
Abstract
Background/objectives:
The objective of this study was to develop approaches to expressing resting energy expenditure (REE) and lean body mass (LM) phenotypes of metabolic disorders in terms of Z-scores relative to their predicted healthy values.
Subjects/methods:
Body composition and REE were measured in 135 healthy participants. Prediction equations for LM and REE were obtained from linear regression and the range of normality by the standard deviation of residuals. Application is demonstrated in patients from three metabolic disorder groups (lipodystrophy, n=7; thyrotoxicosis, n=16; and resistance to thyroid hormone (RTH), n=46) in which altered REE and/or LM were characterised by departure from the predicted healthy values, expressed as a Z-score.
Results:
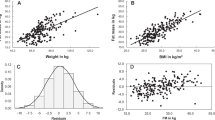
REE (kJ/min)=−0.010 × age (years)+0.016 × FM (kg)+0.054 × fat-free mass (kg)+1.736 (R2=0.732, RSD=0.36 kJ/min).
LM (kg)=5.30 × bone mineral content (kg)+10.66 × height2 (m)+6.40 (male).
LM (kg)=0.20 × fat (kg)+14.08 × height2 (m)−2.93 (female).
(male R2=0.55, RSD=3.90 kg; female R2=0.59, RSD=3.85 kg).
We found average Z-scores for REE and LM of 1.77 kJ/min and −0.17 kg in the RTH group, 5.82 kJ/min and −1.23 kg in the thyrotoxic group and 2.97 kJ/min and 4.20 kg in the LD group.
Conclusion:
This approach enables comparison of data from individuals with metabolic disorders with those of healthy individuals, describing their departure from the healthy mean by a Z-score.
Similar content being viewed by others

Introduction
Many metabolic disorders such as thyroid disease or lipodystrophy (LD) are associated with changes in body composition, energy expenditure or both.1, 2 In describing the phenotypes of such conditions, it is often desirable to describe the extent to which body composition or energy metabolism deviates from that of healthy individuals, but this is not always straight forward. Comparisons against standard predictions of energy expenditure3, 4, 5 may be compromised by atypical body composition, whereas comparisons based on body composition proxies such as body mass index (BMI) may not reveal unusual relationships between fat and lean masses.
Commonly used predictions of resting energy expenditure (REE) may be troublesome owing to their dependence on age and gender, as well as body mass and height.6 Their piecewise linear nature can lead to substantial differences between predicted REE just above and below the intersection of adjacent regression ranges. The use of fat-free mass (FFM=lean body mass (LM)+bone mineral content (BMC) in kg) as a predictor of REE is more accurate and is widely accepted6 and, when allowed an intercept, is disassociated from gender differences in body composition.
Against this background, we have set out an approach to characterise REE and LM in metabolic disorders by reference to measurements in a metabolically healthy cohort. It utilises the accurate and precise measurements of body composition that are now widely available using dual-energy X-ray absorptiometry (DXA).7, 8, 9, 10, 11, 12, 13, 14, 15, 16 The key to our approach has been the description of variability in the difference between measurements and predictions when applied to healthy individuals. This allows us to state with confidence where an individual data point observed in a metabolic disorder lies relative to the healthy range, and so to discuss whether a disorder presents with altered REE or body composition phenotype, or indeed both.
Three conditions (resistance to thyroid hormone (RTH), thyrotoxicosis and LD) in which abnormal energy expenditure and/or increased lean body mass (LM) have been previously documented provide ideal examples to illustrate our method. RTH is a rare genetic condition, with an incidence of 1 in 40 000,17, 18 that is characterised by elevated circulating thyroid hormones (THs) together with central (hypothalamopituitary) and variable peripheral tissue refractoriness to thyroid hormones. More than 90% of affected individuals with RTH have an identified mutation in the THRB gene.19 Thyrotoxicosis (or hyperthyroidism, by which it is known interchangeably) is due to excess TH secretion from the thyroid gland. Most commonly (50–80% of cases), thyrotoxicosis is caused by Graves’ disease, which affects ∼0.5% of the population,20 and is due to autoantibodies causing excess TH production by stimulating the thyroid-stimulating hormone (TSH) receptor in the thyroid gland.21 LD can be either genetic or acquired22 and is characterised by reduced adipocyte storage capacity and loss of adipose tissue with significantly increased LM, contributing to metabolic complications such as insulin resistance and diabetes mellitus.23 We have extensive data in these disorders, which are of particular interest to us, and so have invoked them here for demonstration, although we believe our approach is more generally applicable.
