
Abstract
OBJECTIVE: To describe differences in the 22 y mortality risk associated with body mass index (BMI), body fat or fat-free mass, in order to examine if the differential health consequences of fat and fat-free mass may be responsible for elevated mortality rates at both high and low BMI.
DESIGN: Prospective cohort study, a 22 y follow-up.
SETTING: General community. The study of men born in 1913, Gothenburg.
SUBJECTS: 787 men aged 60 y.
MAIN OUTCOME MEASURES: Number and time of total deaths from 1973 to 1995.
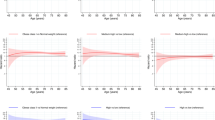
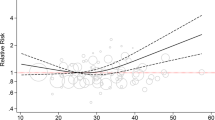
RESULTS: The risk of dying was a linear function of percentage fat and fat-free mass, and increased from a relative risk of 1.00 in men belonging to the lowest fifth to 1.4 (95% confidence interval 1.11–1.99) in men in the highest fifth of percentage fat mass. For BMI the lowest risk was observed for men belonging to the middle fifth of BMI. When the relative risk was set at 1.00 for subjects belonging to the middle fifth of BMI the risk associated with the low BMI fifth was 1.3 (95% confidence interval 0.94–1.68) and that with the highest fifth was 1.5 (95% confidence interval 1.09–1.96). Analyses including both body fat and fat-free mass showed that total mortality was a linear increasing function of high fat and low fat-free mass.
CONCLUSION: The apparent U-shaped association between BMI and total mortality may be the result of compound risk functions from body fat and fat-free mass.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others
References
Seidell JC, Deurenberg P, Hautvast JGAJ . Obesity and fat distribution in relation to health—current insights and recommendations Wld Rev Nutr Diet 1987 50: 57–91.
Yao C-H, Slattery ML, Jacobs DR, Folsom AR, Nelson ET . Anthropometric predictors of coronary heart disease and total mortality: Findings from the US railroad study Am J Epidemiol 1991 134: 1278–1289.
Bengtsson C, Lapidus L, Stendahl C, Waldenstrom J . Hyperuricaemia and risk of cardiovascular disease and overall death. A 12-year follow-up of participants in the population study of women in Gothenburg, Sweden Acta Med Scand 1988 224: 549–555.
US Department of Agriculture, US Department of Health and Human Services . Nutrition and your health: Dietary guidelines for Americans, 3rd edn. US Government Printing Office: Washington, DC, 1990.
US Department of Agriculture, US Department of Health and Human Services . Nutrition and your health: Dietary guidelines for Americans. Homes and Garden Bulletin no. 232). US Government Printing Office: Washington, DC, 1995.
Troiano RP, Frongillo EA, Sobal J, Levitsky DA . The relationship between body weight and mortality: A quantitative analysis of combined information from existing studies Int J Obes 1996 20: 63–75.
Manson JE, Willet WC, Stampfer MJ, Coldtiz GA, Hunter DJ, Hankinson SE, Hennekens CH, Speizer FE . Body weight and mortality among women N Engl J Med 1995 333: 677–685.
Losonczy KG, Harris TB, Cornoni-Huntley J, Simonsick EM, Wallace RB, Cook NR, Ostfeld AM, Blazer DG . Does weight loss from middle age to old age explain the inverse weight mortality relation in old age? Am J Epidemiol 1995 141: 312–321.
Waaler HT . Height, weight and mortality—the Norwegian experience Acta Med Scand 1984 (suppl): 679: 56.
Harris TB, Ballard-Barbasch R, Madan J, Makuc DM, Feldman JJ . Overweight, weight loss, and risk of coronary heart disease in older women. The NHANES I Follow-up Study Am J Epidemiol 1993 137: 1318–1327.
Baumgartner RN, Heymsfield SB, Roche AF . Human body composition and the epidemiology of chronic disease Obes Res 1995 3: 73–95.
