
Abstract
Objective: To analyze the impact of choosing the left or the right side of the body on the anthropometric measurements and derived nutritional indices, in prepubertal children.
Design: Cross-sectional pilot nutrition survey.
Setting: General prepubertal school-age population.
Subjects: One-hundred and sixty-four children (97 boys and 67 girls) aged 7–9 y.
Interventions: None.
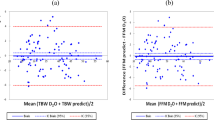
Results: The agreement between anthropometric measurements in both sides of the body showed that in males and in females, suprailiac skinfold thickness and arm circumference were significantly higher in the left than in the right side of the body. The agreement between body composition assessed by anthropometric measurements in both sides of the body showed that only in males was arm muscle area significantly higher in the left than in the right side, and arm fat percentage was higher in the right than in the left side of the body. Total body fat percentage calculated from skinfold thickness did not show statistically significant differences when skinfolds were obtained in the both sides of the body, either in boys and in girls.
Conclusions: Our results show that differences between the sides of the body were lower than the technical error of measurement of the anthropometric measurements obtained and seem not to be biologically significant in this age group. It is necessary to standardize the method of anthropometric assessment of the nutritional status in terms of body side.
Sponsorship: Universidad de Zaragoza (216-17).
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others


References
Barker M, Robinson S, Osmond C, Barker DJP . 1997 Birth weight and body fat distribution in adolescent girls Arch. Dis. Child. 77: 381–383
Bland JM, Altman DG . 1986 Statistical methods for assessing agreement between two methods of clinical measurement Lancet 8: 307–310
Brook CGD . 1971 Determination of body composition of children from skinfold measurements Arch. Dis. Child. 46: 182–184
Burgert SL, Anderson CF . 1979 An evaluation of upper arm measurements used in nutritional assessment Am. J. Clin. Nutr. 32: 2136–2142
Deurenberg P, Pieters JJL, Hauvast JGAJ . 1990 The assessment of the body fat percentage by skinfold thickness measurements in childhood and young adolescence Br. J. Nutr. 63: 293–303
Deurenberg P, Deurenberg Yap M, Wang J, Lin FP, Schmidt G . 1999 The impact of body build on the relationship between body mass index and percent body fat Int. J. Obes. Relat. Metab. Disord. 23: 537–542
Eliakim A, Burke GS, Cooper DM . 1997 Fitness, fatness, and the effect of training assessed by magnetic resonance imaging and skinfold-thickness measurements in healthy adolescent females Am. J. Clin. Nutr. 66: 223–231
Gerver WJM, de Bruin R . 1996 Body composition in children based on anthropometric data. A presentation of normal values Eur. J. Pediatr. 155: 870–876
Goran MI, Gower BA, Treuth M, Nagy TR . 1998 Prediction of intra-abdominal and subcutaneous abdominal adipose tissue in healthy prepubertal children Int. J. Obes. Relat. Metab. Disord. 22: 549–558
Gurrici S, Hartriyanti Y, Hautvast JGAJ, Deurenberg P . 1998 Relationship between body fat and body mass index: differences between Indonesians and Dutch Caucasians Eur. J. Clin. Nutr. 52: 779–783
Jellife DB . 1966 The assessment of the nutritional status of the community Geneva: World Health Organization
Johnston JL, Leong MS, Checkland EG, Zuberbuhler PC, Conger PR, Quinney HA . 1988 Body fat assessed from body density and estimated from skinfold thickness in normal children and children with cystic fibrosis Am. J. Clin. Nutr. 48: 1362–1366
Katzmarzyk PT, Pérusse L, Malina RM, Bouchard C . 1999 Seven-year stability of indicators of obesity and adipose tissue distribution in the Canadian population Am. J. Clin. Nutr. 69: 1123–1129
Lean MEJ, Han TS, Deurenberg P . 1996 Predicting body composition by densitometry from simple anthropometric measurements Am. J. Clin. Nutr. 63: 4–14
