
Abstract
OBJECTIVES: To determine whether girls and boys categorized from body mass index (BMI) values as overweight or obese for their age have lower bone mineral content (BMC) or lower bone area in relation to total body weight than children of normal adiposity.
DESIGN: Cross-sectional study in a university bone research unit.
SUBJECTS: Two hundred girls and 136 boys aged 3–19 y recruited from the general population by advertisement.
MEASUREMENTS: Total body BMC (g) and bone area (cm2) measured by dual energy X-ray absorptiometry (DXA) in relation to body weight (kg), lean tissue mass (kg) and fat mass (kg) in boys and girls of three different BMI percentile groupings: normal weight (BMI<85th percentile); overweight (85 to 94th BMI percentile); obese (≥95th BMI percentile).
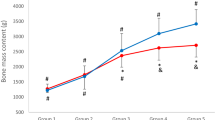
RESULTS: Obese children had higher BMC, bone area, and fat mass for chronological age than those of normal body weight (P<0.001). In spite of this the observed values for age-adjusted total body BMC and bone area relative to body weight were each lower than predicted values, in both overweight and obese children (2.5–10.1% less, P<0.05) than in children of lower adiposity.
CONCLUSION: In overweight and obese boys and girls there is a mismatch between body weight and bone development during growth: their bone mass and bone area are low for their body weight.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others
References
Prentice A, Jebb S . Obesity in Britain: gluttony or sloth? Br Med J 1995 311: 437–439.
Gortmaker S, Must A, Sobol A, Peterson K, Colditz G, Dietz W . Television viewing as a cause of increasing obesity among children in the US, 1986–90 Arch Pediatr Adolesc Med 1996 150: 356–362.
Rossner S . Childhood obesity and adulthood consequences Acta Paediatrica 1998 87: 1–5.
Slemenda CW, Miller JZ, Hui SL, Reister TK, Johnston CC . Role of physical activity in the development of skeletal mass in children J Bone Min Res 1991 11 (6): 1227–1233.
Frost H . Obesity, and bone strength and ‘mass’: a tutorial based on insights from a new paradigm Bone 1997 21:: 211–214.
Klein KO, Larmore KA, de Lancey E, Brown JM, Considine RV, Hassink SG . Effect of obesity on estradiol level, and its relationship to leptin, bone maturation, and bone mineral density in children J Clin Endocrinol Metab 1998 83 (10): 3469–3475.
Goulding A, Cannan R, Williams S, Gold E, Taylor R, Lewis-Barned N . Bone mineral density in girls with forearm fractures J Bone Min Res 1998 13: 143–148.
Goulding A, Taylor R, Jones I, McAuley K, Manning P . Fractures: are overweight children at increased risk? Conference Proc NZ Dietetic Assoc 1998 3: 68–70.
Zamboni G, Soffiati M, Giavarina D, Tato L . Mineral metabolism in obese children Acta Paediat Scandinav 1988 77: 741–746.
McCormick DP, Ponder SW, Fawcett D, Palmer JL . Spinal bone mineral density in 335 normal and obese children and adolescents: evidence for ethnic and sex differences J Bone Min Res 1991 6:: 507–513.
De Schepper J, Van den Broeck M, Jonckheer MH . Study of lumbar spine bone mineral density in obese children Acta Paediatr 1995 84: 313–315.
Loder R, Aronson D, Greenfield M . The epidemiology of bilateral slipped capital femoral epiphysis J Bone Joint Surg 1993 75A: 1141–1147.
Davids J, Huskamp M, Bagley A . A dynamic biomechanical analysis of the etiology of adolescent tibia vara J Pediat Orthop 1996 16: 461–468.
Must A, Dallal G, Dietz W . Reference data for obesity: 85th and 95th percentiles of body mass index (Wt/ht2)—a correction Am J Clin Nutr 1991 54: 773.
Draper N, Smith H . Applied regression analysis, Second edition Wiley: New York 1981.
Tanner JM, Whitehouse RH . Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty Arch Dis Child 1976 51: 170–179.