Subjects and methods
Healthy volunteers were recruited by local advertisement in the East Anglian region of the United Kingdom. We recruited 135 male and female non-smokers, aged between 17 and 65 years who had no known medical conditions, were not taking any medications or supplements likely to influence energy expenditure or body composition and who did not normally exercise for over an hour a day. Volunteers were from different ethnic backgrounds (126 Caucasian, 2 Black, 6 Asian, and 1 Hispanic). All participants provided written, informed consent.
Volunteers from the metabolic disorder groups (LD, n=7; thyrotoxicosis, n=16; and RTH, n=46) were recruited following referral to Addenbrooke’s Hospital and provided written informed consent to participation in their studies. Participants were non-smoking, not on any β-blockers or antiarrhythmic treatment and had no current or past history of eating disorder. All patients with RTH had a mutation identified in the THRB gene. Thyrotoxic patients were identified based on thyroid function tests suggestive of thyroxicosis (serum TSH <0.03 mU/l, free thyroxine (T4) >22.5 pmol/l) and had Graves’ disease, as evidenced by elevated anti-TSH receptor antibody titres. Details on the recruitment of the lipodystrophic participants have been documented previously.24
Healthy participants and metabolically disordered participants were asked to refrain from strenuous physical activity, alcohol and caffeine for 24 h before their visit. Each participant arrived at the NIHR/Wellcome Trust Clinical Research Facility in Cambridge at 1400 hours on day 0 and remained until 1200 hours on day 1. After informed consent and medical examination on day 0, height, weight and body composition were measured. Body composition (fat mass, lean mass and bone mineral density) was assessed by DXA (GE Lunar Prodigy GE Healthcare, Madison, WI, USA; software version 12.2). At 1800 hours, a standardised dinner was served. The energy content of the meal was 1/3 of a participant’s daily requirements estimated from predicted resting metabolic rate3 multiplied by an activity factor of 1.35.25 Meal composition was 30–35% fat, 12–15% protein and 50–55% carbohydrate by energy. The participant retired to bed at 2300 hours and was woken the next morning at 0700 hours. REE was measured between 0700 and 0800 hours by ventilated canopy respiratory gas exchange (GEM; GEMNutrition, Daresbury, UK). Measurements were recorded at 30 s intervals over 20 min. The LD participants’ REE was measured by indirect room calorimetry for 60 min and has been described previously.24 All participants were asked to remain awake and still, without any interactions, for the duration of the measurement. Energy expenditure was calculated from the macronutrient respiratory quotients and energy equivalents of oxygen published by Elia and Livesey.26 Following the REE measurement, fasting blood samples were taken for renal and liver function tests, plasma glucose and thyroid function (free triiodothyronine (T3), T4 and TSH). Urinary metanephrines were also measured.
Body composition and REE measurements were performed in all healthy and metabolically disordered volunteers and are summarised in Supplementary Table 1, Table 1 and Table 2.
Ethics
The study received a favourable opinion from the Cambridge Central East of England Research Ethics Committee and was funded by and conducted in the NIHR/Wellcome Trust Clinical Research Facility (WTCRF, Cambridge, UK).
Statistical analysis
Multiple correlation analyses were undertaken using SPSS19 (SPSS Inc., Chicago, IL, USA) to identify variables or combinations of variables that correlate (P<0.05) to REE and DXA-measured total body LM.
Once the correlating variables were established, forward stepwise multiple linear regression analysis was performed to relate REE (kJ/min) to FFM (kg), FM (kg) and age in all subjects and to relate LM to FM and height for female subjects and LM to height and BMC in male subjects.
A K-fold cross-validation approach was then undertaken to test the reliability of both the models. The data set was randomly numbered and split into test data sets and a validation data set. For the REE validation, the analysis was repeated eight times making sure each data point was tested and validated to establish whether the same variables significantly contributed to the prediction of REE, and then the standard deviations of the residuals (the individual differences between predicted and measured values) were compared. For LM cross-validation, the analysis was repeated five times and was also tested on an additional data set of 19 female subjects and 18 male subjects.
Residuals were derived for each contributing data point and normality was confirmed for the set of all residuals using Shapiro–Wilk test for normality. This allowed the distributions of residuals to be described by their standard deviations, the magnitudes of which were taken as a measure of the precision of the prediction. Furthermore, each experimental data point could be defined in terms of the number of standard deviations from the predicted value (Z-score). When investigating the disease groups, REE or LM was predicted as though belonging to the healthy cohort, and an associated Z-score used as a measure of the deviation from the healthy norm.
Results
Resting energy expenditure
To establish the appropriate variables to include in the prediction of REE, we examined the literature and subsequently explored correlations of REE with age, gender, height2, bone mass, FFM and FM.
