
Abstract
OBJECTIVE:
Observations on a cohort of neonates in the preintervention year of the field trial of home-based neonatal care (HBNC) in rural Gadchiroli, India, showed that preterm birth and low birth weight (LBW), <2500 g, constituted the most important risk factors. Owing to a limited access to hospital care, most neonates were managed at home in the subsequent intervention years. The objective of this paper is to evaluate the feasibility and effectiveness of managing LBW and preterm neonates in home setting.
DESIGN:
We retrospectively analyzed data from the intervention arm (39 villages) in the HBNC trial. Feasibility was assessed by coverage and by quality (19 indicators) of care. Effectiveness was evaluated by change in case fatality (CF) and in the incidence of comorbidities in LBW or preterm neonates by comparing the preintervention year (1995 to 1996) with the intervention years (1996 to 2003).
RESULTS:
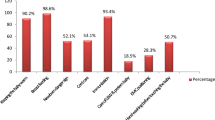
During 1996 to 2003, total 5919 live births occurred in the intervention villages, out of whom 5510 (93%) received HBNC. These included 2015 LBW neonates and 533 preterm neonates, out of whom 97% received only home-based care. The coverage and quality of interventions assessed on 19 indicators was 80.5%. The CF in LBW neonates declined by 58% (from 11.3 to 4.7%, p<0.001), and in preterm neonates, by 69.5% (from 33.3 to 10.2%, p<0.0001). Incidence of the major comorbidities, viz., sepsis, asphyxia, hypothermia and feeding problems, declined significantly. Preterm-LBW neonates without sepsis (270) received only supportive care — CF in them decreased from 28.2 to 11.5% (p<0.01), and those with sepsis (53) received supportive care and antibiotics — CF in them decreased from 61 to 13.2% (p<0.005). Supportive care contributed 75% and treatment with antibiotics 25% in the total averted deaths in preterm-LBW neonates. The intrauterine growth restriction (IUGR)-LBW neonates without sepsis (1409) received only supportive care — the CF was unchanged, and 181 with sepsis received supportive care and antibiotics — the CF decreased from 18.4 to 8.8% (p<0.05). Treatment with antibiotics explained entire reduction in mortality in IUGR neonates. In total, 55 deaths in LBW neonates were averted by supportive care and 35 by the treatment with antibiotics.
CONCLUSIONS:
Home-based management of LBW and the preterm neonates is feasible and effective. It remarkably improved survival by preventing comorbidities, by supportive care, and by treating infections.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others

References
Save the children. State of the World's Newborns. Save the Children. Washington, DC; 2001.
Kramer MS . Intrauterine growth and gestation determinants. Pediatrics 1987;80(4):502–511.
Kramer MS . Effect of energy and protein intakes on pregnancy outcome: an overview of the research evidence from controlled clinical trials. Am J Clin Nutr 1993;58:627–635.
Ramakrishnan U, Neufeld LM . Recent advances in nutrition and intrauterine growth. In: Martorell R, Haschke F, editors. Nutrition and Growth. Nestle Nutrition Workshop Series, Pediatric Program, Vol. 47. Philadelphia: Veveyi/Lippincott Williams and Wilkins; 2001. p. 97–120.
Ceesay SN, Prentice AM, Cole TJ, et al. Effects on birth weight and perinatal mortality of maternal dietary supplements in rural Gambia: 5 year randomised controlled trial. BMJ 1997;315:786–790.
Bang AT, Bang RA, Baitule S, Deshmukh M, Reddy MH . Burden of morbidities and the unmet need for health care in rural neonates — a prospective observational study in Gadchiroli, India. Indian Pediatr 2001;38:952–965.
Bang AT, Reddy HM, Baitule SB, Deshmukh MD, Bang RA . The incidence of morbidities in a cohort of neonates in rural Gadchiroli, India: seasonal & temporal variation: a hypothesis about prevention. J Perinatol 2005;25:S18–S28.
Bang AT, Reddy HM, Bang RA, Deshmukh M . Why do neonates die in rural Gadchiroli, India? (Part II): Estimating population attributable risks and contribution of multiple morbidities for identifying a strategy to prevent deaths. J Perinatol 2005;25:S35–S43.
