Eleven studies (41%) listed value of the information as an element of personal utility, the most in this domain, and included various participant populations and genomic test contexts.
Behavioral
Behavioral outcomes represent the practical uses of genomic information. These uses include: (1) ability for future planning such as long-term care, finances, career, getting affairs in order, and schooling; (2) reproductive autonomy, which involves the ability to plan for affected children, to refrain from having children, to adopt, or to undergo prenatal or pre-implantation genetic diagnosis of a familial condition; (3) communication with relatives, both increased and decreased, as a result of genetic information or genetic status (ie, positive or negative). Ability for future planning was supported by 12 studies (44%), the most in this domain; reproductive autonomy and communication with relatives are supported by 8 (30%) and 6 (22%) studies, respectively.
Social outcomes
Social outcomes involve changes in social support or status on individual, familial, and societal levels. The four elements in this domain are: (1) research altruism, largely for the benefit of research but also for family or society; (2) concern about stigma and concern about discrimination by insurance companies, employers, schools, in social environments, and by the government or police; (3) concern about confidentiality of information and privacy; (4) and change in social support from family, friends, and social resources. Research altruism and concern about discrimination and stigma were the two leading elements in this domain, each supported by 12 (44%) and 10 (37%) studies, respectively.
Endorsement studies
Four studies were identified in which investigators posed elements of personal utility to study participants to assess endorsement. No additional elements were represented to those identified through the data synthesis. The elements posed included: to enhance coping, self-knowledge, curiosity, ability for future planning, reproductive autonomy, research altruism, and concern about discrimination and stigma. A summary of study outcomes is given in additional Supplementary File A2.
Discussion
This systematic review identified 15 distinct elements of personal utility spanning four non-overlapping domains. Each element was cited by three or more independent studies, indicating that all are consistent non-health-related outcomes of genomic testing.
In this analysis, elements were primarily organized into domains according to how they affect the individual (personal outcomes) as the primary stakeholder in personal utility. Yet, we also identified elements that may affect families, communities, and the society at large (social outcomes). Genomic test results may have personal utility at the family level because the information is often relevant to relatives. Personal utility can also affect future family through reproductive planning. As such, the impact of personal utility may be inter-generational and long lasting. Personal utility also influences social constructs through individuals’ social groups and through its impact on the values of society at large. It can alter social relationships and spur concerns about discrimination, stigma, and racism. Studying personal utility by level of impact evinces its reach beyond the lives of individuals to the larger population and broadens understanding of ‘personal’ utility of genomic testing.
The prevalence of personal utility as an outcome of genomic testing was demonstrated in this literature review of 31 studies in which it was assessed. The studies represent a variety of genomic testing contexts that vary by test type, setting, and study population. Further, the elements show no significant skewing by test type or study population, although the relatively small groups make it unlikely that such a difference would be revealed. Our findings suggest that elements of personal utility are spread across genomic test type and are relevant to individuals undergoing genomic testing generally.
Another finding of this review is that alongside personal utility, individuals are experiencing and discussing harms of genomic testing. We found the majority of harms that individuals are experiencing may be classified as ‘social outcomes’. For example, test results have the potential to raise concerns about stigma, discrimination, and privacy. Although individuals may not derive ‘utility’ from these harms per se, the potential for these harms to arise as an outcome play an important role and, depending on perceptions of the potential benefit, sway decisions such as when or whether to undergo testing.
The elements reported in this review were derived using a general definition of personal utility to create a foundational evidence-based characterization of the concept. There have been theoretical and conceptual commentaries around limiting or categorizing the types of outcomes that are defined by ‘personal utility’. For example, Bunnik et al53 argue that genomic test results have personal utility only if they have meaning, purpose, and ‘can reasonably be used for decisions, actions, or self-understanding which are personal in nature.’ Bale and Mitchell54 take a more limited view of personal utility arguing that a test has non-clinical utility only if its results can be used for decisions or actions such as future planning, reproductive planning, or obtaining social resources. In both these views, genomic test results must provide valid information that is cognitively or behaviorally useful.
In our primary synthesis, we chose to include only studies of participants and patients, allowing the concept of personal utility to emerge from the data with minimal prompting by investigators. However, we did identify four studies that used quantitative methods designed by investigators that provide further evidence of the importance of personal utility to those undergoing genomic testing.49, 50, 51, 52 For example, Lupo et al.52 surveyed 202 participants in a genome sequencing study and found that a subset (23%) of participants (classified as ‘enthusiasts’) agreed their study results would influence their reproductive decisions and end of life planning.
