
Abstract
Study design:
Retrospective descriptive study.
Objectives:
To evaluate the leg kinematics and motion characteristics within able-bodied (AB) and spinal cord injured (SCI) individuals during stationary semireclined cycling.
Setting:
Functional Performance Laboratory, Connecticut, USA.
Methods:
Three SCI and three AB subjects participated in steady-state leg pedaling (50 revolutions per minute). The SCI group participated in electrical stimulation (FES)-induced cycling at resistances of 0, 6.25, and 12.5 Watts (W). The AB group cycled on the same ergometer without FES at resistances of 0, 60, and 120 W. Motion capture analysis recorded joint angular position, velocity, and acceleration at hip, knee, and ankle. Joint kinematics of hip, knee, and ankle were measured during steady-state leg cycling and comparisons were made between AB and SCI subjects as resistance proportionally and relatively increased.
Results:
Intrasubject hip and knee movement patterns showed minimal variability across resistance levels. Comparisons between AB and SCI subjects showed that the hip and knee kinematics were very similar at all resistance levels. However, ankle movement patterns appeared to increase in variability (increased dorsiflexion) with increased resistance level in AB subjects and less so with SCI subjects. Overall, the ankle kinematics for AB and SCI subjects were dissimilar at resistance levels greater than zero.
Conclusions:
The joint kinematics of the hip, knee, and ankle were found to be periodic, but the differences in ankle kinematics in AB and SCI subjects suggest more emphasise should be placed on the current design of the bike-pedal and subject-specific seat configurations.
Similar content being viewed by others


Introduction
One of the major challenges in the rehabilitation of individuals with spinal cord injury (SCI) is to improve functional independence and prevent the deterioration of musculoskeletal and cardiovascular systems. Stationary FES-induced semireclined leg cycling (FES-LCE) is used clinically as a form of therapeutic exercise to prevent secondary impairments following SCI injury.1, 2, 3 Results from these studies indicate that FES-LCE: (1) increases muscle mass,4, 5, 6 (2) improves strength and endurance,7, 8, 9 (3) facilitates improvements in function,7 (4) increases cardiovascular fitness,7, 8, 10 (5) improves circulation,7, 8, 11 (6) decreases swelling due to edema,12 (7) reduces rate of bone density loss,13, 14 and (8) reduces lower limb blood pooling.15, 16 These results suggest that FES-induced muscle contraction during cycling exercise can be a valuable clinical rehabilitation tool for individuals with SCI in improving rehabilitation outcome, health, and fitness. Studies have also reported that relatively small performance gains can be achieved by some users and the total number of individuals with SCI able to tolerate FES-LCE was minimal.17 Therefore, modification and improvement of this system is warranted especially in order to reduce secondary conditions associated with SCI.
Possible inefficiencies of FES-LCE as an effective exercise system have been reported to be related to the effects of the system's mechanical configuration on cycling performance,17 the effects of FES parameters and number of muscles stimulated on gross efficiency and cycling performance, the effects of FES control paradigms,18, 19 and the effects of FES parameter optimization techniques on maximizing power output (PO) across a range of cycling cadences.20 Although these studies have greatly contributed to the knowledge needed to improve the exercise system, the focus has been primarily on improving the FES control system. Few studies have evaluated the kinematics and motion characteristics of leg cycling in individuals with SCI and how they differ from able-bodied (AB) individuals.
Kinematic analyses are useful in describing motion of the leg segments and joints (hip, knee, and ankle) in terms of their position, velocity and acceleration. In particular, a kinematic analysis of the hip, knee, and ankle during leg cycling may help identify incorrect movement patterns,21, 22, 23 which can be used to design an optimal rider-bike configurations, in order to promote safe and effective pedaling. Understanding the possible differences in leg movement patterns between AB and SCI individuals may provide insight into ways to redesign FES-LCE systems and thus enhance its potential clinical use.
