
Abstract
Objective: To outline the difficulties and suggest potential solutions in anthropometric assessment of adolescents during humanitarian emergencies.
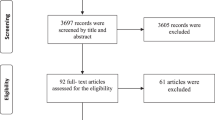
Design: Literature review.
Setting: Multiple settings in which the nutritional status of adolescents has been assessed using anthropometric measurements.
Subjects: Adolescents in multiple populations.
Interventions: None.
Results: The use of anthropometry may be more difficult in adolescents than in other age groups because anthropometric indices in normally nourished adolescents change with age and sexual development. Moreover, survey and reference populations may differ in the age at which certain pubertal landmarks are attained, requiring adjustment for differences between survey and reference populations. Adolescent populations may also differ by ethnicity in various body proportions that affect anthropometric indices. Adjustment may be required when the body proportions of adolescents in the reference population differ from those in the population assessed.
Conclusions: Although no definitive recommendation can be made regarding which anthropometric indices are the most appropriate for adolescents, some revisions may improve current practices. Weight-for-height could be used for prepubertal adolescents and body mass index could be used for postpubertal adolescents. Because cut-off points are age-specific, age should be collected as accurately as possible for all adolescents measured during screening or survey activities. The WHO-recommended reference population of US adolescents is inappropriate in most populations of adolescents. Adolescents should never undergo nutritional assessment in isolation; other population subgroups should be included, and other health, nutrition and food data should be collected at the same time.
Sponsorship: The United Nations Administrative Committee on Coordination/Sub-Committee on Nutrition.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
ACC/SCN. 1992 Second report on the world nutritition situation: volume I, global and regional results Geneva: Administrative Committee on Coordination–Subcommittee on Nutrition
ACC/SCN. 2000 Fourth report on the world nutrition situation: nutrition throughout the life cycle Geneva: United Nations Administrative Committee on Coordination–Subcommittee on Nutrition
Ahmed F, Zareen M, Khan MR, Banu CP, Haq MN, Jackson AA . 1998 Dietary patterns, nutrient intake and growth of adolescent school girls in urban Bangladesh Pub. Health Nutr. 1: 83–92
Benefice E, Fouere T, Malina RM . 1999 Early nutritional history and motor performance of Senegalese children, 4–6 y of age Ann. Hum. Biol. 26: 443–455
Bishop CW, Pitchey SJ . 1987 Estimation of the mid-upper arm circumference measurement error J. Am. Diet. Assoc. 87: 469–473
Brabin L, Ikimalo J, Dollimore N, Kemp J, Ikokwu-Wonodi C, Babatunde S, Obunge O, Briggs N . 1997 How do they grow? A study of south-eastern Nigerian adolescent girls Acta Paediatr. 86: 1114–1120
Branca F, Burkholder BT, Hamel M, Parvanta A, Robertson A . 1996 Health and nutrition survey of internally displaced and resident population of Azerbaijan–April 1996 Atlanta, GA: Centers for Disease Control and Prevention
CDC. 1992 Nutritional needs surveys among the elderly–Russia and Armenia, 1992 Morbid. Mortal. Weekly Rep. 41: 809–810
Chamruengsri K, Kietduriyakul V, Pava-Ro U, Sapsamarnwong C, Chandumpai P . 1991 Nutritional status of low socioeconomic school children at Srakaew Temple, Ang Thong J. Med. Assoc. Thai. 74: 24–29
Chaturvedi S, Kapil U, Bhanthi T, Gnanasekaran N, Pandey RM . 1994 Nutritional status of married adolescent girls in rural Rajasthan Indian J. Pediatr. 61: 695–701
Cole TJ . 1991 Weight-stature indices to measure underweight, overweight, and obesity In: Anthropometric Assessment of Nutritional Status ed. JH Himes, pp 83–111 New York: Wiley–Liss