Currently available measures of outcomes of clinical genetics services capture some aspects of personal utility identified in this literature review.55, 56, 57 The Psychological Adaptation Scale, for example, measures four domains of adaptation, which capture elements of personal utility such as ‘to enhance coping,’ ‘improved spiritual well-being,’ and ‘change in social support’.55 The Genetic Counseling Outcomes Scale and Psychosocial Aspects of Hereditary Cancer questionnaires capture additional elements including: ‘mental preparation;’ ‘feelings of responsibility;’ ‘knowledge of condition;’ ‘self-knowledge;’ ‘ability for future planning;’ ‘reproductive autonomy;’ ‘communication with relatives;’ and ‘concern about discrimination and stigma’.55, 58, 59 However, available measures do not capture identified outcomes of personal utility such as ‘curiosity’, ‘value of information’, and ‘concerns about privacy’. The majority were validated for use with specific genetic diseases or testing contexts. Some of these outcomes appear as items in patient empowerment and health-related quality-of-life scales.60 As these items have not been assembled into one assessment, psychometric investigation would be needed to create a valid and reliable scale of personal utility, alongside differentiation of the construct from concepts like adaptation.
Limitations
Strengths of the literature in this review include the representation of elements of personal utility from general, research, and disease-specific populations, and various test types. This ensures a range of findings and a comprehensive review. However, these data should be interpreted in light of certain limitations. First, although broad search terms were used to capture a comprehensive return of literature, it is possible that relevant data were missed. In particular, due to the subjective nature of defining personal utility, components of the concept may not have been captured, both in our review and through the identified research, a challenge in defining elements of a poorly defined concept. Data also may have been missed due to our exclusion of non-English language papers and may have been biased by the inclusion of papers identified through key author and reference searches. The variable quality of the reporting in the included studies may result in reporting bias. An additional limitation of the systematic literature review involves the inclusion of studies in which participants had no personal experience with genomic testing, possibly jeopardizing the validity of the derived elements. Similarly, we did not discriminate between hypothetical and actual outcomes. As such, the elements identified, including potential harms of genomic testing, may not eventuate in practice.
Implications for research and practice
Findings from this systematic review warrant attention, as they are directly relevant to both researchers and health professionals including genetic counselors. First, an understanding of the elements that comprise personal utility informs shared decision-making between genetic counselors or clinicians and their clients. Genetic counselors often elicit client values and preferences surrounding genomic testing. Having an evidence-based delineation of elements of personal utility will greatly benefit counselors’ knowledge about outcomes that may be most meaningful to clients on both a clinical and personal level. Using knowledge of personal utility, counselors can help clients evaluate the potential harms and benefits of genomic testing, and choose a path most in line with their values and needs.
Personal utility can also help guide the return of individual findings in research studies. Increasing amounts of genetic data necessitate consideration of which results to return to individuals. Previous studies show that research participants and the general public want nearly all genomic information returned to them, regardless of its clinical significance.14, 61 Personal utility provides another lens to help individuals discern which kind of results may have use to them, and thus, which kind of results they would like returned. By both enhancing shared decision-making and informing return of results, personal utility can be an important tool for clinicians and researchers to improve patient-centered care.
This review provides a comprehensive, foundational understanding of the elements that comprise personal utility in genomic testing. Still, there is room for future research to strengthen our evidence of domains and elements of personal utility and their role in decision-making or adaptation to results. Further research of personal utility in diverse testing experiences will shed further light on the generalizability of our findings. Longitudinal studies of personal utility are key, as the construct is dynamic and likely to evolve over time. It is also important to better understand how personal utility varies among diverse populations and cultures. A further critical step to amassing evidence about the prevalence and importance of evidence for elements of personal utility is in designing and assessing a scale for the concept.
Conclusion
By identifying the elements that comprise personal utility in genomic testing, we can now construct a more complete picture of the ways in which genomic testing impacts individuals. This includes individuals’ expectations of genomic testing as well as the ways they react to and use their results. Such an understanding is important to practicing and improving personalized healthcare because it brings into focus the needs of the individual that go beyond medical care. Using our synthesis of personal utility, it may be possible to include the elements identified when evaluating genomic tests for clinical implementation.
References
Grosse SD, Khoury MJ : What is the clinical utility of genetic testing? Genet Med 2006; 8: 448–450.
