
Abstract
BACKGROUND: The prevalence of adiposity in childhood is increasing. Is breast-feeding protective as suggested by cross-sectional studies?
OBJECTIVE: In a longitudinal birth cohort study, we tested whether breast-feeding for more than 2 months has preventive effects against overweight and adiposity at 6?y.
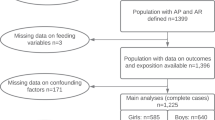
DESIGN: Of 1314 children representing the catchment areas of six delivery units, 918 could be followed up to the age of 6?y. Height, weight, and skin-fold thickness were measured at regular visits. As the criteria of overweight, obesity, and adiposity in the children, the 90th and the 97th percentiles of BMI and skin-fold values were used. Parents with a BMI at or above the 90th percentile, which was 27?kg/m2 or more, were considered overweight. Infants bottle-fed from birth or breast-fed for less than 3 months were classified as ‘bottle-fed’ (BO), and those breast-fed for 3 months and more as ‘breast-fed’ (BR). Univariate comparisons and logistic regression analysis were performed applying SAS 6.12. The final logistic model consisted of the 480 cases for whom complete data for all variables were available. The potential effect of loss to follow-up was analysed by the Cochran–Mantel–Haenzel test: the outcomes were not significantly influenced by loss to follow-up.
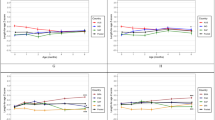
RESULTS: At birth BMIs were nearly identical in both groups. By 3 months, BO had significantly higher BMIs and thicker skin folds than BR. From 6 months on, compared to BR, a consistently higher proportion of BO children exceeded the 90th and the 97th percentile of BMI and skin-fold thickness reference values. From the age of 4?y to 5 and 6?y, in BO the prevalence of obesity nearly doubled and tripled, respectively. With only minor changes of obesity prevalence in BR, the difference of BMI and skin-fold thickness between groups became statistically significant. Logistic regression analysis revealed that overweight of the mother, maternal smoking during pregnancy, bottle feeding, and low social status remained important risk factors for overweight and adiposity at 6?y of age.
CONCLUSION: A maternal BMI of ≥27, bottle-feeding, maternal smoking during pregnancy, and low social status are risk factors for overweight and adiposity at 6?y of age. Early bottle-feeding brings forward the obesity rebound, predictive of obesity in later life.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others

References
Hanley AJG, Harris SB, Gittelsohn J, Wolever TMS, Saksvig B, Zinman B . Overweight among children and adolescents in a Native Canadian community: prevalence and associated factors. Am J Clin Nutr 2000; 71: 693–700.
Goran MI . Metabolic precursors and effects of obesity in children: a decade of progress. Am J Clin Nutr 2001; 73: 158–171.
Chinn S, Rona RJ . Prevalence and trends in overweight and obesity in three cross sectional studies of British children, 1974–94. BMJ 2001; 322: 24–26.
Von Kries R, Koletzko B, Sauerwald T, von Mutius E, Barnert D, Grunert V, von Voss H . Breast feeding and obesity: cross sectional study. BMJ 1999; 319: 147–150.
Hediger ML, Overpeck MD, Kuczmarski RJ, Ruan WJ . Association between infant breastfeeding and overweight in young children. JAMA 2001; 285: 2453–2460.
Gillman MW, Rifas-Shiman SL, Camargo CA, Berkey CS, Frazier AL, Rockett HRH, Field AE, Colditz GA . Risk of overweight among adolescents who were breastfed as infants. JAMA 2001; 285: 2461–2467.
Liese AD, Hirsch T, von Mutius E, Keil U, Leupold W, Weiland SK . Inverse association of overweight and breast feeding in 9–10-y-old children in Germany. Int J Obes Relat Metab Disord 2001; 25: 1644–1650.
Kramer MS . Do breast-feeding and delayed introduction of solid foods protect against subsequent obesity? J Pediatr 1981; 98: 883–887.
Sokol RJ . The chronic disease of childhood obesity: the sleeping giant has awakened. Editorial. J Pediatr 2000; 136: 711–713.