Allison DB, Faith MS, Heo M, Kotler DP . Hypothesis concerning the U-shaped relation between body mass index and mortality Am J Epidemiol 1997 146: 339–349.
Svärdsuud K, Tibblin G . A longitudinal study of blood pressure. Change of blood pressure during ten years in relation to individual values. The study of men born in 1913 J Chron Dis 1980 33: 627–633.
Forbes GB, Gallup J, Hurch JB . Estimation of total body fat from potassium-40 content Science 1961 133: 101.
Grimby G, Wilhelmsen L, Björntorp P, Saltin B, Tibblin G . Habitual physical activity. In Saltin B (ed.). Muscle metabolism during exercise. Plenum Press: New York. 1971 469–481.
Royston P, Altman DG . Regression using fractional polynomials of continuous covariates: Parsimonious parametric modelling Appl Statist 1994 43: 429–467.
StataCorp . Stata Statistical Software, Release 4.0, 1995.
VanItallie TB, Yang M-U, Heymsfield SB, Funk RC, Boileau RA . Height-normalized indices of the body's fat-free mass and fat mass: Potentially useful indicators of nutritional status Am J Clin Nutr 1990 52: 953–959.
Segal KR, Dunaif A, Gutin B, Albu J, Nyman A, Pi-Sunyer FX . Body composition, not body weight, is related to cardiovascular disease risk factors and sex hormone levels in men. J Clin Invest 1987 80: 1050–1055.
AIN Healthy Weight Steering Committee . Report of the American Institute of Nutrition (AIN) Steering Committee on Healthy Weight J Nutr 1994 124: 2240–2243.
Lean ME, Han TS, Seidell JC . Impairment of health and quality of life in people with large waist circumference Lancet 1998 351: 853–856.
Larsson B, Svardsudd K, Welin L, Wilhelmsen L, Björntorp P, Tibblin G . Abdominal adipose tissue distribution, obesity, and risk of cardiovascular disease and death: 13 year follow up of participants in the study of men born in 1913 Br Med J 1984 288: 1401–1404.
Sjöström L, Kvist H, Cederblad Å, Tylén U . Determination of total adipose tissue and body fat in women by computed tomography, 40K and tritium Am J Physiol 1986 250: E736–E745.
Heitmann BL . Methods for estimating body fat and fat free mass. In Romsos DR et al (eds). Obesity: Dietary factor and control. Japan Science Society Press: Tokyo/Karger: Basel 1991 227–236.
Acknowledgements
This study was supported by grants from the Swedish Medical Research Council (B98-27X-0626-17), King Gustaf V and Queen Victoria's Foundation, the Gothenburg Medical Association, the Danish National Research Foundation, the Danish Health Insurance Foundation and the Danish Heart Association.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Heitmann, B., Erikson, H., Ellsinger, BM. et al. Mortality associated with body fat, fat-free mass and body mass index among 60-year-old Swedish men—a 22-year follow-up. The study of men born in 1913. Int J Obes 24, 33–37 (2000). https://doi.org/10.1038/sj.ijo.0801082
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ijo.0801082
Keywords
This article is cited by
-
Body fat and risk of all-cause mortality: a systematic review and dose-response meta-analysis of prospective cohort studies
International Journal of Obesity (2022)
-
Interpretable machine learning prediction of all-cause mortality
Communications Medicine (2022)
-
The Effect of Resistance Training in Healthy Adults on Body Fat Percentage, Fat Mass and Visceral Fat: A Systematic Review and Meta-Analysis
Sports Medicine (2022)
-
Weight Loss After Sleeve Gastrectomy: Does Type 2 Diabetes Status Impact Weight and Body Composition Trajectories?
Obesity Surgery (2021)
-
Defining cutoffs to diagnose obesity using the relative fat mass (RFM): Association with mortality in NHANES 1999–2014
International Journal of Obesity (2020)