Analysis of variance was carried out to test the effect of ethnicity (white, black and Asian) on REE and LM, and showed that in this group of volunteers there was no effect of ethnicity on REE or LM (REE, F=0.286, LM, F=0.921). Stepwise multiple regression analysis was carried out to establish which correlates contributed significantly to the prediction of REE and LM. Those that did not contribute were excluded (Table 3).
The variables that contributed the least to the prediction of REE were gender (R2=0.004), height2 (R2=0.005) and bone mass (R2=0.002). With these removed, age continued to contribute to the overall prediction leaving FM (R2=0.043), FFM (R2=0.660) and age (R2=0.018) in the regression (R2=0.732). The resulting expression derived from the 135 healthy participants is

REE regression validation
The regression expression for REE above has been subject to K-fold validation. The source data was randomised into eight groups and regressions repeatedly derived from 7 × 17 and 1 × 16 subjects and tested in the remaining group. The coefficients of variation for the resulting eight estimates of each regression coefficient were: age 7.3%, FM 12.1%, FFM 2.9% and constant 4.9%. The standard deviation of residuals in the test group for the eight regressions ranged from 0.27 to 0.49 kJ/min compared with 0.36 kJ/min for the whole data set.
Lean mass
The least significant coefficient, age (P>0.05), was taken out of the analysis first. Once this had been removed fat and height2 were highly significant contributors in female subjects but height2 alone was significant in male subjects. Bone mass was a significant contributor to LM in male subjects when it replaced FM but this was not the case in female subjects. Therefore, the two gender-specific regression equations for the prediction of LM are as follows:
Male LM (kg) (n=47)=5.30 × bone mass (kg)+10.66 × height2 (m)+6.40
Female LM (kg) (n=88)=0.20 × fat (kg)+14.08 × height2 (m)−2.94
The standard deviations of residuals for these two regressions are, respectively, 3.90 and 3.85 kg.
Lean mass regression validation
As with the REE validation process, the male and female lean mass regressions have undergone K-fold validation, randomised into five groups and the analysis repeated five times. The female results indicated that the standard deviation of residuals ranged from 3.0 to 4.26 kg compared with 3.85 kg from the whole data set. The male results indicated a range of 2.38–4.83 kg compared with 3.90 kg from the whole data set. The data were also tested in independent male and female data sets drawn from the entire control group of another study and its ongoing successor (n=18 males and 19 females). For the male group, the mean residual in the test group is −1.49 kg with s.d. 3.91 kg. The offset of the male mean from zero is predominantly due to a single outlier whose residual was double that of any other subject, yet is not significantly different from zero. For the female group, the mean residual is 0.15 kg (NS) with s.d. 2.2 kg.
Representation of data: Z-scores
Resting energy expenditure
To represent the normative data, the residuals of measured REE−predicted REE were plotted with corresponding Z-scores (Figure 1). LM, the strongest predictive variable, is used to separate the data points. To assess the utility of this approach in disorder states known to be associated with altered body composition and resting metabolic rate, we characterised patients with RTH, thyrotoxicosis and LD.1, 27 When data from patients with metabolic disorders is represented alongside the healthy volunteer data, clear differences between health and the disorder states emerge (Figure 2). As expected, all the metabolic disease groups manifest elevated REE (mean Z RTH: 1.77; LD: 2.97) with the thyrotoxicosis group having the highest REE values with a mean Z-score of 5.8 and a range from 1.5 to 9.6.

Measured−predicted REE (kJ/min) in healthy controls with 2 s.d.

Differences between measured and predicted REE and LM in metabolic disorders and the healthy cohort.
Lean mass
Supplementary Figure 1 shows the variability in LM within the metabolically healthy male and female subjects. The residuals of the difference between measured and predicted LM are again presented together with Z-scores. Height was used to separate the points. Figure 2 also demonstrates how metabolic disorders may be characterised by comparison with healthy subject data. The differences between LM in thyrotoxicosis and RTH can be compared with that of the healthy cohort (mean Z thyrotoxic: −1.23; RTH: −0.17). The LD data (mean Z: 4.20) illustrates the substantial excess of lean tissue present in this disorder.
LM and REE Z-scores may be plotted orthogonally, where they combine to offer a succinct insight into the phenotypes of metabolic disorders. Figure 3 illustrates the relationship between changes in REE and LM in metabolic disorders compared with the healthy group. The lipodystrophic group are characterised by elevated LM and elevated REE with Z-scores ranging from 2.2 to 7.3 Z for LM and 1.4 to 4.8 Z for REE. The thyrotoxicosis group also manifest elevated REE (1.5–9.6 Z) but, in contrast to the LD group, have reduced LM (mean Z=−1.2).