Bang AT, Bang RA, Baitule S, Reddy MH, Deshmukh M . Effect of home-based neonatal care and management of sepsis on neonatal mortality: field trial in rural India. Lancet 1999;354:1955–1961.
Bang AT, Bang RA . Background of the field trial of home-based neonatal care in Gadchiroli, India. J Perinatol 2005;25:S3–S10.
Bang AT, Bang RA, Reddy HM, et al. Methods and the baseline situation in the field trial of home-based neonatal care in Gadchiroli, India. J Perinatol 2005;25:S11–S17.
Bang AT, Bang RA, Stoll BJ, Baitule SB, Reddy HM, Deshmukh MD . Is home-based diagnosis and treatment of neonatal sepsis feasible and effective? Seven years of intervention in the Gadchiroli field trial (1996–2003). J Perinatol 2005;25:S62–S71.
Reddy HM, Bang AT . How to identify neonates at the risk of death in rural India: clinical criteria for the risk approach. J Perinatol 2005;23:S44–S50.
Bergman NJ, Jurisoo LA . The “Kangaroo” method for treating low birth weight babies in a developing country. Trop Doc 1994;24(2):57–60.
Bang AT, Bang RA, Reddy HM, Deshmukh MD, Baitule S . Reduced incidence of neonatal morbidities: effect of home-based neonatal care in rural Gadchiroli, India. J Perinatol 2005;25:S51–S61.
Bang AT, Reddy HM, Deshmukh MD, Baitule SB, Bang RA . Neonatal and infant mortality in the 10 years (1993 to 2003) of the Gadchiroli field trial: Effect of home-based neonatal care. J Perinatol 2005;25:S92–S107.
Goldenberg RL, Rouse DJ . Prevention of premature birth. N Engl J Med 1998;339(5):313–332.
Standing H, Costello A . Social and developmental issues affecting perinatal health of mothers and their infants. In: Costello A, Manandhar D, editors. Improving Newborn Infant Health in Developing Countries. London: Imperial College Press; 2000. p. 79–98.
Conde-Agudelo A, Diaz-Rosello JL, Belizan JM . Kangaroo mother care to reduce morbidity and mortality in low birth weight infants. Cochrane Database System Rev 2004;1:1–23.
Pratinidhi A, Shah U, Shrotri A, Bodhani N . Risk approach strategy in neonatal care. Bull WHO 1986;64(2):291–297.
Datta N, Kumar V, Kumar L . Application of case management to the control of acute respiratory infections in low birth weight infants: a feasibility study. Bull World Health Organization 1987;5:77–82.
National Neonatology Forum, India. National Neonatal Perinatal Database: Year 2000. India, New Delhi: National Neonatology Forum; 2001.
Bang AT, Bang R A, Reddy HM . Home-based neonatal care: Summary and applications of the field trial in rural Gadchiroli, India (1993 to 2003). J Perinatol 2005;25:S108–S122.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work was financially Supported by the John D. and Catherine T. MacArthur Foundation, The Ford Foundation, Saving Newborn Lives, Save the Children, USA and Bill & Melinda Gates Foundation.
Rights and permissions
About this article
Cite this article
Bang, A., Baitule, S., Reddy, H. et al. Low Birth Weight and Preterm Neonates: Can they be Managed at Home by Mother and a Trained Village Health Worker?. J Perinatol 25 (Suppl 1), S72–S81 (2005). https://doi.org/10.1038/sj.jp.7211276
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jp.7211276
This article is cited by
-
Training programs to improve identification of sick newborns and care-seeking from a health facility in low- and middle-income countries: a scoping review
BMC Pregnancy and Childbirth (2021)
-
Community health workers at the dawn of a new era: 6. Recruitment, training, and continuing education
Health Research Policy and Systems (2021)
-
Evaluating the efficacy of a multistrain probiotic supplementation for prevention of neonatal sepsis in 0–2-month-old low birth weight infants in India—the “ProSPoNS” Study protocol for a phase III, multicentric, randomized, double-blind, placebo-controlled trial
Trials (2021)
-
Lower mortality is observed among low birth weight young infants who have received home-based care by female community health volunteers in rural Nepal
BMC Pregnancy and Childbirth (2017)
-
Home-based neonatal care by community health workers for preventing mortality in neonates in low- and middle-income countries: a systematic review
Journal of Perinatology (2016)
