
Abstract
Study design:
Experimental study.
Objectives:
The objective of this study was to establish a non-invasive model to produce pressure ulcers of varying severity in animals with spinal cord injury (SCI).
Setting:
The study was conducted at the Johns Hopkins Hospital in Baltimore, Maryland, USA.
Methods:
A mid-thoracic (T7–T9) left hemisection was performed on Sprague-Dawley rats. At 7 days post SCI, rats received varying degrees of pressure on the left posterior thigh region. Laser Doppler Flowmetry was used to record blood flow. Animals were killed 12 days after SCI. A cardiac puncture was performed for blood chemistry, and full-thickness tissue was harvested for histology.
Results:
Doppler blood flow after SCI prior to pressure application was 237.808±16.175 PFUs at day 7. Following pressure application, there was a statistically significant decrease in blood flow in all pressure-applied groups in comparison with controls with a mean perfusion of 118.361±18.223 (P<0.001). White blood cell counts and creatine kinase for each group were statistically significant from the control group (P=0.0107 and P=0.0028, respectively).
Conclusions:
We have created a novel animal model of pressure ulcer formation in the setting of a SCI. Histological analysis revealed different stages of injury corresponding to the amount of pressure the animals were exposed to with decreased blood flow immediately after the insult along with a subsequent marked increase in blood flow the next day, conducive to an ischemia–reperfusion injury (IRI) and a possible inflammatory response following tissue injury. Following ischemia and hypoxia secondary to microcirculation impairment, free radicals generate lipid peroxidation, leading to ischemic tissue damage. Future studies should be aimed at measuring free radicals during this period of increased blood flow, following tissue ischemia.
Similar content being viewed by others

Introduction
The efficient prevention and treatment of pressure/decubitus ulcers (bed sores) remain a significant challenge in the care of individuals with spinal cord injury, and such lesions impart a substantial cost to society.1 The Agency for Healthcare Research and Quality states that pressure ulcers cost the US health-care system an estimated $9.1–$11.6 billion annually.2 Pressure ulcers not only necessitate significant medical expenses in the future but also irreversibly impair the quality of life of affected patients.3, 4 The most severe pressure ulcers cause substantial necrosis of subcutaneous fascia and muscle, with the potential to produce osteomyelitis.5, 6 Paraplegic patients are at a particularly high risk for the development of pressure ulcers due to immobility, compounded by the loss of sensation, in the extremities. Ninety-five percent of all pressure ulcers occur in the lower extremities, and the rate of surgical complications and recurrence is particularly high for individuals with a spinal cord injury (SCI). For patients with a SCI and pressure ulcer, 40% suffer from surgical complications and 79% have recurring ulcers.6, 7, 8, 9, 10, 11, 12 It has been reported that 6.6% of all hospital readmissions for individuals with SCI are due to pressure ulcers.13 The global incidence of SCI is estimated to be between 40 and 80 cases per million in the population.14 The National Spinal Cord Injury Association reports that as many as 450 000 people in the United States are living with a SCI with an estimated 11 000 new cases every year.15
Pressure ulcers are clinically and histologically classified into four categories with increasing severity corresponding to the extent of tissue loss, that is, Stage I–IV, according to the National Pressure Ulcer Advisory Board. Stage I is defined as a non-blanchable erythema at the skin surface. Stage II is defined as a shallow open ulcer with partial thickness loss of dermis. Stage III is full-thickness tissue loss. Stage IV is full-thickness tissue loss with exposed bone, tendon or muscle and often includes tunneling.16 Although visible damage and erythema at the level of the skin may be a concern in the earlier stages of pressure ulcer formation, pressure is highest between the bony prominence and the underlying soft tissue. Deep tissue damage is therefore far greater than the visible damage to the skin. As such, pressure ulcers have been often defined as having an ‘iceberg-like’ quality, with the skin being the tip of the iceberg.17 Histologically, it would be expected that deep tissue injury would be far greater even though the dermis is intact in early stage ulcers.
Although pressure ulcers can significantly alter patient health, effective treatment modalities for these ulcers are exceptionally scarce. Progress is impeded because there are currently no translational research models that accurately produce a range of pressure ulcers in spinal cord injury, as they would be observed clinically.18, 19, 20, 21 For models that do produce pressure ulcers in spinal cord injury, these ulcers are not followed over time for soft tissue breakdown.
For an animal model to successfully recapitulate a pressure ulcer, there must be an external and measurable sustained force at the surface of the skin that causes compression of the underlying muscle. It must also exist in an animal that is immobilized or significantly dependent, as occurs with a spinal cord injury. Prior models of pressure ulcer formation have several disadvantages that create difficulty in drawing substantial conclusions.