Therefore, the purpose of this study was to compare the joint kinematics and movement patterns of SCI and AB individuals during steady-state semireclined stationary leg cycling at different resistance levels. Differences in movement characteristics were then analyzed and compared between the two groups; leg muscles artificially stimulated (FES-LCE, SCI group) and leg muscles voluntarily activated (LCE, AB group).
Methods
Subjects
Six subjects participated in this study (three SCI and three AB). AB subjects were recruited from student volunteers and were in good health with no history of cardiovascular or musculoskeletal problems. None of the AB subjects were regular users of leg cycling and were considered untrained cyclists (leg cycling <10 miles/week). SCI subjects were all regular users of FES-LCE (have used the system for at least 3 months) and were in good health. The Regional Chapter of the National Spinal Cord Injury Association helped with the recruitment of SCI subjects who were living in the community. Subjects were comparable for their age and anthropometrics characteristics. Table 1 depicts the physical characteristics of the subjects.
Prior to participation, subjects were informed of the nature of this project, the extent of their involvement, the possible benefits/risks, and their right to terminate participation at any time without penalty. Agreement and understanding was indicated by a signed informed consent, which was approved by the university's Institutional Review Board. SCI inclusion criteria: (1) complete or incomplete injury to the spinal cord at or below the fourth cervical spine, (2) age between 20 and 55 years, and (3) previous experience using the FES-LCE system for at least 3 months. SCI exclusion criteria: (1) history of cardiovascular disease, (2) major musculoskeletal impairment, (3) secondary problems due to paralysis, (4) pregnancy, (5) history of smoking, and (6) spinal cord injury sustained less than 1 year.
Experimental protocol
All subjects participated in three 5-min sessions consisting of leg cycling at three different resistance levels. The SCI group participated in the FES-LCE sessions at 35–50 revolutions per minute (rpm) and resistances of 0, 6.25, and 12.5 watts (W). The AB group participated in voluntary reclined cycling on the same ergometer at a crank cadence of 50 rpm and resistances of 0, 60, and 120 W. These resistance levels were chosen based on previous studies of low, medium, and high resistance for both groups. Data were collected for 30 s following 2 min of warm-up at a given resistance. A 5-min rest period was provided for all subjects at the end of each trial. For consistency, both groups were tested on a standard FES-LCE system. AB subjects did not receive FES or use the thigh constraints required for SCI subjects, which provide side-to-side stability of the legs during pedaling. Both AB and SCI subjects used the FES-LCE boot pedals, designed to restrict sagittal and transverse plane movements at the ankle since stimulation to the lower leg muscles is nonexistent.
Procedures
For SCI subjects, the FES-LCE (ERGYS® System, Therapeutic Alliances Inc., Fairborn, OH, USA) provided electrical stimulation to 12 surface electrodes placed on the skin surface over the hamstrings, quadriceps, and gluteal muscle groups (two electrodes for each muscle group). The FES protocol consisted of monophasic square wave pulses of 450 μs duration at a frequency of 30 Hertz (Hz), synchronized for each electrode pair. Horizontal seat depth was adjusted for all subjects so that the knee did not fully extend during maximal downstroke (approximately 110° from vertical). The maximal down stroke was adjusted and a goniometer was used to measure minimal knee flexion between 40° and 45°. The adjusted FES-LCE bike remained unchanged for each subject during testing.
Target cadence was set at 50 rpm for all SCI subjects. During cycling if the cycling cadence dropped below 35 rpm (indicating fatigue) stimulation stopped.
For AB subjects, resistance was applied to the FES-LCE flywheel by a friction-induced band wrapped around the flywheel with a control dial to adjust tension levels. In addition, the FES-LCE system was equipped with a speedometer that allowed each rider to maintain steady-state cycling at approximately 50 rpm.