Low CA, Bower JE, Kwan L, Seldon J : Benefit finding in response to BRCA1/2 testing. Ann Behav Med 2008; 35: 61–69.
Neumann PJ, Hammitt JK, Mueller C et al: Public attitudes about genetic testing for Alzheimer's disease. Health Aff 2001; 20: 252–264.
Ravitsky V, Wilfond BS : Disclosing individual genetic results to research participants. Am J Bioeth 2006; 6: 8–17.
Wasson K, Sanders TN, Hogan NS, Cherny S, Helzlsouer KJ : Primary care patients' views and decisions about, experience of and reactions to direct-to-consumer genetic testing: a longitudinal study. J Community Genet 2013; 4: 495–505.
Botkin JR, Teutsch SM, Kaye CI et al: Outcomes of interest in evidence-based evaluations of genetic tests. Genet Med 2010; 12: 228–235.
Bunnik EM, Schermer MH, Janssens AC : Personal genome testing: test characteristics to clarify the discourse on ethical, legal and societal issues. BMC Med Ethics 2011; 12: 11.
Finch AP, Lubinski J, Møller P et al: Impact of oophorectomy on cancer incidence and mortality in women with a BRCA1 or BRCA2 mutation. J Clin Oncol 2014; 32: 1547–1553.
Grosse SD, Wordsworth S, Payne K : Economic methods for valuing the outcomes of genetic testing: beyond cost-effectiveness analysis. Genet Med 2008; 10: 648–654.
Rogowski WH, Grosse SD, John J et al: Points to consider in assessing and appraising predictive genetic tests. J Community Genet 2010; 1: 185–194.
Berkenstadt M, Shiloh S, Barkai G, Katznelson MB-M, Goldman B : Perceived personal control (PPC): a new concept. Am J Med Genet 1999; 82: 53–59.
Bakos AD, Hutson SP, Loud JT, Peters JA, Giusti RM, Greene MH : BRCA mutation-negative women from hereditary breast and ovarian cancer families: a qualitative study of the BRCA-negative experience. Health Expect 2008; 11: 220–231.
Bernhardt BA, Zayac C, Pyeritz RE : Why is genetic screening for autosomal dominant disorders underused in families? The case of hereditary hemorrhagic telangiectasia. Genet Med 2011; 13: 812–820.
Bollinger JM, Scott J, Dvoskin R, Kaufman D : Public preferences regarding the return of individual genetic research results: findings from a qualitative focus group study. Genet Med 2012; 14: 451–457.
Shostak S, Zarhin D, Ottman R : What’s at stake? Genetic information from the perspective of people with epilepsy and their family members. Soc Sci Med 2011; 73: 645–654.
Burke W, Atkins D, Gwinn M et al: Genetic test evaluation: information needs of clinicians, policy makers, and the public. Am J Epidemiol 2002; 156: 311–318.
Veenstra DL, Roth JA, Garrison LP, Ramsey SD, Burke W : A formal risk-benefit framework for genomic tests: facilitating the appropriate translation of genomics into clinical practice. Genet Med 2010; 12: 686–693.
Haddow JE, Palomaki GE ACCE: a model process for evaluating data on emerging genetic tests; Human Genome Epidemiology: A Scientific Foundation for Using Genetic Information to Improve Health and Prevent Disease. USA: Oxford University Press: New York, NY, USA, 2004, pp 217–233..
Athens BA, Caldwell SL, Umstead KL, Connors PD, Brenna E, Biesecker BB : A systematic review of randomized controlled trials to assess outcomes of genetic counseling. Journal of Genetic Counseling 2017, [in press].
Cribb A, Owens J : Whatever suits you: unpicking personalization for the NHS. J Eval Clin Pract 2010; 16: 310–314.
Feero WG, Wicklund C, Veenstra DL : The economics of genomic medicine: insights from the IOM roundtable on translating genomic-based research for health. JAMA 2013; 309: 1235–1236.
Paul J, Metcalfe S, Stirling L, Wilson B, Hodgson J : Analyzing communication in genetic consultations—A systematic review. Patient Educ Couns 2015; 98: 15–33.
Kmet LM, Lee RC, Cook LS Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields. Edmonton: Alberta Heritage Foundation for Medical Research, 2004..
Dixon-Woods M, Agarwal S, Jones D, Young B, Sutton A : Synthesising qualitative and quantitative evidence: a review of possible methods. J Health Serv Res Policy 2005; 10: 45–53B.