In this manuscript, we describe a model for pressure ulcer formation that involves hemi-sectioning the spinal cord of a rat to induce spinal cord injury, followed by a calibrated pressure to the affected limb to create reproducible ulcers of varying severity. Furthermore, we histologically and physiologically characterize our animal model in terms of the clinical phenotypes found in the human condition. This method of pressure ulcer formation has important features that make it clinically relevant.
Materials and methods
Animals
Twenty-five female adult Sprague-Dawley rats, aged 6-week old, were used for all experiments. Five animals were placed in each pressure ulcer (PU) group to establish the SCI/PU model. Rats were housed under a normal light cycle and temperature of 25 °C. All procedures were approved by the institution’s ACUC committee.
Spinal cord injury
All animals were shaved before surgical manipulation. A spinal cord hemisection was performed at a mid-thoracic level (T7–T9) under aseptic conditions to simulate spinal cord injury. Animals were anesthetized with a mixture of inhalational anesthesia comprising isoflurane 5% initially and 3.5% maintenance with 2% oxygen. A 3-cm midline incision was made on the back, and the paraspinal muscles were retracted to expose the thoracic laminae. A laminectomy was performed exposing the dura of the thoracic spinal cord (T7–T9), the dura was opened and the spinal cord exposed. The midline of the spinal cord was identified, and one half (the left side) of the spinal cord was transected completely using fine scissors and surgical forceps. Hemostasis was attained, the surgical areas were lavaged and the wounds were closed. Rats were treated with buprenorphine (0.05 mg kg−1 body weight, s.c.) post-operatively to minimize discomfort.
Pressure application
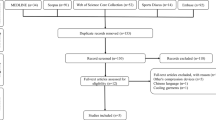
After the hind limb fur was shaved, pressure was applied externally, on the surface of the skin, 7 days after spinal cord injury. Twenty-five Sprague-Dawley rats were separated into five groups with five rats in each group (Figure 1). The first group did not receive any external pressure. Each subsequent group received enough pressure to produce a stage 1, 2, 3 or 4 pressure ulcer, based on the previously established pressure values18, 19, 20, 21, 22, 23, 24 (Table 1).

Pressure application model. (a) Medical illustration of rats placed on platform scales with a C-clamp used to apply load pressure. Pressure was calibrated using the weight of the scale and the surface area of the external clamp. (b) Medical illustration of pressure ulcer progression from edema after a few hours following compression. (c) Broken epithelium and skin breakdown. (d) Early infiltration of polymorphonuclear cells. (e) Inflammatory exudate after the pressure application. Printed with permission. ©JHU Neurosurgery - Ian Suk.
Pressure was applied with Husky 4-inch C-clamps (The Home Depot, Cranbury, NJ, USA) for a period of 8 h, at varying pressures, to the posterior thigh region of the left, paralyzed, hindlimb. Each animal was placed on a Horizon HPS-110 Digital Platform Postage Scale (Horizon Solutions, Rochester, NY, USA), which was tared and utilized to assess the quantity of load pressure. Pressure was calculated using the following formula:

The tissue exposed to pressure was assessed daily for the development of pressure ulcers. The presence or absence of skin breakdown was noted. Each animal was photographed, before killing, 12 days after spinal cord injury.
Laser Doppler flowmetry
A moorLDI (Moor Instruments, Wilmington, DE, USA) Laser Doppler machine was used to assess blood flow every day, following spinal cord injury. Blood flow for animals receiving pressure was assessed twice on the day of pressure application, once before pressure and once after pressure. Ischemia/reperfusion is expected in the development of pressure ulcers and will be represented in a value of perfusion units (PFUs).
Histology
All animals were killed on day 12, relative to spinal cord injury. Full-thickness tissue from the pressure zone (posterior thigh region) of each animal was harvested. Tissue from the same region of the opposite, neural intact, limb was harvested for each animal. Formalin-fixed, paraffin-embedded, tissue was stained with hematoxylin and eosin (H&E).
Blood chemistry
A cardiac stick was performed on each animal, following euthanasia. Several blood tests were performed to assess inflammatory response and tissue damage. Blood tests included a complete blood count with differential and creatine kinase.
Statistical analysis
Statistical analysis consisted of one-way analysis of variance followed by the Tukey Multiple comparison test using Prism (Graph Pad Software Inc., La Jolia, CA, USA). A P-value <0.05 was deemed statistically significant.