Measurement of kinematic data
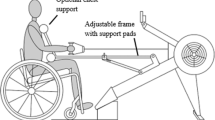
A video-based motion analysis system (Peak Motus® System, Peak Performance Technologies Inc., Denver, CO, USA) recorded, at 60 Hz, was used to evaluate hip, knee, ankle, and crank position during each trial. Retroreflective markers were placed on the left acromion, greater trochanter, lateral epicondyle of femur, lateral malleolus, lateral aspect of 5th metatarsal head, pedal spindle, crank center, and crank shaft tip. Since the lateral malleolus was covered by the boot, a reflective marker was placed directly on the boot-pedal approximate to the lateral malleolus (Figure 1). The video data from the motion of these retroreflective markers were processed to determine the sagittal plane kinematic motions. Raw positional data were filtered with a 5th order, zero-lag, low-pass Butterworth digital filter, with a cutoff frequency of 10 Hz.

Angular kinematic displacements of the hip, knee, ankle, and crank measured in the sagittal plane. *Black circles represent the retroreflective marker locations for the hip, knee, and 5th metatarsal head. A white circle represents the ankle marker, which was placed on the FES-LCE boot approximating the lateral malleolus
The kinematic data were collected for 30 s. Joint angular position, velocity, and acceleration were calculated for the hip, knee, and ankle during three cycling resistance levels for each subject tested with respect to crank position (Figure 1). These data were then ensemble averaged over 10 crank periods during 30 s of data collection at each resistance level. One crank period was defined as a full revolution (360°) of the crank arm about its center. These trials represented the subject's average movement patterns during steady cycling cadence at each resistance condition. The top-dead-position (TDP) was defined as the highest location of the crank relative to the floor. The bottom-dead-position was defined at the lowest location of the crank relative to the floor. The hip angle was defined as the angle formed in the sagittal plane by the long axis of the thigh and the vertical line that intersects the hip and shoulder markers. Knee angle was measured by the angle formed in the sagittal plane between the long axes of the thigh and shank. The ankle angle was defined in the sagittal plane between the long axes of the shank and the foot axes (Figure 1).
Maximum joint excursion, minimum joint excursion, and total joint excursion were determined for each cycle period. Maximum joint excursion was defined as the greatest angular displacement of the distal joint segment relative to the anatomical position (ie, flexion). Minimum joint excursion was defined as the smallest angular displacement of the distal joint segment relative to the anatomical position (ie, extension). The crank positions for maximum and minimum joint excursions were also recorded. Total joint excursion referred to the difference between the maximum and minimum joint excursion. For the ankle, maximum and minimum joint excursion referred to the conventional terminology of dorsiflexion and plantar flexion, respectively. The crank location of zero joint angular velocity indicated the location of transition between joint maximum and minimum excursion (ie, transition between flexion and extension). The rate of this transition was evaluated using the magnitude of the angular acceleration at that same crank location.
Data analysis
For each resistance level, the last ten crank revolutions (pedal cycles) were defined as 10 individual cycling trials for each subject. Each trial was representative of the kinematic changes of either AB subjects or SCI subjects (30 individual trials for each level of resistance for each group) during 360° of crank rotation. Analyses of the kinematic values for the AB and SCI subjects were based on the average of 30 trials at each cycling condition.
Results
Angular kinematic analysis
Referring to Table 2, the angular kinematic patterns were comparable between AB and SCI subjects for the hip and knee, but variations were most apparent in the ankle.
Phase-plane analysis




The phase-planes represented the pattern of joint velocity versus joint displacement for all subjects (Figures 2 and 3).24 Phase-plane trends across resistance levels were consistent within each subject group. However, these trends were not the same between groups. For AB and SCI subjects, the shape of the phase-planes may be generically characterized as elliptical. The area and perimeter of the enclosed ellipses is proportional to the total excursion of the joint. Elliptical phase-planes for the hip and knee are shown in Figures 2 and 3. These smooth curves indicate that smooth transitions of flexion and extension occurred at the hip and knee joints. The SCI subjects presented with limited ankle excursion and angular velocity range (25° to −25°/s).