Cornelis C, Tibben A, Dondorp W et al: Whole-exome sequencing in pediatrics: parents’ considerations toward return of unsolicited findings for their child. Eur J Hum Genet 2016; 24: 1681–1687.
Daack-Hirsch S, Driessnack M, Hanish A et al: 'Information is information': a public perspective on incidental findings in clinical and research genome-based testing. Clin Genet 2013; 84: 11–18.
Facio FM, Brooks S, Loewenstein J, Green S, Biesecker LG, Biesecker BB : Motivators for participation in a whole-genome sequencing study: implications for translational genomics research. Eur J Hum Genet 2011; 19: 1213–1217.
Facio F, Eidem H, Fisher T et al: Intentions to receive individual results from whole-genome sequencing among participants in the ClinSeq study. Eur J Hum Genet 2013; 21: 261–265.
Fox E, McCuaig J, Demsky R et al: The sooner the better: genetic testing following ovarian cancer diagnosis. Gynecol Oncol 2015; 137: 423–429.
Giordimaina AM, Sheldon JP, Petty EM : Anticipated motivation for genetic testing among smokers, nonsmokers, and former smokers: an exploratory qualitative study of decision making. Public Health Genomics 2014; 17: 228–239.
Goh AM, Chiu E, Yastrubetskaya O et al: Perception, experience, and response to genetic discrimination in Huntington's disease: the Australian results of The International RESPOND-HD study. Genet Test Mol Biomarkers 2013; 17: 115–121.
Gooding HC, Linnenbringer EL, Burack J, Roberts JS, Green RC, Biesecker BB : Genetic susceptibility testing for Alzheimer disease: motivation to obtain information and control as precursors to coping with increased risk. Patient Educ Couns 2006; 64: 259–267.
Hayeems RZ, Babul-Hirji R, Hoang N, Weksberg R, Shuman C : Parents' experience with pediatric microarray: transferrable lessons in the era of genomic counseling. J Genet Couns 2016; 25: 298–304.
Hoskins LM, Werner-Lin A : A multi-case report of the pathways to and through genetic testing and cancer risk management for BRCA mutation-positive women aged 18-25. J Genet Couns 2013; 22: 27–38.
Levenseller BL, Soucier DJ, Miller VA, Harris D, Conway L, Bernhardt BA : Stakeholders' opinions on the implementation of pediatric whole exome sequencing: implications for informed consent. J Genet Couns 2014; 23: 552–565.
Lewis KL, Hooker GW, Connors PD et al: Participant use and communication of findings from exome sequencing: a mixed-methods study. Genet Med 2016; 18: 577–583.
Meisel SF, Wardle J : 'Battling my biology': psychological effects of genetic testing for risk of weight gain. J Genet Couns 2014; 23: 179–186.
Reiff M, Giarelli E, Bernhardt BA et al: Parents' perceptions of the usefulness of chromosomal microarray analysis for children with autism spectrum disorders. J Autism Dev Disord 2015; 45: 3262–3275.
Steinberg AG, Kaimal G, Bain L, Krantz I, Li Y : Parental narratives on genetic testing for children with hearing loss: a qualitative inquiry. Am J Med Genet A 2007; 143: 1533–1545.
Van Der Zwaag AM, Weinreich SS, Bosma AR et al: Current and best practices of genetic testing for maturity onset diabetes of the young: views of professional experts. Public Health Genomics 2015; 18: 52–59.
Vayena E, Gourna E, Streuli J, Hafen E, Prainsack B : Experiences of early users of direct-to-consumer genomics in Switzerland: an exploratory study. Public Health Genomics 2012; 15: 352–362.
Williams JK, Erwin C, Juhl A, Mills J, Brossman B, Paulsen JS : Personal factors associated with reported benefits of Huntington disease family history or genetic testing. Genet Test Mol Biomarkers 2010; 14: 629–636.
Wright MF, Lewis KL, Fisher TC et al: Preferences for results delivery from exome sequencing/genome sequencing: genome results preferences. Genet Med 2014; 16: 442.
Yu JH, Crouch J, Jamal SM, Bamshad MJ, Tabor HK : Attitudes of non-African American focus group participants toward return of results from exome and whole genome sequencing. Am J Med Genet A 2014; 164a: 2153–2160.
Yu JH, Crouch J, Jamal SM, Tabor HK, Bamshad MJ : Attitudes of African Americans toward return of results from exome and whole genome sequencing. Am J Med Genet A 2013; 161a: 1064–1072.