Results
Spinal cord-injured pressure ulcer model
All animals tolerated the spinal cord injury and pressure application well. All rats had paralysis of their left leg immediately post spinal cord hemi-section. Varying amounts of pressure were applied to each group under the conditions specified above 7 days after spinal cord hemi-section. Immediately following pressure application, there was a shallow depression corresponding to the size and location of the applicator (Figure 1). The paralyzed hind limb demonstrated the presence of edema after a few hours following compression. Animals demonstrated evidence of skin breakdown as early as 6 h after the pressure application in a graded response and were photographed 5 days after pressure application, at the time of euthanasia (day 12 of the study) (Figure 2). Control animals had no evidence of skin breakdown. Animals treated with 250 mm Hg pressure application demonstrated intact skin with non-blanchable redness over the applied location. Animals treated with 500 mm Hg pressure application showed partial thickness loss of the dermal layer, with reddish pink wound bed and superficial sloughing of the skin. Figure 2b demonstrates a stage 2 ulcer with an open/ruptured blister. At 750 mm Hg pressure application, treated animals demonstrated full-thickness tissue loss with exposure of the subcutaneous fat and muscle, with no bony or tendinous exposure, whereas animals treated with 1000 mm Hg pressure application had the same full-thickness tissue loss with exposed bone and/or tendons as well as muscle.

Representative images of pressure ulcers. (a) Rats receiving 250 mm Hg displayed characteristics of a stage 1 pressure ulcer, with non-blanchable redness and erythema. (b) Rats receiving 500 mm Hg displayed characteristics of a stage 2 pressure ulcer, with early signs of epithelial breakdown, a reddish pink wound bed and superficial sloughing of the skin. (c) Rats receiving 750 mm Hg displayed characteristics of a stage 3 pressure ulcer, with full-thickness tissue loss, exposure of the subcutaneous fat and muscle, and no bony or tendinous exposure. (d) Rats receiving 1000 mm Hg displayed characteristics of a stage 4 pressure ulcer, with full-thickness tissue loss extending deep into the muscle to exposed bone and tendons.
Histological analysis
Pressure-induced ulcer formation was assessed via hematoxylin and eosin staining of full-thickness cross-sectional slides taken from the pressure zone in the paralyzed hind limb 5 days after pressure application. Histological staining demonstrated an intact epithelium with early necrotic damage in the pressure zone of animals treated with 250 mm Hg as compared with control. Control animals demonstrated intact epithelium, viable layers of dermis and well-organized loosely packed connective tissue throughout (Figure 3a1). Animals treated with 250 mm Hg demonstrated necrosis to deeper layers of the dermis and muscle, although overlying epithelium was intact, consistent with the ‘iceberg effect’ (Figure 3b1). Animals treated with 500 mm Hg demonstrated early epithelial breakdown, eschar formation, densely packed connective tissue in the deeper layers of the dermis and bloating and distortion of dermal collagen fibers (Figure 3c1). Animals treated with 750 mm Hg were denoted by broken epithelium, necrotic damage, widespread densely packed connective tissue and muscle necrosis with an infiltration of inflammatory cells and polymorphonuclear leukocytes. The overall muscle architecture was still preserved in this group (Figure 3d1). The group of animals that underwent pressure application with 1000 mm Hg showed substantial necrotic damage to the muscle, inflammatory cell infiltration, a loss of cellular integrity, complete loss of the epithelial layer and hematoma formation in the dermal layer. Higher stage pressure ulcers were also at greater risk for inflammation and exudate6, 25, 26 (Figure 3e1).

Representative histology of pressure ulcers. Following euthanasia, full-thickness tissue was harvested on each limb of each animal. H&E staining was performed for all tissue sections. (a1, a2 and a3) × 10, × 40 and × 64 magnification, respectively, of a hemiparaplegic rat that did not receive pressure. (b1, b2 and b3) × 10, × 40 and × 64 magnification, respectively, of a hemiparaplegic rat that received 250 mm Hg pressure to the left posterior thigh region. These animals demonstrated necrosis to deeper layers of the dermis and muscle, although overlying epithelium was entirely intact, consistent with the ‘iceberg effect’. (c1, c2 and c3) × 10, × 40 and × 64 magnification, respectively, of a hemiparaplegic rat that received 500 mm Hg pressure to the left posterior thigh region. These animals demonstrated early epithelial breakdown, eschar formation, densely packed connective tissue in the deeper layers of the dermis and bloating and distortion of dermal collagen fibers. (d1, d2 and d3) × 10, × 40 and × 64 magnification, respectively, of a hemiparaplegic rat that received 750 mm Hg pressure to the left posterior thigh region. These animals demonstrated epithelial breakdown, necrotic damage, widespread densely packed connective tissue and muscle necrosis with an infiltration of inflammatory cells and polymorphonuclear leukocytes (PMNs). The overall muscle architecture was still preserved in this group. (e1, e2 and e3) × 10, × 40 and × 64 magnification, respectively, of a hemiparaplegic rat that received 1000 mm Hg pressure to the left posterior thigh region. These animals demonstrated substantial necrotic damage to the muscle, inflammatory cell infiltration, a loss of cellular integrity, complete loss of the epithelial layer and hematoma formation in the dermal layer. Black arrow: intact epithelium. Orange arrow: broken epithelium. Yellow arrow: eschar. Red arrow: loosely packed connective tissue. Green arrow: irregular densely packed connective tissue. Blue arrow: necrotic muscle. Purple arrow: hematoma.