Svendsen O, Haarbo J, Christiansen C . Accuracy of measurements of body composition by dual-energy X-ray absorptiometry in vivo Am J Clin Nutr 1993 57: 605–608.
Jensen L, Quaade F, Sorensen O . Bone loss accompanying voluntary weight loss in obese humans J Bone Min Res 1994 9: 459–463.
Van Loan M, Johnson H, Barbieri T . Effect of weight loss on bone mineral content and bone mineral density in obese women Am J Clin Nutr 1998 67: 734–738.
Pritchard J, Nowson C, Wark J . Bone loss accompanying diet-induced or exercise-induced weight loss: a randomised controlled study Int J Obes 1996 20: 513–520.
De Simone M, Farello G, Palumbo M, Gentile T, Ciuffreda M, Olioso P, Cinque M, De Matheis F . Growth charts, growth velocity and bone development in childhood obesity Int J Obes 1995 19: 851–857.
Southern M, Loftin M, Suskind R, Udall J, Wilson J, Hensel L, Hargis J, Blecker U . The impact of mild, moderate and severe obesity on upper and lower bone mineral content, lean and fat body mass Int J Obes 1998 22 (Suppl 3): P383.
Reid I, Plank L, Evans M . Fat mass is an important determinant of whole body bone density in premenopausal women but not in men J Clin Endocrinol Metab 1992 75: 779–782.
Cicuttini F, Spector T . Obesity, arthritis, and gout Handbook of Obesity Marcel Dekker: New York 1998, pp 741–752.
Goulding A, Gold E, Cannan R, Taylor R, Williams S, Lewis-Barned N . DEXA supports the use of BMI as a measure of fatness in young girls Int J Obes 1996 20: 1014–1021.
Pietrobelli A, Faith M, Allison D, Gallagher D, Chiumello G, Heymsfield S . Body mass index as a measure of adiposity among children and adolescents: A validation study J Ped 1998 132: 204–210.
Troiano R, Flegal K, Kuczmarski R, Campbell S, Johnson C . Overweight prevalence and trends for children and adolescents Arch Pediatr Adolesc Med 1995 149: 1085–1091.
Dietz W . How to tackle the problem early? The role of education in the prevention of obesity Int J Obes 1999 23 (Suppl 4): S7–S9.
Morris F, Naughton G, Gibbs J, Carlson J, Wark J . Prospective ten-month exercise intervention in premenarcheal girls: positive effect on bone and lean mass J Bone Min Res 1997 12: 1453–1462.
Rizzoli R, Bonjour J-P . Hormones and bones Lancet 1997 349 (Suppl 1): 20–23.
Ferretti J, Capozza R, Cointry G, Garcia S, Plotkin H, Alvarez Filgueira M, Zanchetta J . Gender-related differences in the relationship between densitometric values of whole-body bone mineral content and lean body mass in humans between 2 and 87 years Bone 1998 22: 683–690.
Acknowledgements
This study was supported by the Health Research Council of New Zealand. We thank the participants and their parents for their willing co-operation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Goulding, A., Taylor, R., Jones, I. et al. Overweight and obese children have low bone mass and area for their weight. Int J Obes 24, 627–632 (2000). https://doi.org/10.1038/sj.ijo.0801207
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ijo.0801207
Keywords
This article is cited by
-
Die Rolle von Magnesium bei Knochenbrüchen in übergewichtigen Kindern und Jugendlichen
Journal für Mineralstoffwechsel & Muskuloskelettale Erkrankungen (2021)
-
Dairy product intake decreases bone resorption following a 12-week diet and exercise intervention in overweight and obese adolescent girls
Pediatric Research (2020)
-
Association of adiposity measures in childhood and adulthood with knee cartilage thickness, volume and bone area in young adults
International Journal of Obesity (2019)
-
Effect of cardiometabolic risk factors on the relationship between adiposity and bone mass in girls
International Journal of Obesity (2018)
-
Effects of interventions with a physical activity component on bone health in obese children and adolescents: a systematic review and meta-analysis
Journal of Bone and Mineral Metabolism (2018)