Zarate OA, Brody JG, Brown P, Ramirez-Andreotta MD, Perovich L, Matz J : Balancing benefits and risks of immortal data: participants' views of open consent in the personal genome project. Hastings Cent Rep 2016; 46: 36–45.
Bernhardt BA, Zayac C, Pyeritz RE : Why is genetic screening for hereditary hemorrhagic telangiectasia underutilized in families? Hematol Rep 2011; 3: 37.
Birmingham WC, Agarwal N, Kohlmann W et al: Patient and provider attitudes toward genomic testing for prostate cancer susceptibility: a mixed method study. BMC Health Serv Res 2013; 13: 279.
Henneman L, Timmermans DR, Van Der Wal G : Public attitudes toward genetic testing: perceived benefits and objections. Genet Test 2006; 10: 139–145.
Neumann PJ, Cohen JT, Hammitt JK et al: Willingness-to-pay for predictive tests with no immediate treatment implications: a survey of US residents. Health Econ 2012; 21: 238–251.
Roberts SJ, LaRusse SA, Katzen H et al: Reasons for seeking genetic susceptibility testing among first‐degree relatives of people with Alzheimer disease. Alzheimer Dis Assoc Disord 2003; 17: 86–93.
Lupo PJ, Robinson JO, Diamond PM et al: Patients' perceived utility of whole-genome sequencing for their healthcare: findings from the MedSeq project. Per Med 2016; 13: 13–20.
Bunnik EM, Janssens AC, Schermer MH : Personal utility in genomic testing: is there such a thing? J Med Ethics 2015; 41: 322–326.
Bale SJ, Mitchell AG : Genetic testing in ectodermal dysplasia: availability, clinical utility, and the nuts and bolts of ordering a genetic test. Am J Med Genet A 2009; 149: 2052–2056.
Biesecker BB, Erby LH, Woolford S et al: Development and validation of the psychological adaptation scale (PAS): use in six studies of adaptation to a health condition or risk. Patient Educ Couns 2013; 93: 248–254.
Payne K, Nicholls S, McAllister M, MacLeod R, Donnai D, Davies LM : Outcome measurement in clinical genetics services: a systematic review of validated measures. Value Health 2008; 11: 497–508.
McAllister M, Dearing A : Patient reported outcomes and patient empowerment in clinical genetics services. Clin Genet 2015; 88: 114–121.
Eijzenga W, Bleiker EM, Hahn DE et al: Psychosocial aspects of hereditary cancer (PAHC) questionnaire: development and testing of a screening questionnaire for use in clinical cancer genetics. Psychooncology 2014; 23: 862–869.
McAllister M, Wood AM, Dunn G, Shiloh S, Todd C : The Genetic Counseling Outcome Scale: a new patient-reported outcome measure for clinical genetics services. Clin Genet 2011; 79: 413–424.
Barr PJ, Scholl I, Bravo P, Faber MJ, Elwyn G, McAllister M : Assessment of patient empowerment-a systematic review of measures. PLoS ONE 2015; 10: e0126553.
Turbitt E, Halliday J, Amor D, Metcalfe S : Preferences for results from genomic microarrays: comparing parents and health care providers. Clin Genet 2015; 87: 21–29.
Acknowledgements
We would like to thank Judith Welsh and Verma Walker, NIH Librarians for developing the database search strategies and performing the literature searches in support of this systematic review. The Intramural Research Program of the National Human Genome Research Institute, National Institutes of Health funded this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on European Journal of Human Genetics website
Supplementary information
Rights and permissions
About this article

Cite this article
Kohler, J., Turbitt, E. & Biesecker, B. Personal utility in genomic testing: a systematic literature review. Eur J Hum Genet 25, 662–668 (2017). https://doi.org/10.1038/ejhg.2017.10
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejhg.2017.10
This article is cited by
-
The value of genomic testing in severe childhood speech disorders
European Journal of Human Genetics (2024)
-
QALYs and rare diseases: exploring the responsiveness of SF-6D, EQ-5D-5L and AQoL-8D following genomic testing for childhood and adult-onset rare genetic conditions in Australia
Health and Quality of Life Outcomes (2023)
-
Genomic medicine in neonatal care: progress and challenges
European Journal of Human Genetics (2023)
-
Key drivers of family-level utility of pediatric genomic sequencing: a qualitative analysis to support preference research
European Journal of Human Genetics (2023)
-
“I am not a number!” Opinions and preferences of people with intellectual disability about genetic healthcare
European Journal of Human Genetics (2023)