Moreno LA, Fleta J, Mur L, Feja C, Sarría A, Bueno M . 1997 Indices of body fat distribution in Spanish children aged 4.0 to 14.9 y J. Pediatr. Gastroenterol. Nutr. 25: 175–181
Moreno LA, Fleta J, Mur L, Sarría A, Bueno M . 1998 Fat distribution in obese and nonobese children and adolescents J. Pediatr. Gastroenterol. Nutr. 27: 176–180
Moreno LA, Fleta J, Mur L, Rodríguez G, Sarría A, Bueno M . 1999 Waist circumference values in Spanish children—gender-related differences Eur. J. Clin. Nutr. 53: 429–433
Moreno LA, Fleta J, Sarría A, Rodríguez G, Gil C, Bueno M . 2001a Secular changes in body fat patterning in children and adolescents of Zaragoza (Spain), 1980–1995 Int. J. Obes. Relat. Metab. Disord. 125: 1656–1660
Moreno LA, Fleta J, Sarría A, Rodriguez G, Bueno M . 2001b Secular increases in body fat percentage in male children of Zaragoza (Spain), 1980–1995 Prev. Med. 33: 357–363
Must A, Dallal GE, Dietz WH . 1991 Reference data for obesity: 85th and 95th percentiles of body mass index (wt/ht2) and triceps skinfold thickness Am. J. Clin. Nutr. 53: 839–846
Paul AA, Cole TJ, Ahmed EA, Whitehead RG . 1998 The need for revised standards for skinfold thickness in infancy Arch. Dis. Child. 78: 354–358
Peters D, Fox K, Armstrong N, Sharpe P, Bell M . 1994 Estimation of body fat and body fat distribution in 11-year-old children using magnetic resonance imaging and hydrostatic weighing, skinfolds, and anthropometry Am. J. Hum. Biol. 6: 237–243
Rolland-Cachera MF, Brambilla P, Manzoni P, Akrout M, Sironi S, Del Maschio A, Chiumello G . 1997 Body composition assessed on the basis of arm circumference and triceps skinfold thickness: a new index validated in children by magnetic resonance imaging Am. J. Clin. Nutr. 65: 1709–1713
Sangi H, Mueller WH . 1991 Which measure of body fat distribution is best for epidemiologic research among adolescents? Am. J. Epidemiol. 133: 870–883
Schell LM, Johnston FE, Smith DR, Paolone AM . 1985 Directional asymmetry of body dimensions among white adolescents Am. J. Phys. Anthropol. 67: 317–322
Tanner JM, Whitehouse RH . 1962 Standards for subcutaneous fat in British children. Percentiles for thickness of skinfolds over triceps and below scapula Br. Med. J. 1: 446–450
Tanner JM, Whitehouse RH . 1975 Revised standards for triceps and subscapular skinfolds in British children Arch. Dis. Child. 50: 142–145
Wang J, Thornton JC, Kolesnik S, Pierson RN . 2000 Anthropometry in body composition. An overview Ann. NY Acad. Sci. 904: 317–326
Weststrate JA, Deurenberg P . 1989 Body composition in children: proposal for a method for calculating body fat percentage from total body density or skinfold-thickness measurements Am. J. Clin. Nutr. 50: 1104–1115
Weststrate JA, Deurenberg P, van Tinteren H . 1989 Indices of body fat distribution and adiposity in Dutch children from birth to 18 y of age Int. J. Obes. 13: 465–477
Acknowledgements
This work was supported by grant 216-17 from Universidad de Zaragoza, Zaragoza (Spain).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Moreno, L., Rodríguez, G., Guillén, J. et al. Anthropometric measurements in both sides of the body in the assessment of nutritional status in prepubertal children. Eur J Clin Nutr 56, 1208–1215 (2002). https://doi.org/10.1038/sj.ejcn.1601493
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejcn.1601493
Keywords
This article is cited by
-
Equations based on anthropometric measurements for adipose tissue, body fat, or body density prediction in children and adolescents: a scoping review
Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity (2022)
-
The association between maternal dietary micronutrient intake and neonatal anthropometry – secondary analysis from the ROLO study
Nutrition Journal (2015)
-
Inflammation profile in overweight/obese adolescents in Europe: an analysis in relation to iron status
European Journal of Clinical Nutrition (2015)
-
Methodologies to assess paediatric adiposity
Irish Journal of Medical Science (1971 -) (2015)
-
Reliability and Intermethod Agreement for Body Fat Assessment Among Two Field and Two Laboratory Methods in Adolescents
Obesity (2012)