Laser Doppler flowmetry/blood flow analysis
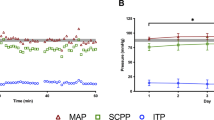
Pressure ulcers are hypothesized to occur secondary to induced ischemia followed by a reperfusion injury. To determine whether our model was consistent with this hypothesis, we utilized laser Doppler flowmetry to assess blood flow in the paralyzed and unaffected hind limb every 24 h following spinal cord injury. In animals receiving pressure, blood flow was assessed before pressure application and after pressure application. A region of interest of constant area was selected on the posterior thigh region of each animal (Figure 4a). The Doppler blood flow after spinal cord injury before pressure application was 238±16 PFUs at day 7. Immediately following pressure application, there was a statistically significant decrease in blood flow in all pressure applied groups in comparison with controls with a mean perfusion of 118±18 (P<0.001). The day after pressure application (day 8), there was a substantial increase in the perfusion of the pressure zone with a mean perfusion of 289±17 when compared with the perfusion immediately after pressure application (P<0.001). These results demonstrate that the pressure application induced a decrease in blood flow in the affected area followed by a significant increase in blood flow to the affected area, which is consistent with the hypothesized ischemia/reperfusion mechanism. This increased blood flow is expected to be due to reactive hyperemia followed by inflammatory vasodilation (Figure 4b).

Laser Doppler blood flow analysis. (a) Laser dopper flowmetry was performed every day, following spinal cord injury. Blood flow for animals receiving pressure was assessed twice on the day of pressure application, once before pressure and once after pressure. (b) The Doppler blood flow after spinal cord injury before pressure application was 237.808±16.175 PFUs at day 7. Immediately following pressure application, there was a statistically significant decrease in blood flow in all pressure applied groups in comparison with controls with a mean perfusion of 118.361±18.223 (P<0.001). The day after pressure application (day 8), there was a substantial increase in the perfusion of the pressure zone with a mean perfusion of 288.997±16.512 when compared with the perfusion immediately after pressure application (P<0.001).
Blood chemistry—cell count
Before killing on day 12, 5 days after pressure application, we performed a cardiac puncture to collect blood on each animal to determine whether pressure-applied animals demonstrated an increased inflammatory response and/or evidence of muscle breakdown. We analyzed the blood from each group for red blood cell counts, white blood cell counts, % of neutrophils, % of lymphocytes, % of monocytes and % of eosinophils, as well as creatine kinase (CK), blood urea nitrogen and creatinine. We found no statistically significant difference in red blood cell counts, % of neutrophils, % of monocytes and % of eosinophils between controls and pressure-applied animals; however, we did find a statistically significant difference between controls and all of the pressure-applied animals for white blood cell, and lymphocyte counts and creatine kinase (P<0.01; Figure 5). Furthermore, when we stratified groups based on the presence or absence of intact epithelium (stages 1 and 2 vs 3 and 4), we found that the white blood cell and lymphocyte counts for each group were statistically significant from those of the control group (P=0.0107 and P=0.005, respectively). Furthermore, the lymphocyte count increased from 2326±332 cells μl−1 in the control group to 4718±390 cells μl−1 in groups 1 and 2 to 5315±412 cells μl−1 in groups 3 and 4. When muscle breakdown was assessed via the CK level, we found that the CK levels in groups 1 and 2 versus groups 3 and 4 were significantly increased in comparison with controls (P=0.0028), and moreover groups 3 and 4 had significantly higher CK levels than groups 1 and 2 (P<0.01). The CK level increased from 480±35 U l−1 in the control group to 1286±274 U l−1 in groups 1 and 2 to 2855±480 U l−1 in groups 3 and 4. These results demonstrate that pressure application increases an animal’s inflammatory response as measured by white blood cell and lymphocyte counts, in addition to increasing the degree of muscle breakdown as the amount of pressure is increased.

