
Abstract
Data sources Medline (1980–present) and bibliographic citations from each article were consulted to find relevant studies.
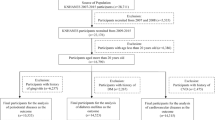
Study selection Analyses were restricted to cohort studies published between 1980 and February 2001 so that any effects of secular trends could be minimised. Studies were included if sample size was over 100 and if the ascertainment of exposure before outcome provided relative risk (RR) and confidence intervals (CI), or enough information to calculate these.
Data extraction and synthesis Studies were reviewed by two dentists and two physicians. The RR, CI and standard errors were extracted or calculated. The quality of studies was assessed with a combination of modified Liddle's criteria. Homogeneity was assessed with Q statistics and the data were analysed using a random-effects model.
Results The summary RR was 1.19 (95% CI, 1.08–1.32), indicating a higher risk of future cardiovascular events in individuals who had periodontal disease than in those who did not. In an analysis stratified to individuals of ⩽65 years of age, the RR was 1.44 (95% CI, 1.20–1.73).
Conclusions Periodontal disease appears to be associated with a 19% increase in the risk of future cardiovascular disease (CVD). This increase in RR is more prominent (44%) in individuals under 65 years of age. The increment of risk between subjects with or without periodontal disease in the general population is modest, at around 20%, because nearly 40% of population has periodontal disease. This modest increase may have a profound public health impact, however.
Similar content being viewed by others

Commentary
This meta-analysis was restricted to cohort studies investigating the possible correlation between periodontal disease and coronary heart disease and stroke. The authors examined the effect of the use of proxy measures for periodontal disease and the influence of residual confounding variables on the summary value for relative risk (RR). Specific analysis for risk in people aged ⩽65 years old and for stroke was also examined.
The nine studies analysed gave a RR of 1.19, which increased to 1.44 for individuals aged ⩽65 years old. When fatal cardiac diseases and stroke were considered as outcomes, the RR were 1.54 and 2.85, respectively. Residual confounding in some studies probably overestimated the risk by 12.9% and the proxy employed in other studies underestimated the same by 29.7%. However, in combination, the summary weighted average for periodontal to cardiac disease relation assessment might be reasonably unbiased.
The methodology applied in the present meta-analysis was good and publication bias probably did not occur. Cohort studies were correctly chosen to establish the possible association between CVD and periodontal disease because both pathologies (outcome and exposure) are chronic conditions. When they are investigated in cross-sectional studies, the temporal relationship cannot be inferred.
The rubric for quality assessment of studies included in such an analysis should take into account the mean age in sample groups in those studies. Investigations that tested the hypothesis that poorer periodontal status increased the risk for systemic conditions have had serious problems when the sample mean age was less than 30 years old: it is difficult to establish a valid association between periodontal disease and CVD when the mean age of people included is low because the prevalence of severe periodontal disease is also low.1
The studies considered in the present paper were heterogeneous. Despite the fact that there was a clear definition of cardiovascular events and of the assessment, distinct pathologies were joint outcomes. Periodontal disease was defined as gingivitis or periodontitis. The micro-organisms and immunological host response to such conditions are quite different. Since the potential biological mechanism linking periodontal disease and CVD involves the increase in C-reactive protein and fibrinogen levels and the migration of periodontopathogens to the cardiac valve and these changes are not seen in gingivitis, studies considering periodontal disease gingivitis as a predictor variable should be avoided.
Since the potential biological mechanism linking periodontal disease and CVD involves the increase in C-reactive protein and fibrinogen levels and the migration of periodontopathogens to the cardiac valve and these changes are not seen in gingivitis, studies considering periodontal disease gingivitis as a predictor variable should be avoided.
The authors would contend that change in humoral milieu is sufficient to initiate the pathogenesis of cardiovascular disease.2, 3 Thus, including gingivitis is justified. However conducting the analysis separately for gingivitis and periodontal disease would provide information to assess the real importance in screening periodontal disease in patients at risk for CVD, since gingivitis is very common in all populations. In addition, the risk for CVD should be considered in separate analyses for mild and severe periodontitis.
Practice point
-
There is insufficient evidence to suggest that periodontal disease screening and periodontal treatment in people at risk for CVD would reduce the incidence of CVD.
References
Sheiham A, Netuveli GS . Periodontal diseases in Europe. Periodontology 2000 2002; 29:104–121.
Libby P, Ridker P, Maseri A . Inflammation and atherosclerosis. Circulation 2002; 105:1135–1143.
Ross R . Atherosclerosis — an inflammatory disease. N Engl J Med 1999; 340:115–126.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Sok-Ja Janket, DMD, MPH, Boston University Goldman School of Dental Medicine, Rm. 619, E. Newton Street, Boston, USA. E-mail: sjanket@hsph.harvard.edu.
Janket SJ, Baird AE, Chuang SK, Jones JA. Meta-analysis of periodontal disease and risk of coronary heart disease and stroke. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003; 95:559–569
Rights and permissions
About this article
Cite this article
Vettore, M. Periodontal disease and cardiovascular disease. Evid Based Dent 5, 69 (2004). https://doi.org/10.1038/sj.ebd.6400272
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400272
This article is cited by
-
Short-term changes on C-reactive protein (CRP) levels after non-surgical periodontal treatment in systemically healthy individuals
Clinical Oral Investigations (2017)