Bergmann KE, Bergmann RL . Therapie der Adipositas im Kindesalter. Pädiatr Grenzgeb 1997; 35: 409–424.
Butte NF . The role of breast feeding in obesity. Pediatr Clin North Am 2001; 48: 189–198.
Bergmann RL, Edenharter G, Bergmann KE, Forster J, Bauer CP, Wahn V, Zepp F, Wahn U . Atopic dermatitis in early infancy predicts allergic airway disease at 5 years. Clin Exp Allergy 1998; 28: 965–970.
Bergmann RL, Dudenhausen JW, Bergmann KE, Schmidt E, Wahn U . Wie werden Säuglinge in Deutschland ernährt. Ergebnisse aus der multizentrischen Allergiestudie am Geburtsjahrgang 1990. Monatsschr Kinderheilkd. 1994; 142: 412–417.
Cameron N . The methods of auxological anthropometry. In: Falkner F, Tanner JM (eds). Human growth. 2nd edn. Plenum Press: New York and London; 1986. pp 3–46.
Rolland-Cachera MF, Cole TJ, Sempé M, Tichet J, Rossignol C, Charraud A . Body mass index variations: centiles from birth to 87 years. Eur J Clin Nutr 1991; 45: 13–21.
Prader A, Largo RH, Molinari L, Issler C . Physical growth of Swiss children from birth to 20 years of age. Helv Paediatr Acta 1989; 52 (Suppl): 82–85.
Winkler J . Die Messung des sozialen Status mit Hilfe eines Index in den Gesundheitssurveys der DHP (Scaling social status in the German National Health Surveys). In: Ahrens W, Bellach B, Jökel KH (eds). Messung soziodemographischer Merkmale in der Epidemiologie. RKI-Schriften: MMV München; 1998. pp 69–74.
Bergmann KE, Mensink GBM . Körpermaße und Übergewicht. In: Bundesgesundheits-Survey. Gesundheitswesen. Sonderheft 1999; 2: S115–S120.
Bergmann RL, Edenharter G, Bergmann KE, Lau S, Wahn U the MAS-Research Group Socioeconomic status is a risk factor for allergy in parents but not in their children. Clin Exp Allergy 2000; 30: 1740–1745.
Anderson TA, Fomon SJ . Beikost. In: Fomon SJ (ed). Infant nutrition. Saunders: Philadelphia; 1974. pp 408–434.
Bouchard C, Pérusse L . Genetics of obesity. Annu Rev Nutr 1993; 13: 337–354.
Rolland-Cachera M-F, Deheeger M, Bellisle F, Sempé M, Guilloud-Bataille M, Patois E . Adiposity rebound in children: a simple indicator for predicting obesity. Am J Clin Nutr 1984; 39: 129–135.
Baranowski T, Rassin DK, Harrison JA, Henske JC . Ethnicity, infant-feeding practices, and childhood adiposity. J Dev Behav Pediatr 1990; 11: 234–239.
Dietz W . Factors associated with childhood obesity. Nutrition 1991; 7: 290–291.
Thefeld W, Bergmann KE, Hermann-Kunz E, Junge B, Knopf H, Melchert H-U, Mensink G, Stolzenberg H, Tietze K . Wohnortgröße und Gesundheit Stadt-/Land- Unterschiede. In: Belach B-M (ed). Die Gesundheit der Deutschen, Chapter 1. RKI-Hefte 15/96. Robert Koch – Institut: Berlin; 1996.
Stunkard AJ, Harris JR, Pedersen RL, Mc Clearn GE . The body mass index of twins who have been reared apart. New Engl J Med 1990; 322: 1483–1487.
Stunkard AJ, Berkowitz RI, Stallings VA, Schoeller DA . Energy, intake not energy output, is a determinant of body size in infants. Am J Clin Nutr 1999; 69: 524–530.
McCance DR, Pettitt DJ, Hanson RL, Jacobsson LT, Knowler WC, Benett PH . Birth weight and non-insulin dependent diabetes: thrifty genotype, thrifty phenotype, or surviving small baby genotype? BMJ 1994; 308: 942–945.
Friedman JM . Molecular genetic approaches to complex traits. In: Bouchard C, Bray GA (eds). Regulation of body weight: Biological and Behavioral Mechanisms. Wiley & Sons: Chichester; 1996. pp 251–269.