Combination of LM and REE Z-scores to illustrate the contribution to metabolic disorders. The circle indicates a Z-score of ±2 for REE and LM.
Discussion
The aim of this work was to develop approaches to the description of metabolic phenotypes in terms of the distribution of REE and LM in metabolically healthy people. The novelty of our approach lies in the way in which metabolic and body composition data is represented. Subtracting a predicted value from measured values produces a residual; and dividing this by the standard deviation of residuals in a healthy cohort, we can assign a Z-score. Z-scores are commonly used in the analysis of bone densitometry28 and on growth charts to highlight individuals whose results deviate from the population average.29 Here, we commend the use of Z-scores to highlight individuals and groups of patients with abnormal metabolic rates and/or abnormal LM.
Body composition measurements
The body composition measurements on which this paper relies were undertaken by DXA. This is a widely available technique that is able to provide quick and well-tolerated estimates of body composition supported by reports of good accuracy and precision.7 However, it is important to consider whether any disorder to which our proposed methodology is applied might generate a bias in the DXA measurements relative to the healthy population. The work of Williams et al.30 offers valuable context for this consideration. In the case of our example disorder groups, we do not believe bias in DXA estimates to have been a concern. Body composition data in our most extreme phenotype, LD, was corroborated by air displacement plethysmography measurements.31
Resting energy expenditure
The results from the REE multiple regression analysis in this study demonstrate a model that predicts REE accurately and with good precision in healthy individuals. The variables that contribute to our predictive equation are FFM, FM and age. These have previously been documented as appropriate covariates.6, 32, 33, 34 FFM is recognised as the main predictor of the interindividual variability in resting energy expenditure. The relationship between FFM and REE differs between men and women when constrained through the origin, as is implicit when REE is expressed per unit FFM. However, in preparing this work, we have confirmed that when an intercept is allowed, men and women tend to fall on the same regression line. Moreover, the relationship between REE and FFM is strengthened and therefore allows one regression equation for both genders. There is, however, conflicting literature regarding the contribution of FM to energy expenditure. In a review, Cunningham6 suggested that FM contributes to energy expenditure in women, but mostly in obese women. Our study found that FM explained 4.0% of the variance in energy expenditure and when the analysis was broken down by gender there was no significant difference in the variance explained by FM between male and female subjects, even though we had a greater number of female subjects in the cohort. The most commonly used predictive equations for estimating energy expenditure in a clinical setting are Schofield and Henry.3, 5 They include simple measurements such as height and weight, age and gender, regardless of literature that disputes their accuracy and precision, especially when applied to individuals outside the original data sets.35, 36 Weijs et al.37 performed a meta-analysis of common REE prediction equations on 48 outpatients and 45 in-patients with conditions including anorexia, overweight, thyroid disease and inflammatory bowel disease, all of which have body compositions and energy expenditures differing from healthy controls.38, 39, 40, 41, 42 They saw errors ranging from 975 to 1782 kJ per day, with at most only 40% of in-patients having an accurately predicted REE when compared with measured REE. Johnstone et al.43 demonstrated an average increase in accuracy of 32.9% (240 kJ per day) when including body composition (FFM and FM) and anthropometric measurements (skinfold thickness and circumference) compared with the Schofield equation.3
FFM and FM may explain between 60 and 85% of the variance in REE,6 leaving at least 15% unaccounted for. Our results demonstrated that FFM and FM combined account for 70%, leaving 30% unexplained. Age, gender, ethnicity and physical activity have been reported to contribute to this variance.33 In our study, we found a significant but small contribution of age to the prediction of REE (2%). Nielsen et al.32 investigated whether adjusting FFM for extracellular fluid would improve the prediction of REE, but found that this was not the case. Johnstone et al.44 investigated the influence of FFM, FM, age, T4, T3 and leptin levels on REE. They concluded that REE was not influenced by age, gender, leptin or T3, although in men 25% of the variance was associated with circulating T4 levels.
Lean mass
Predictions of FFM or LM are less frequently documented. Previous publications predicting LM have used bioelectrical impedance and skinfold thickness with DXA acting as the reference measurement.45 The variables chosen for the LM prediction equation in the current study were height2 and FM for the female group and height2 and bone mass for the male group. The presence of height2 in the equation reflects the fat and FFM index concept,46, 47 which recognises a relationship between body composition and in body size and offers the prospect of discrimination between health and individuals with abnormal fat or FFM for their size.