Blood counts. A cardiac puncture was performed for each animal, following euthanasia. (a) White blood cell counts for each group were statistically significant from the control group (P=0.0107). (b) Lymphocyte counts for each group were statistically significant from the control group (P=0.005). Lymphocyte count increased from 2.326±0.3317 in the control group to 4.718±0.3902 in groups 1 and 2 to 5.315 ±0.4115 in groups 3 and 4. (c) CK levels in groups 1 and 2 vs groups 3 and 4 were significantly increased in comparison with controls (P=0.0028), and groups 3 and 4 had significantly higher CK levels than groups 1 and 2 (P<0.01). *P<0.001; **P<0.01.
Discussion
Even with the best clinical care, pressure ulcers are a substantial challenge to individuals with spinal cord injury and impart a significant cost to the US health-care system. Pressure ulcers are caused by sustained pressure at the surface of the skin, thereby resulting in soft tissue breakdown between the compressed skin and underlying bony prominence.2, 3, 4, 5, 6 Capillary closure and ischemia are present in the subdermal layers of such wounds with visible erythema of the skin, in its earliest stages.3, 12 Because the skin displays only minor signs of breakdown, pressure ulcers are often characterized as having an ‘iceberg-like’ quality, in that the extent of the damage occurs subdermally and is not visible on the surface, adding to the challenge of diagnosing and preventing these wounds.7, 8, 9, 10, 11, 27 The pressure ulcers seen clinically often result from a combination of direct pressure and shear forces causing friction.5, 16, 17
Currently used animal models have drawbacks that limit their usefulness. Models to evaluate these ulcers, including the surgical placement of an implant underneath the muscle and a pressure applicator screwed into the bone, or an implanted magnet and overlying magnet, alter the environment of soft tissue before the onset of pressure ulcer formation.22, 24, 25 Other less-invasive models include pinching the skin with magnetic plates but do not apply pressure to the underlying muscle.11 As such, wounds created from these models do not demonstrate true pressure ulcers.
Rat pressure ulcer models have been developed to increase our understanding of the risk factors, progression and efficacy of potential treatment modalities. In this study, we demonstrate a non-invasive method to produce pressure ulcers of varying severity in a rat spinal cord-injured model. Utilizing an external pressure model, we show that, with varying pressures, we can reproducibly generate different pressure ulcer severity with associated visual and histological characteristics. Furthermore, we show that the pressure-induced damage is associated with increased white blood cell and lymphocyte counts, as well as increases in creatine kinase. This model also demonstrates the ischemia/reperfusion mechanism of injury that is presumed to be a causative factor in pressure ulcer formation. Taken together, these results provide a novel preclinical model that can effectively and reproducibly mimic the clinical phenotypes seen in patients diagnosed with pressure ulcers following spinal cord injury.
Prior models of pressure ulcer formation have several advantages and disadvantages that create difficulty in drawing substantial conclusions. For an animal model to successfully recapitulate this injury, there must be an external and measurable sustained force and time following the onset of pressure for ischemic necrosis to take place.14 The model proposed by Lin et al.24 simulates the role of a bony prominence in pressure ulcer formation by implanting a metal pellet on the lateral surface of the rat’s tibial bone. The model proposed by Hyodo et al.22 fabricates a pressure applicator from a 6.5-mm diameter cancellous screw percutaneously implanted into the greater trochanter of a monoplegic pig. These models alter the environment of soft tissue before the onset of pressure ulcer formation. Surgical implantation, or any other breach in the skin barrier, releases inflammatory cytokines and compromises the integrity of soft tissue even before pressure application. As such, the most clinically relevant pressure ulcer model demands a solely external and non-invasive load—mimicking what would ensue clinically.
The model by Stadler et al.11 attempts to create a model without an invasive surgical component through the use of magnets. Although there is visible erythema and pressure at the level of the skin, this model only superficially encompasses pressure ulcers without the subdermal necrotic damage characteristic of the pathology. Early stage pressure ulcers are characterized by an ‘iceberg-effect’, in that the bulk of tissue damage occurs at the level of muscle with minimal damage to the overlying epithelium. Because this model fails to apply any load force to the muscle the wound formed is not a true pressure ulcer.17
The model by Bosboom et al.28 uses an external indentor but does not do so in the setting of spinal cord injury, nor are there varying stages of ulcers studied. This model also fails to follow the progression of ulcers by harvesting 24 h after pressure application. Models by Cui et al.,29 Gefen et al.30 and Jiang et al.1 harvest tissue following pressure application but do not do so in the setting of spinal cord injury. The model by Gostein et al.31 studied tissue breakdown from externally applied pressure in pigs over a period of 10 days but did not study stage III or IV ulcers. In addition, this was not performed in the setting of spinal cord injury. The model by Kokate et al.32 studied temperature on pressure ulcer progression over time but did not do so in spinal cord injury and only applied 100 mm Hg external pressure in each group studied. Models by Linder-Ganz et al.30, 33, 34, 35 successfully study deep tissue injury in externally applied pressure ulcer models with varying pressure but harvest tissue immediately following pressure and do not study these ulcers in the setting of spinal cord injury. The model by Salcido et al.36 externally applied pressure and measured blood flow by Laser Doppler but only applied 145 mm Hg and measured perfusion during pressure application. To capture the range of ulcers, varying pressures must be used. In addition, blood flow should be measured before pressure in order to determine a baseline and after pressure to determine reperfusion.