Bergmann KE, Bergmann RL, Eisenberg A . Offspring of diabetic mothers have a higher risk for childhood overweight than offspring of diabetic fathers. Nutr Res 1984; 4: 545–552.
Pettitt DJ . Long-term effects of the intrauterine environment, birth weight, and breast-feeding in Pima Indians. Diabetes Care 1998; 21: B138–B141.
Vohr BR, McGarvey ST, Tucker R . Effects of maternal gestational diabetes on offspring adiposity at 4–7 years of age. Diabetes Care 1999; 22: 1284–1291.
Whitaker RC, Dietz WH . Role of the prenatal environment in the development of obesity. J Pediatr 1998; 132: 768–776.
Hilson JA, Rasmussen KM, Kjolhede CL . Maternal obesity and breast-feeding success in a rural population of white women. Am J Clin Nutr 1997; 66: 1371–1378.
Bergmann RL, Diepgen TL, Kuss O, Bergmann KE, Sommerfeld C, Kujat J, Wahn U . Breastfeeding duration is a risk factor for atopic eczema. Clin Exp Allergy 2002; 32: 205–209.
Ravelli GP, Stein ZA, Susser MW . Obesity in young men after famine exposure in utero and early infancy. N Engl J Med 1976; 295: 349–353.
Dörner G, Plagemann A . Perinatal hyperinsulinism as a possible predisposing factor for diabetes mellitus, obesity, and enhanced cardiovascular risk in later life. Horm Metab Res 1994; 26: 213–221.
Ong KK, Ahmed ML, Emmett PM, Preece MA, Dunger DB . Association between postnatal catch-up growth and obesity in childhood: prospective cohort study. BMJ 2000; 320: 967–971.
Eriksson JG, Forsén T, Tuomilchto J, Osmond C, Barker DJP . Early growth and coronary heart disease in later life: longitudinal study. BMJ 2001; 822: 949–953.
von Kries R, Hermann M, Grunert VP, von Mutius E . Is obesity a risk factor for childhood asthma? Allergy 2001; 56: 318–322.
Young SY, Gunzenhauser JD, Malone KE, McTiernan A . Body mass index and asthma in the military population of the northwestern United States. Arch Int Med 2001; 161: 1605–1611.
Kark JD, Troya G, Friedlander Y, Slater PE, Stein Y . Validity of maternal reporting of breast feeding history and the association with blood lipids in 17 year olds in Jerusalem. J Epidemiol Community Health 1984; 38: 218–225.
Yoneyama K, Nagata H, Asano H . Growth of Japanese breast-fed infants from birth to 20 months. Ann Hum Biol 1994; 21: 597–608.
Fomon SJ, Rogers R, Ziegler EE, Nelson SE, Thomas L . Indices of fatness and serum cholesterol at age 8 years in relation to feeding and growth during early infancy. Pediatr Res 1984; 18: 1233–1238.
Fomon SJ, Filer LJ, Thomas LN, Rogers RR . Growth and serum chemical values of normal breastfed infants. Acta Pediatr Scand 1978; 273: 1–29.
World Health Organization/United Nations Children's Fund. Ten steps to successful breastfeeding in protection, promotion and support of breastfeeding: the special role of maternity services. World Health Organization/United Nations Children's Fund: Geneva Switzerland; 1989.
Elliott KG, Kjolhede CL, Gournis E, Rasmussen KM . Duration of breastfeeding associated with obesity during adolescence. Obesity Res 1997; 5: 538–541.
Lucas A, Boyes S, Bloom R, Aynsley-Green A . Metabolic and endocrine responses to a milk feed in six-day-old term infants: differences between breast and cow's milk formula feeding. Acta Paediatr Scand 1981; 70: 195–200.
Salmenperä L, Perheentupa J, Siimes MA, Adrian TE, Bloom SR, Aynsley-Green A . Effects of feeding regimen on blood glucose levels and plasma concentrations of pancreatic hormones and gut regulatory peptides at 9 months of age: comparison between infants fed with milk formula and infants exclusively breast-fed from birth. J Pediatr Gastroenterol Nutr 1988; 7: 651–656.