Cross-validation
To test our prediction equations, we performed an observational analysis of the coefficients from published studies that have also used FM, FFM and age as variables for prediction of REE (Supplementary Table 2). Supplementary Table 2 suggests that our coefficients for FFM, FM and age are similar to those published previously.6, 32, 48, 49, 50 Of this published work, only Nielson’s32 used DXA for composition measurement; Horrie used bioimpedance,49 whereas Nelson et al.’s48 and Cunningham’s6 papers were based on data previously published by others. When applied to the current data set, the Nielsen equations produced a residual standard deviation of 0.37 compared with 0.36 produced by our equation. In the light of this sparsity of robust comparative data, we performed a K-fold cross-validation analysis on REE and LM models to test their reliability. Comparison of means and standard deviations of residuals in these test groups with those of the training groups suggests that the regressions may be applied beyond the training group with some confidence, although we accept that testing in a larger group would increase this confidence. We would encourage readers who would like to apply our approaches to derive and publish prediction regressions from their own reference cohorts until such time as the published coefficients have converged to a closer consensus than we have presented in Supplementary Table 2—perhaps when published predictions agree to within 1 pooled standard deviation of their residuals.
Application examples
Thyroid disorders
Thyroid conditions such as thyrotoxicosis and RTH result in altered body composition and a raised energy expenditure. Mitchell et al.40 showed that REE is raised in RTH and markedly elevated in thyrotoxic patients. In both conditions there was a higher fat-to-lean mass ratio compared with the healthy controls, although the data suggest that in thyroid disorders the dominant abnormality lies in REE rather than body composition. Our results from the lean mass regression equation suggest that the thyrotoxic group have reduced LM (Z=−1.23), whereas the RTH group have normal LM (Z=−0.17) despite the increased REE.
Our results confirm that REE is higher in a cohort of RTH subjects compared with healthy controls; however, in patients with thyrotoxicosis, the magnitude of elevation in REE is more substantial. In RTH, predominant expression of defective thyroid receptor-β in the hypothalamus and pituitary mediates resistance to hormone action within the pituitary–thyroid feedback axis, resulting in elevated levels of circulating free T4 and T3 with normal or increased levels of TSH.51 Energy expenditure is raised as some peripheral tissues (e.g. myocardium, skeletal muscle) that express normal thyroid receptor-α retain sensitivity to elevated levels of TH.40 In contrast, both β- and α-receptor-mediated signalling is intact in conventional thyrotoxicosis, with preserved responsiveness of tissues to elevated TH, resulting in markedly increased energy expenditure, despite a reduction in LM.52
Lipodystrophy
Lipodystrophic subjects are characterised by an elevated REE and LM.24 Importantly, this is not simply a result of a relative reduction in fat mass, which is present in all of these patients, but appears to be a true increase in lean mass. Although organomegaly and pseudoacromegaly are features of LD (particularly the generalised form),22 the increased lean mass probably reflects contributions from several tissues. Organ tissue will have some contribution to the estimation of lean mass, although it has a relatively small mass of approximately 4.4 kg,34 whereas skeletal muscle mass is almost certainly the largest contributing tissue. We show a mean residual increase of lean mass of 16 kg (Z-score>4) relative to our healthy cohort, suggesting an increase in lean mass over an above that expected through organ contribution. Savage et al.24 investigated the increase in REE in the lipodystrophic participants and concluded that the increase in lean mass in LD patients accounted for their elevated REE. When REE was presented per kg of LM, there was no significant difference between REE in lipodystrophics and healthy matched controls. However, this picture changes when the relationship between REE and LM is allowed an intercept, and changes further when fat mass contributes to the model. We have found an elevation in REE with a Z-score averaging 2 (range 1.4–4.8 kJ/min) relative to our healthy controls (Figure 2). As our prediction of REE takes into account the influence of measured FFM, our approach arguably removes any coupling between departures from the norm in REE and FFM, so our Z-scores are effectively independent. In doing so, it suggests that there may be a component of the elevation in REE in LD beyond that which is associated with FFM alone.
As mentioned in the methods, the lipodystrophic participants had REE measured by room calorimetry rather than the ventilated canopy measurement. In the light of this, we investigated the difference between measurements made using the canopy compared with room calorimetry, on a separate cohort. The results indicated a difference of 0.20 kJ/min between the two methods, suggesting that even after accounting for this difference in measurement the lipodystrophic participants would still display an REE Z-score >2 (mean Z: 2.98 kJ/min).