Phase-Plane analyses of three able-bodied (AB) subjects during steady-state leg cycling (50 rpm) at 0, 60, and 120 W for the hip, knee, and ankle. *Vertical bars extending above and below each data point represent SD about the ensemble average. The rows of graphs correspond to angular velocity versus position graphs for the hip, knee, and ankle. The locations of top-dead-center (TDC) and and bottom-dead-center (BDC) of the crank as well as the direction of crank rotation (arrows) are indicated on the graph. The displacement of the joint into flexion or extension (dorsiflexion or plantar-flexion) is defined along the horizontal axes ( 0 W, 60 W, ▪ ▪ ▪ 120 W)

Phase-Plane analyses of three spinal cord injury (SCI) subjects during steady-state leg cycling (50 rpm) at 0, 6.25, and 12.0 W for the hip, knee, and ankle. *Vertical bars extending above and below each data point represent standard deviations about the ensemble average. The rows of graphs correspond to angular velocity versus position graphs for the hip, knee, and ankle. The locations of top-dead-center (TDC) and bottom-dead-center (BDC) of the crank as well as the direction of crank rotation (arrows) are indicated on the graph. The displacement of the joint into flexion or extension (dorsiflexion or plantar-flexion) is defined along the horizontal axes ( 0 W, 60 W, ▪ ▪ ▪ 120 W)
Discussion
Franco et al (1999) suggested that the bike-rider configuration for some users might compromise knee stability. He evaluated FES-induced leg cycling dynamics of the knee and found that knee joint kinetics in a group of SCI individuals during low resistances were comparable in magnitude to AB individuals cycling at higher resistance levels and cadences.25 The data revealed large knee joint reaction forces opposite in direction to data reported for AB individuals during cycling.
Although movement studies have been carried out on AB individuals during upright leg cycling,26, 27, 28, 29 details comparing the movement characteristics of AB and SCI individuals in semireclined cycling have not been studied nor have there been analyses performed to determine the relationship between changes in pedaling resistance and leg kinematics.
The movements patterns of AB subjects in our study were similar to those reported for AB subjects in previous studies.22, 24, 28, 30 Sagittal plane motions were approximately sinusoidal during semireclined cycling. All AB subjects displayed relatively smooth reversals in flexion and extension at the knee and hip joints as illustrated in the phase-plane analyses (Figure 2). The pattern of knee motion at each resistance level was found to be very similar. The sagittal plane motion of the ankle increased with increased cycling resistance for AB subjects. During sagittal plane motion of the ankle there appeared to be a greater increase of max-flexion (dorsiflexion) as cycling resistance increased.
For this study, we adjusted the seat depth configuration based on an individual's leg length. Therefore, we expected angular displacement to remain relatively constant within subjects and between the AB and SCI groups during cycling. In addition, the consistencies found for the hip and knee excursions of AB and SCI subjects during pedaling were also due in part to the constraints defined by the mechanical bike-rider closed-loop system; the mechanical design of the FES bike system limits movements of the hip and knee in one plane. For safety considerations, the design also assumes that the shank and foot segments are rigidly fixed where the boot-pedal constrains ankle movements for side-to-side stability as well as maintain passive pedal orientation throughout the 360° of crank rotation since the stimulation controls are for the upper leg muscles only. Although the ankle marker could not fully account for all ankle motions that occurred in the boot, the analysis did reveal considerable differences in combined ankle and boot movements between AB and SCI subjects with increased resistance.
The boot-pedal design acts to immobilize the ankle, but total excursion of the ankle still increased as resistance increased for AB subjects. One explanation for this occurrence is that the ankle acts primarily to position the pedal for force transfer from the rider to the pedal crank and less as a power generator. Previous studies suggested that certain pedal angles maximize the transfer of work from the cyclist to the bike.27, 31 However, these observations were not evident in the SCI subjects for obvious reasons; the passive ankle movement patterns in SCI subjects were opposite to that reported for AB subjects cycling against resistance. Furthermore, ankle plantar-flexion occurred at mid to late recovery phase for SCI subjects. This would suggest that although no activation of the lower leg muscles is occurring, the activation of the quadriceps muscles during late recovery phase corresponded to hip flexion and subsequent lifting of the lower leg. The lifting of the lower leg caused the ankle to passively plantar-flex. The passive plantar-flexion mainly induced by inertial boot-pedal forces was also observed in AB subjects 1 and 2 at 0 W resistance.