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH . 2000 Establishing a standard definition for child overweight and obesity worldwide: international survey Br. Med. J. 320: 1240–1243
Collins S . 1993 The need for adult therapeutic care in emergency feeding programs. Lessons from Somalia JAMA 270: 637–638
Collins S . 1996 Using middle upper arm circumference to assess severe adult malnutrition during famine JAMA 276: 391–395
Collins S, Myatt M . 2000 Short-term prognosis in severe adult and adolescent malnutrition during famine: use of a simple prognostic model based on counting clinical signs JAMA 284: 621–626
Collins S, Myatt M, Duffield AE . 2000 The assessment of adult nutritional status in emergency-affected populations Geneva: ACC/SCN
Cookson ST, Woodruff BA, Slutsker L . 1998 Prevalence of anemia and low body-mass index among adolescents 10–19 y of age in refugee camps in Dadaab District, Kenya Atlanta, GA: Centers for Disease Control and Prevention
de Onis M, Bloessner M . 1997 WHO global database on child growth and malnutrition p 710 Geneva: WHO
de Onis M, Dasgupta P, Saha S, Sengupta D, Blössner M . 2001 The National Center for Health Statistics reference and the growth of Indian adolescent boys Am. J. Clin. Nutr. 74: 248–253
Delgado HL, Hurtado E . 1990 Physical growth and menarche in Guatemalan adolescents Arch. Latinoam. Nutr. 40: 503–517
Deurenberg P, Pieters JJ, Hautvast JG . 1990 The assessment of the body fat percentage by skinfold thickness measurements in childhood and young adolescence Br. J. Nutr. 63: 293–303
DHHS. 1981 Basic data on anthropometric measurements and angular measurements of the hip and knee joints for selected age groups 1-74 y of age, United States, 1971–1975 Hyattsville, MD: US Department of Health and Human Resources
Dreizen S, Spirakis CN, Stone RE . 1967 A comparison of skeletal growth and maturation in undernourished and well-nourished girls before and after menarche J. Pediatr. 70: 256–263
Duke PM, Litt IF, Gross RT . 1980 Adolescents' self-assessment of sexual maturation Pediatrics 66: 918–920
Eveleth PB, Tanner JM . 1990 Worldwide Variation in Human Growth 2nd edn Cambridge: Cambridge University Press
Ferro-Luzzi A, James WP . 1996 Adult malnutrition: simple assessment techniques for use in emergencies Br. J. Nutr. 75: 3–10
Foster TA, Voors AW, Webber LS, Frerichs RR, Berenson GS . 1977 Anthropometric and maturation measurements of children, ages 5 to 14 y, in a biracial community–the Bogalusa Heart Study Am. J. Clin. Nutr. 30: 582–591
Freedman DS, Perry G . 2000 Body composition and health status among children and adolescents Prev. Med. 31: S34–S53
Frisancho AR . 1981 New norms of upper limb fat and muscle areas for assessment of nutritional status Am. J. Clin. Nutr. 34: 2540–2545
Fuller NJ, Jebb SA, Goldberg GR, Pullicino E, Adams C, Cole TJ, Elia M . 1991 Inter-observer variability in the measurement of body composition Eur. J. Clin. Nutr. 45: 43–49
Garcia Llop LA, Ramada Benedito A, Rodriguez-Estecha P . 1990 Relationship between sexual maturation and subcutaneous fat An. Esp. Pediatr. 33: 349–353
Gasser T, Ziegler P, Kneip A, Prader A, Molinari L, Largo RH . 1993 The dynamics of growth of weight, circumferences and skinfolds in distance, velocity and acceleration Ann. Hum. Biol. 20: 239–259
Gerver WJ, De Bruin R . 1995 Relationship between height, sitting height and subischial leg length in Dutch children: presentation of normal values Acta Paediatr. 84: 532–535
Habicht JP, Martorell R, Yarbrough C, Malina RM, Klein RE . 1974 Height and weight standards for preschool children. How relevant are ethnic differences in growth potential? Lancet 1: 611–614
Hammer LD, Kraemer HC, Wilson DM, Ritter PL, Dornbusch SM . 1991 Standardized percentile curves of body-mass index for children and adolescents Am. J. Dis. Child. 145: 259–263