It is essential to determine a distinction between pressure ulcer models in the setting of spinal cord injury and those without spinal cord injury.37 In the setting of spinal cord injury, in addition to atrophy and decreased blood flow, MRI scans have shown significant anatomical differences in gluteal and high-risk areas of patients with spinal cord injury.38, 39, 40, 41, 42 Because of the significant necrosis that occurs from reactive oxygen species following ischemia it is also necessary that effective pressure ulcer models allow time following injury to accurately study the breadth of pressure ulcer formation.43 Our model overcomes these issues by applying external pressure without breaching the skin in a spinal cord-injured model, following progression over time, and studying varying stages of pressure ulcers. Furthermore, the ability to alter the amount of pressure the animal experiences ensures that a graded pressure ulcer response can be achieved. This allows for more precise assessment of the pathophysiologic mechanisms associated with a given pressure ulcer stage and the ability to reproducibly create the desired stage for further testing. Moreover, laser Doppler blood flow close to the infrared spectrum allows for an analysis of muscle blood flow and deep tissue perfusion.44, 45
Pressure ulcer progression relies on ischemia and reperfusion of tissue. Sustained pressure causes ischemia in the capillaries and microvasculature of the muscle tissue. Thus, subsequent reperfusion delivers free radicals, exacerbating damage done to the previously hypoxic tissue.3, 5, 6, 12 Through Laser Doppler Flowmetry we showed that our external pressure model results in increased blood reperfusion following pressure application and recapitulates the presumed mechanism of ischemia/reperfusion associated with pressure ulcer formation. We were able to show a statistically significant decrease in blood flow immediately following pressure application compared with blood flow assessment before the insult. Subsequent measurement of blood flow after 24 h, however, showed a marked increase in blood flow to the region. Taken together, these data further support current evidence about the role of ischemia/reperfusion in the development of pressure ulcers while emphasizing the robustness of our model in recapitulating clinically significant pressure ulcers.
Patients with SCI represent a unique population that is particularly susceptible to the development of pressure ulcers with increased morbidity and mortality associated with the occurrence of the ulcer, in addition to monetary cost to the health system. A number of models have been developed in animals to study pressure ulcer formation. Our model and data add to our continued understanding of the unique factors that contribute to how pressure ulcers are formed. The potential exists for the use of this model to study therapies for both patients who are at risk and those affected. Such therapies may focus on ways to strengthen the skin as well as means to decrease ischemia/reperfusion injury via a free radical scavenging system or methods to increase blood flow to areas susceptible to the development of ulcers. Further studies into free radical scavenging systems following pressure ulcer formation are required to address ischemia–reperfusion injury. These modalities will be relevant not only for patients with SCI but others at risk for the development of ulcers including the elderly, malnourished patients, patients with other neurovascular injuries (that is, diabetic patients) or chronically deconditioned patients among others.
Our model may have several limitations and disadvantages that could limit the ability to draw substantial conclusions. For instance, in our model, a clamp is applied to the hindlimb of animals and compressed against a scale. In human patients, their ulcer normally falls from a single-sided compression. Furthermore, animals are hemi-sectioned instead of a full spinal cord injury, which is more consistent with what is found in spinal cord-injured patients. This model does not study the reactive oxygen species associated with reperfusion injury, nor does it study shear forces in addition to direct pressure. These limitations may hinder the true assessment of pressure ulcer formation in animals; however, these limitations can be considered minor in comparison with the ability to induce a pressure ulcer through a non-invasive method.
Conclusions
We have created a novel animal model of pressure ulcer formation in the setting of a spinal cord injury. Histological analysis revealed different stages of injury corresponding to the clinical stages and related to the amount of pressure the animals were exposed to. Decreased blood flow immediately after the insult along with a subsequent marked reperfusion in blood flow the next day suggests reactive hyperemia a possible inflammatory response. Animals who sustained the insult also had increased levels of creatine kinase with elevated WBC and lymphocyte blood counts. In this way, this model serves as an accurate preclinical tool to study spinal cord injury-associated pressure ulcers for evaluation of the human condition.
Data archiving
There were no data to deposit.