Our results suggest that cycling resistance levels influence ankle movement patterns for AB subjects. These findings are congruent with previous studies.26 This may be due to the recruitment of lower leg muscles (ie, gastrocnemius, soleus, and tibialis anterior) during leg cycling. In a recent study by Trumbower et al32 the electrical activities of leg muscles were recorded using electromyography (EMG) during semireclined cycling in AB individuals. The results showed that the electrical activity of the gastrocnemius peaked during the mid to late power phase and EMG activity of the tibialis anterior peaked during mid to late recovery phase. These activity patterns parallel the kinematic patterns of ankle plantar-flexion and ankle dorsi-flexion corresponding to mid to late power phase and mid to late recovery phase, respectively. Trumbower et al32 also reported a 199% increase in gastrocnemius muscle activity and a 140% increase in tibialis anterior muscle activity with increasing cycling resistance level (0–120 W).
From a clinical standpoint, applying FES to lower leg muscles is not a new treatment concept. It has been used clinically for the prevention of deep venous thrombosis (DVT) after SCI.33 Moreover, Faghri et al34 evaluated the effects of FES of lower limb muscles during 30 min of upright standing on the central and peripheral hemodynamic response in persons with SCI and concluded that FES could be used as an adjunct during standing to prevent circulatory hypokinesis.34 Implementing FES to lower leg muscles during FES-LCE may provide extended rehabilitation benefits by improving muscle-pumping action of lower leg muscles that increase venous blood return to the heart.
A future modification to the bike design may consider the shank and foot segments as not rigidly fixed. Permitting sagittal plane motion about the ankle joint may be an acceptable alternative to the pre-existing system design. This would require a modification to the current boot-pedal in order to offer pedal forces and orientations that more closely resemble AB semireclined leg cycling. Although increasing the system's degrees-of-freedom (decrease number of constraints) would increase the complexity of FES system controls, it may offer improved joint kinematics and muscle energy transfer. The ability to effectively orient muscle forces to transfer energy from the limbs to the crank could improve the overall effectiveness of pedaling.34 The transmission of the energy from the muscles to the pedal characterizes the pedal force necessary to produce work.
There are a number of possible explanations for the inconsistent movement patterns seen in the SCI group. Although seat configuration was carefully repositioned for each subject, only the seat depth was actually adjusted. This may not necessarily be a sufficient adjustment for a variety of users’ anthropometries. In addition, the FES-LCE uses surface electrodes for muscle stimulation. Although placement of these electrodes was carefully selected prior to testing, it is still difficult to determine the exact location of the motor points and whether the electrode placement and size is appropriate for some individuals. Finally, the inconsistent movement patterns may have been caused by inappropriate muscle responses to FES (ie, spasticity, fatigue), which is very difficult to measure noninvasively.
Clinicians should also keep in mind that integrity of an SCI subject's muscles is heavily influenced by injury-related changes such as: atrophy, contractures, fatigue, and spasticity. Unfortunately, the FES-LCE system always uses the same stimulation-control pattern regardless of a subject's limitations. Therefore, FES control algorithms can only partially contribute to the translation of muscle responses into limb movements. The timing of stimulation is not configuration- or subject-specific and thereby lends itself to amplify the injury-related affects to kinematic variations.
A major clinical consideration is that FES-LCE systems should not be ‘one size fits all’. Individualized modifications to the bike configuration should be made based on a user's movement patterns, response to FES, and anthropometry. The clinical effectiveness and utility of FES-LCE systems requires careful assessment of these indicators.