Hardoff D, Tamir A . 1993 Self-assessment of pubertal maturation in socially disadvantaged learning-disabled adolescents J. Adolesc. Health 14: 398–400
Hussain A, Lindtjorn B, Kvale G . 1996 Protein energy malnutrition, vitamin A deficiency and night blindness in Bangladeshi children Ann. Trop. Paediatr. 16: 319–325
IRC. 1997 Nutritional status of school aged children in Kakuma refugee camp Nairobi: International Rescue Committee
James WP, Mascie-Taylor GC, Norgan NG, Bistrian BR, Shetty PS, Ferro-Luzzi A . 1994 The value of arm circumference measurements in assessing chronic energy deficiency in Third World adults Eur. J. Clin. Nutr. 48: 883–894
Jeejeebhoy KN . 1994 How should we monitor nutritional support: structure or function? New Horiz. 2: 131–138
Kurz KM . 1996 Adolescent nutritional status in developing countries Proc. Nutr. Soc. 55: 321–331
Kurz KM, Johnson-Welch C . 1994 The nutrition and lives of adolescents in developing countries: findings from the nutrition of adolescent girls research program Washington, DC: International Center for Research on Women
Leung SS, Lau JT, Xu YY, Tse LY, Huen KF, Wong GW, Law WY, Yeung VT, Yeung WK, Leung NK . 1996 Secular changes in standing height, sitting height and sexual maturation of Chinese–the Hong Kong Growth Study, 1993 Ann. Hum. Biol. 23: 297–306
Malina RM . 1991 Ratios and derived indicators in the assessment of nutritional status In: Anthropometric Assessment of Nutritional Status ed. JH Himes, pp 151–171 New York: Wiley–Liss
Martinez E, Devesa M, Bacallao J, Amador M . 1993 Subscapular/ triceps index: percentile values in Cuban children and adolescents Arch. Latinoam. Nutr. 43: 199–203
McNabb SJ, Welch K, Laumark S, Peterson DE, Ratard RC, Toole MJ, Farley TA . 1994 Population-based nutritional risk survey of pensioners in Yerevan, Armenia Am. J. Prev. Med. 10: 65–70
MSF. 1995 Nutrition Guidelines 1st edn Paris: Medécins sans Frontières
Neinstein LS . 1982 Adolescent self-assessment of sexual maturation: reassessment and evaluation in a mixed ethnic urban population Clin. Pediatr. (Phila.) 21: 482–484
Norgan NG . 1994a Interpretation of low body mass indices: Australian aborigines Am. J. Phys. Anthropol. 94: 229–237
Norgan NG . 1994b Population differences in body composition in relation to the body mass index Eur. J. Clin. Nutr. 48: (Suppl 3): S10–25 discussion S26–27
Norgan NG . 1994c Relative sitting height and the interpretation of the body mass index Ann. Hum. Biol. 21: 79–82
Norgan NG, Jones PR . 1995 The effect of standardising the body mass index for relative sitting height Int. J. Obes. Relat. Metab. Disord. 19: 206–208
Omura M, Zinno S, Harada T, Inoue N . 1993 Evaluation of validity of five weight-height obesity indices Fukuoka Igaku Zasshi 84: 305–310
Owa JA, Adejuyigbe O . 1997 Fat mass, fat mass percentage, body mass index, and mid-upper arm circumference in a healthy population of Nigerian children J. Trop. Pediatr. 43: 13–19
Pathmanathan G, Prakash S . 1994 Growth of sitting height, subischial leg length and weight in well-off northwestern Indian children Ann. Hum. Biol. 21: 325–334
Qamra SR, Mehta S, Deodhar SD . 1990 Evaluation of anthropometric indices for the assessment of nutritional status in girls–III Ind. Pediatr. 27: 1275–1279
Riley AP . 1990 Dynamic and static measures of growth among pre- and postmenarcheal females in rural Bangladesh Am. J. Hum. Biol. 2: 255–264
Riley AP, Huffman SL, Chowdhury AK . 1989 Age at menarche and postmenarcheal growth in rural Bangladeshi females Ann. Hum. Biol. 16: 347–359
Rolland-Cachera MF, Cole TJ, Sempe M, Tichet J, Rossignol C, Charraud A . 1991 Body Mass Index variations: centiles from birth to 87 y Eur. J. Clin. Nutr. 45: 13–21
Samsudin. 1990 The age of menarche as related to physical growth of junior high school girls in Jakarta Paediatr. Indones. 30: 254–260