References
Jiang LP, Tu Q, Wang Y, Zhang E . Ischemia-reperfusion injury-induced histological changes affecting early stage pressure ulcer development in a rat model. Ostomy Wound Manage 2011; 57: 55–60.
Agency for Healthcare Research and Quality Are we ready for this change? preventing pressure ulcers in hospitals: a toolkit for improving quality of care, 2011 (cited 2015). Avilable at http://www.ahrq.gov/professionals/systems/hospital/pressureulcertoolkit/index.html.
Khoo C . Pressure ulcer research: current and future perspective. Ann R Coll Surg Engl 2007; 89: 193.
Kosiak M, Kubicek WG, Olson M, Danz JN, Kottke FJ . Evaluation of pressure as a factor in the production of ischial ulcers. Arch Phys Med Rehabil 1958; 39: 623–629.
Bouten CV, Oomens CW, Baaijens FP, Bader DL . The etiology of pressure ulcers: skin deep or muscle bound? Arch Phys Med Rehabil 2003; 84: 616–619.
Byrne DW, Salzberg CA . Major risk factors for pressure ulcers in the spinal cord disabled: a literature review. Spinal Cord 1996; 34: 255–263.
Dinsdale SM . Decubitus ulcers: role of pressure and friction in causation. Arch Phys Med Rehabil 1974; 55: 147–152.
Goodman CM, Cohen V, Armenta A, Thornby J, Netscher DT . Evaluation of results and treatment variables for pressure ulcers in 48 veteran spinal cord-injured patients. Ann Plast Surg 1999; 42: 665–672.
Kosiak M . Etiology of decubitus ulcers. Arch Phys Med Rehabil 1961; 42: 19–29.
Lindan O . Etiology of decubitus ulcers: an experimental study. Arch Phys Med Rehabil 1961; 42: 774–783.
Stadler I, Zhang RY, Oskoui P, Whittaker MS, Lanzafame RJ . Development of a simple, noninvasive, clinically relevant model of pressure ulcers in the mouse. J Invest Surg 2004; 17: 221–227.
Vasconez LO, Schneider WJ, Jurkiewicz MJ . Pressure sores. Curr Probl Surg 1977; 14: 1–62.
ACC EBH Group. Pressure ulcers in spinal cord injured clients, 2009 (cited 2015). Available at http://www.acc.co.nz/PRD_EXT_CSMP/groups/external_communications/documents/reports_results/wpc090235.pdf.
Department of Economic and Social Affairs of the United Nations Secretariat. World Population Prospects: the 2012 revision, 2013 (cited 2015). Available at http://esa.un.org/unpd/wpp/Publications/Files/WPP2012_HIGHLIGHTS.pdf.
American Association of Neurological Surgeons. Spinal Cord Injury, 2015 (cited 2015). Available at http://www.aans.org/patientinformation/conditionsandtreatments/spinalcordinjury.aspx.
National Pressure Ulcer Advisory Panel, E.P.U.A.P., and Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Clinical Practice Guideline. Cambridge Media: Osborne Park, Western Australia. 2014.
Clay KS, HCPro. Evidence-Based Pressure Ulcer Prevention, vol. 2nd edn. Chapter 1. HCPro Inc., 2008.
Daniel RK, Priest DL, Wheatley DC . Etiologic factors in pressure sores: an experimental model. Arch Phys Med Rehabil 1981; 62: 492–498.
Duncan ST, Levi AD . Multi-tiered treatment of pressure sores in two cynomologous macaques (Macaca fascicularis). J Med Primatol 2001; 30: 283–289.
Nola GT, Vistnes LM . Differential response of skin and muscle in the experimental production of pressure sores. Plast Reconstr Surg 1980; 66: 728–733.
Swaim SF, Bradley DM, Vaughn DM, Powers RD, Hoffman CE. The greyhound dog as a model for studying pressure ulcers. Decubitus 1993; 6: 32–35, 38–40.
Hyodo A, Reger SI, Negami S, Kambic H, Reyes E, Browne EZ . Evaluation of a pressure sore model using monoplegic pigs. Plast Reconstr Surg 1995; 96: 421–428.
Krouskop TA, Reddy NP, Spencer WA, Secor JW . Mechanisms of decubitus ulcer formation—an hypothesis. Med Hypotheses 1978; 4: 37–39.
Lin F, Pandya A, Cichowski A, Modi M, Reprogle B, Lee D . Deep tissue injury rat model for pressure ulcer research on spinal cord injury. J Tissue Viability 2010; 19: 67–76.
Pierce SM, Skalak TC, Rodeheaver GT . Ischemia-reperfusion injury in chronic pressure ulcer formation: a skin model in the rat. Wound Repair Regeneration 2000; 8: 68–76.