In summary, we offer expressions for REE and LM in health based on FM, FFM, BMC, age and height2 measurements. Measurements from individuals with uncommon metabolic disorders were examined in the context of data from healthy subjects and differences to be expressed as a Z-score. This facilitates the representation and differentiation of disease phenotypes. This approach may also aid in the characterisation and potentially evaluation of the treatment in such individuals. Further validation of our regressions on a separate cohort of healthy individuals is desirable, but we believe the Z-score approach to metabolic phenotype description will prove valuable and illuminating in these and other metabolic disorders.
References
Savage DB, Semple RK, Clatworthy MR, Lyons PA, Morgan BP, Cochran EK et al. Complement abnormalities in acquired lipodystrophy revisited. J Clin Endocrinol Metab 2009; 94: 10–16.
Psota T, Chen KY . Measuring energy expenditure in clinical populations: rewards and challenges. Eur J Clin Nutr 2013; 67: 436–442.
Schofield WN . Predicting basal metabolic rate, new standards and review of previous work. Hum Nutr Clin Nutr 1985; 39 (Suppl 1), 5–41.
Harris JA, Benedict FG . A biometric study of human basal metabolism. Proc Natl Acad Sci USA 1918; 4: 370–373.
Henry CJ . Basal metabolic rate studies in humans: measurement and development of new equations. Public Health Nutr 2005; 8: 1133–1152.
Cunningham JJ . Body composition as a determinant of energy expenditure: a synthetic review and a proposed general prediction equation. Am J Clin Nutr 1991; 54: 963–969.
Withers RT, LaForgia J, Pillans RK, Shipp NJ, Chatterton BE, Schultz CG et al. Comparisons of two-, three-, and four-compartment models of body composition analysis in men and women. J Appl Physiol 1998; 85: 238–245.
Cordero-MacIntyre ZR, Peters W, Libanati CR, Espana RC, Abila SO, Howell WH et al. Reproducibility of DXA in obese women. J Clin Densitometry 2002; 5: 35–44.
Genton L, Karsegard VL, Zawadynski S, Kyle UG, Pichard C, Golay A et al. Comparison of body weight and composition measured by two different dual energy X-ray absorptiometry devices and three acquisition modes in obese women. Clin Nutr 2006; 25: 428–437.
Arngrimsson S, Evans EM, Saunders MJ, Ogburn CL III, Lewis RD, Cureton KJ . Validation of body composition estimates in male and female distance runners using estimates from a four-component model. Am J Hum Biol 2000; 12: 301–314.
Chen Z, Wang Z, Lohman T, Heymsfield SB, Outwater E, Nicholas JS et al. Dual-energy X-ray absorptiometry is a valid tool for assessing skeletal muscle mass in older women. J Nutr 2007; 137: 2775–2780.
Deurenberg-Yap M, Schmidt G, van Staveren WA, Hautvast JG, Deurenberg P . Body fat measurement among Singaporean Chinese, Malays and Indians: a comparative study using a four-compartment model and different two-compartment models. Br J Nutr 2001; 85: 491–498.
Goran MI, Toth MJ, Poehlman ET . Assessment of research-based body composition techniques in healthy elderly men and women using the 4-compartment model as a criterion method. Int J Obes Relat Metab Disord 1998; 22: 135–142.
Van Der Ploeg GE, Withers RT, Laforgia J . Percent body fat via DEXA: comparison with a four-compartment model. J Appl Physiol 2003; 94: 499–506.
Visser M, Fuerst T, Lang T, Salamone L, Harris TB . Validity of fan-beam dual-energy X-ray absorptiometry for measuring fat-free mass and leg muscle mass. Health, Aging, and Body Composition Study—Dual-Energy X-ray Absorptiometry and Body Composition Working Group. J Appl Physiol 1999; 87: 1513–1520.
Silva AM, Heymsfield SB, Sardinha LB . Assessing body composition in taller or broader individuals using dual-energy X-ray absorptiometry: a systematic review. Eur J Clin Nutr 2013; 67: 1012–1021.
Lafranchi SH, Snyder DB, Sesser DE, Skeels MR, Singh N, Brent GA et al. Follow-up of newborns with elevated screening T4 concentrations. J Pediatr 2003; 143: 296–301.
Chiesa A, Olcese MC, Papendieck P, Martinez A, Vieites A, Bengolea S et al. Variable clinical presentation and outcome in pediatric patients with resistance to thyroid hormone (RTH). Endocrine 2012; 41: 130–137.
Weiss RE, Refetoff S . Resistance to thyroid hormone. Rev Endocr Metab Disord 2000; 1: 97–108.