Additional studies investigating muscle activity patterns and kinetics may further explain the differences observed between AB and SCI individuals and the kinematic changes of the ankle during leg cycling. These studies should focus on the coordination of movements and quantify the characteristics of various movement techniques associated with FES-induced semireclined cycling. Through comprehensive musculoskeletal simulations, it may also be possible to demonstrate an improved FES-LCE exercise system that more closely emulates voluntary leg cycling.
Conclusion
This study provided descriptive analysis of semireclined bike pedaling that may help elucidate the clinical concerns associated with FES-induced leg cycling movements in SCI patients. The joint kinematics of the hip, knee, and ankle were found to be periodic, but the variations in ankle kinematics in AB and SCI subjects suggest more emphasize should be placed on the current design of the bike-pedal and subject-specific seat configurations. It is important to note that this preliminary study was limited by the small sample size. Since only six subjects participated in this kinematics study, we were unable to generalize our findings. However, it is also important to note that little variability existed between the trials of AB subjects. This was expected because geometric constraints of leg cycling limit variability within and between subjects when anthropometry is standardized. Future performance evaluations involving a greater number of subjects that measure not only kinematics but also movement control and coordination through dynamic analyses should also be performed.
References
Faghri P, Votto J, Hovorka C . Venous hemodynamic responses to electrical stimulation. J Phelebol Digest 1999; 4: 19–21.
Figoni SF et al. Acute hemodynamic responses of spinal cord injured individuals to functional neuromuscular stimulation-induced knee extension exercise. J Rehabil Res Dev 1991; 28: 9–18.
Figoni SF et al. Physiologic responses of paraplegics and quadriplegics to passive and active leg cycle ergometry. J Am Paraplegia Soc 1990; 13: 33–39.
Chilibeck PD, Jeon J, Weiss C, Bell G, Burnham R . Histochemical changes in muscle of individuals with spinal cord injury following functional electrical stimulated exercise training. Spinal Cord 1999; 37: 264–268.
Hjeltnes N et al. Improved body composition after 8 wk of electrically stimulated leg cycling in tetraplegic patients. Am J Physiol 1997; 273: R1072–R1079.
Mohr T et al. Long-term adaptation to electrically induced cycle training in severe spinal cord injured individuals. Spinal Cord 1997; 35: 1–16.
Figoni S . Perspectives on cardiovascular fitness and SCI. J Am Paraplegia Soc 1990; 13: 63–71.
Phillips W, Burkett LN, Munro R, Davis M, Pomeroy K . Relative changes in blood flow with functional electrical stimulation during exercise of the paralyzed lower limbs. Paraplegia 1995; 33: 90–93.
Gerrits HL, de Haan A, Sargeant AJ, Dallmeijer A, Hopman MT . Altered contractile properties of the quadriceps muscle in people with spinal cord injury following functional electrical stimulated cycle training. Spinal Cord 2000; 38: 214–223.
Faghri PD, Glaser RM, Figoni SF . Functional electrical stimulation leg cycle ergometer exercise: training effects on cardiorespiratory responses of spinal cord injured subjects at rest and during submaximal exercise. Arch Phys Med Rehabil 1992; 73: 1085–1093.
Faghri P, Votto J, Hovorka C . The effects of electrical calf muscle stimulation and voluntary exercise on venous blood flow. Med Sci Sport Exerc 1997; 29: S174.
Faghri PD . The effects of neuromuscular stimulation-induced muscle contraction versus elevation on hand edema in CVA patients. J Hand Ther 1997; 10: 29–34.
Rodgers MM et al. Musculoskeletal responses of spinal cord injured individuals to functional neuromuscular stimulation-induced knee extension exercise training. J Rehabil Res Dev 1991; 28: 19–26.
Hangartner T, Rodgers M, Glaser R, Barre P . Tibial bone density loss in spinal cord injured patients: effects of FES exercise. J Rehabil Res 1994; 31: 50–61.
Faghri PD, Van Meerdervort HF, Glaser RM, Figoni SF . Electrical stimulation-induced contraction to reduce blood stasis during arthroplasty. IEEE Trans Rehabil Eng 1997; 5: 62–69.