Shizgal HM, Vasilevsky CA, Gardiner PF, Wang WZ, Tuitt DA, Brabant GV . 1986 Nutritional assessment and skeletal muscle function Am. J. Clin. Nutr. 44: 761–771
Simondon KB, Simon I, Simondon F . 1997 Nutritional status and age at menarche of Senegalese adolescents Ann. Hum. Biol. 24: 521–532
Singh R . 1995 Secular increase in body size and nutritional anthropometric measurements of Indian children In: Essays on Auxology ed. R Hauspie, G Lindgren & K Falkner, pp 332–333 Avon: Castlemead
Spurr GB, Reina JC, Barac-Nieto M . 1983 Marginal malnutrition in school-aged Colombian boys: anthropometry and maturation Am. J. Clin. Nutr. 37: 119–132
Strickland SS, Ulijaszek SJ . 1992 Energy nutrition of Iban in Song and Kanowit, February–April 1990 Sarawak Museum J. 43: 135–196
Tanner JM . 1976 Population differences in body size, shape and growth rate. A 1976 view Arch. Dis. Child. 51: 1–2
The Sphere Project. 1998 Humanitarian Charter and Minimum Standards in Disaster Response 1st edn Geneva: IFRC
Toole MJ, Serdula M . 1996 Determining the nutritional status of the elderly in post-cold war Russia Am. J. Public Health 86: 299–301
Toriola AL . 1990 Anthropometric assessment of nutritional status of Nigerian children Trop. Geogr. Med. 42: 337–341
Victora CG . 1992 The association between wasting and stunting: an international perspective J. Nutr. 122: 1105–1110
WHO. 1995 Physical status: the use and interpretation of anthropometry Report of a WHO Expert Committee Geneva: World Health Organization
WHO. 2000 The Management of Nutrition in Major Emergencies 2nd edn, p 236 Geneva: World Health Organization
Woodruff BA, Slutsker L, Cook ST . 1998 Prevalence of anemia and low body-mass index in adolescents 10–19 y of age in Kakuma camp, Kenya Atlanta, GA: Centers for Disease Control and Prevention
Woodruff BA, Duffield A, Blanck H, Larson MK, Pahari S, Bhatia R . 1999 Prevalence of low body mass index and specific micronutrient deficiencies in adolescents 10–19 y of age in Bhutanese refugee camps, Nepal, October 1999 Atlanta, GA: Centers for Disease Control and Prevention
Young H, Jaspars S . 1995 Nutrition, disease and death in times of famine Disasters 19: 94–109
Yun DJ, Yun DK, Chang YY, Lim SW, Lee MK, Kim SY . 1995 Correlations among height, leg length and arm span in growing Korean children Ann. Hum. Biol. 22: 443–458
Acknowledgements
We are grateful to the following reviewers for their comments: Monika Blössner (WHO), Tim Cole (Institute of Child Health), Mary Corbett (Concern), Mercedes de Onis (WHO), Mike Golden (University of Aberdeen), Saskia van der Kam (Médecins sans Frontières), Carlos Navarro-Colorado (Action contre la Faim), Nick Norgan (University of Loughborough), Claudine Prudhon (Action contre la Faim), Simon Strickland (London School of Hygiene and Tropical Medicine), and Stanley Ulijaszek (Oxford University).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Woodruff, B., Duffield, A. Anthropometric assessment of nutritional status in adolescent populations in humanitarian emergencies. Eur J Clin Nutr 56, 1108–1118 (2002). https://doi.org/10.1038/sj.ejcn.1601456
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejcn.1601456
Keywords
This article is cited by
-
Prevalence and associated factors of stunting and thinness among adolescent Somalian refugee girls living in eastern Somali refugee camps, Somali regional state, Southeast Ethiopia
Conflict and Health (2019)
-
Assessment of nutritional status using anthropometric variables by multivariate analysis
BMC Public Health (2019)
-
Prevalence and factors associated with stunting and thinness among adolescent students in Northern Ethiopia: a comparison to World Health Organization standards
Archives of Public Health (2015)
-
Child health in Syria: recognising the lasting effects of warfare on health
Conflict and Health (2015)
-
Impact of maternal under nutrition on obstetric outcomes
Journal of Endocrinological Investigation (2015)