Brent GA . Clinical practice. Graves’ disease. N Engl J Med 2008; 358: 2594–2605.
Weetman AP . Graves’ disease. N Engl J Med 2000; 343: 1236–1248.
Garg A . Clinical review#: Lipodystrophies: genetic and acquired body fat disorders. J Clin Endocrinol Metab 2011; 96: 3313–3325.
Simha V, Garg A . Lipodystrophy: lessons in lipid and energy metabolism. Curr Opin Lipidol 2006; 17: 162–169.
Savage DB, Murgatroyd PR, Chatterjee VK, O'Rahilly S . Energy expenditure and adaptive responses to an acute hypercaloric fat load in humans with lipodystrophy. J Clin Endocrinol Metab 2005; 90: 1446–1452.
Westerterp KR . Obesity and physical activity. Int J Obes Relat Metab Disord 1999; 23 (Suppl 1), 59–64.
Elia M, Livesey G . Energy expenditure and fuel selection in biological systems: the theory and practice of calculations based on indirect calorimetry and tracer methods. World Rev Nutr Diet 1992; 70: 68–131.
Chatterjee VKK . Resistance to thyroid hormone. Hormone Res 1997; 48: 43–46.
Ellis KJ, Shypailo RJ, Hardin DS, Perez MD, Motil KJ, Wong WW et al. Z score prediction model for assessment of bone mineral content in pediatric diseases. J Bone Miner Res 2001; 16: 1658–1664.
Ogden CL, Kuczmarski RJ, Flegal KM, Mei Z, Guo S, Wei R et al. Centers for Disease Control and Prevention 2000 Growth Charts for the United States: Improvements to the 1977 National Center for Health Statistics Version. Pediatrics 2002; 109: 45–60.
Williams JE, Wells JC, Wilson CM, Haroun D, Lucas A, Fewtrell MS . Evaluation of Lunar Prodigy dual-energy X-ray absorptiometry for assessing body composition in healthy persons and patients by comparison with the criterion 4-component model. Am J Clin Nutr 2006; 83: 1047–1054.
Fields DA, Goran MI, McCrory MA . Body-composition assessment via air-displacement plethysmography in adults and children: a review. Am J Clin Nutr 2002; 75: 453–467.
Nielsen S, Hensrud DD, Romanski S, Levine JA, Burguera B, Jensen MD . Body composition and resting energy expenditure in humans: role of fat, fat-free mass and extracellular fluid. Int J Obes Relat Metab Disord 2000; 24: 1153–1157.
Ravussin E, Bogardus C . Relationship of genetics, age, and physical fitness to daily energy expenditure and fuel utilization. Am J Clin Nutr 1989; 49 (Suppl), 968–975.
Hunter GR, Weinsier RL, Gower BA, Wetzstein C . Age-related decrease in resting energy expenditure in sedentary white women: effects of regional differences in lean and fat mass. Am J Clin Nutr 2001; 73: 333–337.
Horgan GW, Stubbs J . Predicting basal metabolic rate in the obese is difficult. Eur J Clin Nutr 2003; 57: 335–340.
Scalfi L, Marra M, De Filippo E, Caso G, Pasanisi F, Contaldo F . The prediction of basal metabolic rate in female patients with anorexia nervosa. Int J Obes Relat Metab Disord 2001; 25: 359–364.
Weijs PJ, Kruizenga HM, van Dijk AE, van der Meij BS, Langius JA, Knol DL et al. Validation of predictive equations for resting energy expenditure in adult outpatients and inpatients. Clin Nutr 2008; 27: 150–157.
El Ghoch M, Alberti M, Capelli C, Calugi S, Dalle Grave R . Resting energy expenditure in anorexia nervosa: measured versus estimated. J Nutr Metab 2012; 2012: 652932.
Sasaki M, Johtatsu T, Kurihara M, Iwakawa H, Tanaka T, Bamba S et al. Energy expenditure in Japanese patients with severe or moderate ulcerative colitis. J Clin Biochem Nutr 2010; 47: 32–36.
Mitchell CS, Savage DB, Dufour S, Schoenmakers N, Murgatroyd P, Befroy D et al. Resistance to thyroid hormone is associated with raised energy expenditure, muscle mitochondrial uncoupling, and hyperphagia. J Clin Invest 2010; 120: 1345–1354.
Herwig A, Ross AW, Nilaweera KN, Morgan PJ, Barrett P . Hypothalamic thyroid hormone in energy balance regulation. Obes Facts 2008; 1: 71–79.
Ahmad A, Duerksen DR, Munroe S, Bistrian BR . An evaluation of resting energy expenditure in hospitalized, severely underweight patients. Nutrition 1999; 15: 384–388.