Phillips WT et al. Effect of spinal cord injury on the heart and cardiovascular fitness. Curr Probl Cardiol 1998; 23: 641–716.
Schutte L, Rodgers M, Zajac F, Glaser R . PhD Dissertation. Stanford University, Palo Alto, CA, 1993.
Rodgers M et al. In: Biewener AA, Goel VK (eds). American Society of Biomechanics 17th Annual Meeting. Iowa City, IA, 1993, pp 175–176.
Glaser R et al. In: Enders A, Hall M (eds). RESNA ’96 – Exploring New Horizons: Pioneering the 21st Century. Washington, DC 1996, pp 279–281.
Gfohler M, Lugner P . Cycling by means of functional electrical stimulation. IEEE Trans Rehabil Eng 2000; 8: 233–243.
Nordeen-Snyder KS . The effect of bicycle seat height variation upon oxygen consumption and lower limb kinematics. Med Sci Sports 1977; 9: 113–117.
Houtz SJ, Fischer FJ . An analysis of muscle action and joint excursion during exercise on a stationary bicycle. J Bone Joint Surg Am 1959; 41-A: 123–131.
Bailey MP, Maillardet FJ, Messenger N . Kinematics of cycling in relation to anterior knee pain and patellar tendinitis. J Sports Sci 2003; 21: 649–657.
Rosecrance JC, Giuliani CA . Kinematic analysis of lower-limb movement during ergometer pedaling in hemiplegic and nonhemiplegic subjects. Phys Ther 1991; 71: 334–343.
Franco JC, Perell KL, Gregor RJ, Scremin AM . Knee kinetics during functional electrical stimulation induced cycling in subjects with spinal cord injury: a preliminary study. J Rehabil Res Dev 1999; 36: 207–216.
Hull ML, Kautz S, Beard A . An angular velocity profile in cycling derived from mechanical energy analysis. J Biomech 1991; 24: 577–586.
Hull ML, Jorge M . A method for biomechanical analysis of bicycle pedalling. J Biomech 1985; 18: 631–644.
Neptune RR, Herzog W . Adaptation of muscle coordination to altered task mechanics during steady-state cycling. J Biomech 2000; 33: 165–172.
Boylls CC, Zomlefer MR, Zajac FE . Kinematic EMG reactions to imposed interlimb phase alterations during bipedal cycling. Brain Res 1984; 324: 342–345.
Smak W, Neptune R, Hull M . The influence of pedaling rate on bilateral asymmetry in cycling. J Biomech 1999; 32: 899–906.
Fregly BJ, Zajac FE . A state-space analysis of mechanical energy generation, absorption, and transfer during pedaling. J Biomech 1996; 29: 81–90.
Trumbower RD, Faghri PD . Improving pedal power during semireclined leg cycling. IEEE Eng Med Biol Mag 2004; 23: 62–71.
Mysiw W, Jackson R . In: Braddom L (ed). Physical Medicine and Rehabilitation. WB Saunders Co.: Philadelphia 1996, pp 464–491.
Faghri PD, Yount JP, Pesce WJ, Seetharama S, Votto JJ . Circulatory hypokinesis functional electric stimulation during standing in persons with spinal cord injury. Arch Phys Med Rehabil 2001; 82: 1587–1595.
Acknowledgements
This study was supported in part by University of Connecticut Research Foundation, Storrs Connecticut, USA.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Trumbower, R., Faghri, P. Kinematic analyses of semireclined leg cycling in able-bodied and spinal cord injured individuals. Spinal Cord 43, 543–549 (2005). https://doi.org/10.1038/sj.sc.3101756
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101756
Keywords
This article is cited by
-
Lower-extremity joint kinematics and muscle activations during semi-reclined cycling at different workloads in healthy individuals
Journal of NeuroEngineering and Rehabilitation (2014)
-
Leg joint power output during progressive resistance FES-LCE cycling in SCI subjects: developing an index of fatigue
Journal of NeuroEngineering and Rehabilitation (2008)