Livesley NJ, Chow AW . Infected pressure ulcers in elderly individuals. Clin Infect Dis 2002; 35: 1390–1396.
Rudolph R . Location of the force of wound contraction. Surg Gynecol Obstet 1979; 148: 547–551.
Bosboom EM, Bouten CV, Oomens CW, van Straaten HW, Baaijens FP, Kuipers H . Quantification and localisation of damage in rat muscles after controlled loading; a new approach to study the aetiology of pressure sores. Med Eng Phys 2001; 23: 195–200.
Cui W, Yang LF, Wei WH, Zhu YQ, Wu X, Mu PX et al. Interleukin-17 expression in murine pressure ulcer tissues. Exp Ther Med 2013; 5: 803–806.
Gefen A, Gefen N, Linder-Ganz E, Margulies SS . In vivo muscle stiffening under bone compression promotes deep pressure sores. J Biomech Eng 2005; 127: 512–524.
Goldstein B, Sanders J . Skin response to repetitive mechanical stress: a new experimental model in pig. Arch Phys Med Rehabil 1998; 79: 265–272.
Kokate JY, Leland KJ, Held AM, Hansen GL, Kveen GL, Johnson BA et al. Temperature-modulated pressure ulcers: a porcine model. Arch Phys Med Rehabil 1995; 76: 666–673.
Linder-Ganz E, Engelberg S, Scheinowitz M, Gefen A . Pressure-time cell death threshold for albino rat skeletal muscles as related to pressure sore biomechanics. J Biomech 2006; 39: 2725–2732.
Linder-Ganz E, Gefen A . Mechanical compression-induced pressure sores in rat hindlimb: muscle stiffness, histology, and computational models. J Appl Physiol (1985) 2004; 96: 2034–2049.
Linder-Ganz E, Gefen A . The effects of pressure and shear on capillary closure in the microstructure of skeletal muscles. Ann Biomed Eng 2007; 35: 2095–2107.
Salcido R, Fisher SB, Donofrio JC, Bieschke M, Knapp C, Liang R et al. An animal model and computer-controlled surface pressure delivery system for the production of pressure ulcers. J Rehabil Res Dev 1995; 32: 149–161.
Salcido R, Popescu A, Ahn C . Animal models in pressure ulcer research. J Spinal Cord Med 2007; 30: 107–116.
Linder-Ganz E, Gefen A . Stress analyses coupled with damage laws to determine biomechanical risk factors for deep tissue injury during sitting. J Biomech Eng 2009; 131: 011003.
Linder-Ganz E, Shabshin N, Itzchak Y, Gefen A . Assessment of mechanical conditions in sub-dermal tissues during sitting: a combined experimental-MRI and finite element approach. J Biomech 2007; 40: 1443–1454.
Linder-Ganz E, Shabshin N, Itzchak Y, Yizhar Z, Siev-Ner I, Gefen A . Strains and stresses in sub-dermal tissues of the buttocks are greater in paraplegics than in healthy during sitting. J Biomech 2008; 41: 567–580.
Linder-Ganz E, Yarnitzky G, Yizhar Z, Siev-Ner I, Gefen A . Real-time finite element monitoring of sub-dermal tissue stresses in individuals with spinal cord injury: toward prevention of pressure ulcers. Ann Biomed Eng 2009; 37: 387–400.
Solovyev A, Mi Q, Tzen YT, Brienza D, Vodovotz Y . Hybrid equation/agent-based model of ischemia-induced hyperemia and pressure ulcer formation predicts greater propensity to ulcerate in subjects with spinal cord injury. PLoS Comput Biol 2013; 9: e1003070.
Nguyen PK, Smith AL, Reynolds KJ . A literature review of different pressure ulcer models from 1942-2005 and the development of an ideal animal model. Australas Phys Eng Sci Med 2008; 31: 223–225.
Bergstrand S, Lindberg LG, Ek AC, Linden M, Lindgren M . Blood flow measurements at different depths using photoplethysmography and laser Doppler techniques. Skin Res Technol 2009; 15: 139–147.
Zhang Q, Lindberg LG, Kadefors R, Styf J . A non-invasive measure of changes in blood flow in the human anterior tibial muscle. Eur J Appl Physiol 2001; 84: 448–452.
Acknowledgements
CRG: Research grants from NREF, Burroughs Wellcome Fund and the UNCF Merck Science Initiative. Rachel Sarabia-Estrada: Grants from NASS and AOSpine.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Ahmed, A., Goodwin, C., Sarabia-Estrada, R. et al. A non-invasive method to produce pressure ulcers of varying severity in a spinal cord-injured rat model. Spinal Cord 54, 1096–1104 (2016). https://doi.org/10.1038/sc.2016.61
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2016.61