Johnstone AM, Rance KA, Murison SD, Duncan JS, Speakman JR . Additional anthropometric measures may improve the predictability of basal metabolic rate in adult subjects. Eur J Clin Nutr 2006; 60: 1437–1444.
Johnstone AM, Murison SD, Duncan JS, Rance KA, Speakman JR . Factors influencing variation in basal metabolic rate include fat-free mass, fat mass, age, and circulating thyroxine but not sex, circulating leptin, or triiodothyronine. Am J Clin Nutr 2005; 82: 941–948.
Stewart AD, Hannan WJ . Prediction of fat and fat-free mass in male athletes using dual X-ray absorptiometry as the reference method. J Sports Sci 2000; 18: 263–274.
Dulloo AG, Jacquet J, Solinas G, Montani JP, Schutz Y . Body composition phenotypes in pathways to obesity and the metabolic syndrome. Int J Obes (Lond) 2010; 34 (Suppl 2), S4–S17.
VanItallie TB, Yang MU, Heymsfield SB, Funk RC, Boileau RA . Height-normalized indices of the body’s fat-free mass and fat mass: potentially useful indicators of nutritional status. Am J Clin Nutr 1990; 52: 953–959.
Nelson KM, Weinsier RL, Long CL, Schutz Y . Prediction of resting energy expenditure from fat-free mass and fat mass. Am J Clin Nutr 1992; 56: 848–856.
Horie LM, Gonzalez MC, Torrinhas RS, Cecconello I, Waitzberg DL . New specific equation to estimate resting energy expenditure in severely obese patients. Obesity (Silver Spring, MD) 2011; 19: 1090–1094.
Cunningham JJ . A reanalysis of the factors influencing basal metabolic rate in normal adults. Am J Clin Nutr 1980; 33: 2372–2374.
Chatterjee VK, Nagaya T, Madison LD, Datta S, Rentoumis A, Jameson JL . Thyroid hormone resistance syndrome. Inhibition of normal receptor function by mutant thyroid hormone receptors. J Clin Invest 1991; 87: 1977–1984.
Acotto CG, Niepomniszcze H, Mautalen CA . Estimating body fat and lean tissue distribution in hyperthyroidism by dual-energy X-ray absorptiometry. J Clin Densitometry 2002; 5: 305–311.
Acknowledgements
We thank Elizabeth Blower for assistance in data collection, and all the staff of the NIHR/Wellcome Trust Clinical Research Facility Cambridge for their assistance with the clinical studies. We particularly thank the volunteers who contributed their time and measurements to our research. This study was supported by the NIHR/Wellcome Trust Clinical Research Facility. DBS (078986/Z/06/Z), VKC (095564/Z/11/Z) and NS (100585/Z/12/Z) are supported by the Wellcome Trust, the Medical Research Council Centre for Obesity and Related Disorders, NIHR Cambridge Biomedical Research Centre. LB is supported by the UK Medical Research Council programme number MC_UP_A090_1005.
Author contributions
The authors’ responsibilities were as follows: LW—conducted research, analysed data and performed statistical analysis, drafted of manuscript, primary responsibility for the final content; PRB—conducted research, statistical analysis, revision of the manuscript and important intellectual contributions; CM, NS, CM, LB, DBS—critical revision of the manuscript and important intellectual contributions, KC—critical revision of the manuscript, important intellectual contributions and supervision; and PRM—study concept and design, critical revision of the manuscript, important intellectual contributions, analysis and interpretation. All authors read and approved the final manuscript. LB’s contribution formed part of the Medical Research Council programme number SPT60.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on European Journal of Clinical Nutrition website
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Watson, L., Raymond-Barker, P., Moran, C. et al. An approach to quantifying abnormalities in energy expenditure and lean mass in metabolic disease. Eur J Clin Nutr 68, 234–240 (2014). https://doi.org/10.1038/ejcn.2013.237
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejcn.2013.237
Keywords
This article is cited by
-
Resistance to thyroid hormone induced tachycardia in RTHα syndrome
Nature Communications (2023)
-
Estimating physical activity from self-reported behaviours in large-scale population studies using network harmonisation: findings from UK Biobank and associations with disease outcomes
International Journal of Behavioral Nutrition and Physical Activity (2020)
-
Estimating energy expenditure from wrist and thigh accelerometry in free-living adults: a doubly labelled water study
International Journal of Obesity (2019)
-
Normalizing resting energy expenditure across the life course in humans: challenges and hopes
European Journal of Clinical Nutrition (2018)