Dewey KG . Nutrition, growth, and complementary feeding of the breastfed infant. Pediatr Clin North Am 2001; 48: 87–104.
Kent JC, Mitoulas L, Cox DB, Owens RA, Hartmann PE . Breast volume and milk production during extended lactation in women. Exp Physiol 1999; 84: 435–447.
Matheny RJ, Birch LL, Picciano MF . Control of intake by human-milk-fed infants: relationships between feeding size and interval. Developmental Psychobiology 1990; 23: 511–518.
Bergmann RL, Bergmann KE . Nutrition and growth infancy. In: Falkner F, Tanner JM (eds). Human growth. A comprehensive treatise, 2nd edn, Vol III: Methodology, ecological genetic and nutritional effects on growth. Plenum Press: New York; 1986, pp 389–413.
Widdowson ME, Mc Cance RA . A review: new thoughts on growth. Pediatr Res 1975; 9: 154–156.
Birch LL, Fisher JO . Development of eating behaviors among children and adolescents. Pediatrics 1998; 101: 539–549.
Levin BE . Metabolic imprinting on genetically predisposed neural circuits perpetuates obesity. Nutrition 2000; 16: 909–915.
Ounsted M, Sleigh G . The infant's self-regulation of food intake and weight gain. Difference in metabolic balance after growth constraint or acceleration in utero. Lancet 1975; 7922: 1393–1397.
Stettler N, Zemel BS, Kumanyika S, Stallings VA . Infant weight gain and childhood overweight status in a multicenter cohort study. Pediatrics 2002;109: 194–199.
Wilson AC, Forsyth JS, Greene SA, Irvine L, Hau C, Howie PW . Relation of infant diet to childhood health: seven year follow up of cohort of children in Dundee infant feeding study. BMJ 1998; 316: 21–25.
Blake KV, Gurrin LC, Evans SF, Beilin LJ, Landau LI, Stanley FJ, Newnham JP . Maternal cigarette smoking during pregnancy, low birth weight and subsequent blood pressure in early childhood. Early Hum Development 2000; 57: 137–147.
Bergmann KE, Bergmann RL, Schulz J, Graß T, Wahn U . Prediction of atopic disease in the newborn: methodological aspects. Clin Experim Allergy 1990; 203 (Suppl): 21–26.
Rothman KJ, Greenland S . Modern epidemiology. 2nd edn. Lippincott-Raven: Philadelphia; 1998.
Kramer MS, Chalmers B, Hodnett ED, Sevkovskaya Z, Dzikovich I, Shapiro S, Collet J-P, Vanilovich I, Mezen I, Ducruet T, Shishko G, Zubovich V, Mknuik D, Gluchanina E, Dombrovskiy V, Ustinovitch A, Kot T, Bogdanovich N, Ovchinikova L, Helsing E . Promotion of Breastfeeding Intervention Trial (PROBIT). A randomized trial in the Republic of Belarus. JAMA 2001; 285: 413–420.
Acknowledgements
Supported by a grant of the German Federal Ministry of Research and Technology BMBF # 01 EE 9406/8
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bergmann, K., Bergmann, R., von Kries, R. et al. Early determinants of childhood overweight and adiposity in a birth cohort study: role of breast-feeding. Int J Obes 27, 162–172 (2003). https://doi.org/10.1038/sj.ijo.802200
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ijo.802200
Keywords
This article is cited by
-
Birth outcomes and early growth patterns associated with age at adiposity rebound: the Ma’anshan birth cohort (MABC) study
BMC Public Health (2023)
-
Prolonged breastfeeding protects from obesity by hypothalamic action of hepatic FGF21
Nature Metabolism (2022)
-
The Role of Children’s Dietary Pattern and Physical Activity in the Association Between Breastfeeding and BMI at Age 5: The GECKO Drenthe Cohort
Maternal and Child Health Journal (2021)
-
Grow well/Crecer bien: a protocol for research on infant feeding practices in low-income families
BMC Public Health (2020)
-
Diabetes Management During Breastfeeding in Women with Type 1 Diabetes
Current Diabetes Reports (2020)
