
Abstract
Previously, we conducted dual energy x-ray absorptiometry (DXA) (Hologic QDR-1000/W) scans and carcass analysis of piglets to evaluate the Pediatric Whole Body software (PedWB) (V5.35) for use in infants. A software upgrade designed for infant whole body (InfWB) (V5.56) led to a reassessment of DXA by: 1) reanalysis of the original scans using InfWB software and 2) comparison of InfWB-estimates of bone mineral content (BMC) and lean and fat mass with chemical analysis. Other assessments included 1) methods of regional analysis and 2) artifacts and the Infant Table Pad in the scan field. The mean coefficients of variation for InfWB whole body measures in small piglets(n = 10, weight 1575 ± 73 g) and large piglets (n = 10, weight 5894 ± 208 g) were less than 2.6% except for fat mass which was higher (8.0% versus 6.3% and 6.6% versus 3.5%, respectively) compared with PedWB. In large piglets InfWB produced good estimates of BMC, lean and fat masses. In small piglets, fat mass by InfWB was correlated with chemical analysis, but not by PedWB. There was improvement in the estimation of BMC with InfWB, from 27 ± 2.2 g to 32 ± 2.3 g(carcass ash = 38 ± 3.3 g). Femur BMC analysis by InfWB was precise and was accurate when compared with chemical analysis. Artifacts in the DXA scan field (diapers and blankets) resulted in an increase of the DXA-estimated fat and lean masses. The Infant Table Pad increased the estimate of fat mass in a small piglet by 50%, thus further study is required before it is used routinely. Improvements of the DXA technology have resulted in a more accurate tool, if scanning procedures are carefully implemented.
Similar content being viewed by others

Main
A “gold standard” method is needed to measure total body composition including bone and soft tissue components, which has been validated and universally accepted for clinical assessment in infants. DXA is a relatively new imaging approach with analytical software programs specifically designed to assess the composition of small bodies, including human infants and rats. DXA estimates total BMC and total body soft tissue, the latter of which can be separated into total body fat and lean masses by virtue of using factory-installed calibration materials that simulate the attenuation properties of lean and fat(2). Other imaging techniques that can measure bone and soft tissue include computed tomography, with a radiation exposure too high to permit safe use in human infants, and magnetic resonance, which generally has limited access for research purposes. TOBEC has recently been investigated for use in infants(3, 4), but is limited because it measures only the lean soft tissue compartment. Other indirect measures of fat free mass such as40 K counting and estimating dilution space by stable isotope methodology are difficult to conduct accurately(5, 6).
Despite the growing use of DXA in small infants for clinical and research purposes(1, 7–10), validation of the precision and accuracy of DXA in infants has been mostly limited to in vitro repeated measures of small tissue phantoms or excised bone(9, 11). In our previous validation study(1), using the original PedWB from the manufacturer(Hologic Incorporated, Waltham, MA), repeated DXA measurements of live piglets(approximately 6.0-kg body weight) were precise and accurate compared with chemical carcass analysis. However, in small piglets (1.6-kg body weight) the accuracy of DXA-estimated whole body BMC was low, and total body fat was overestimated by greater than 200%. Subsequent to these findings, the manufacturer provided an upgrade to the PedWB, which is identified as InfWB.
The primary objective of this study was to assess the precision and accuracy of DXA estimates of whole body weight, BMC, and fat and lean mass in the piglets when analyzed with the revised software (InfWB) compared with the original findings (PedWB and chemical carcass analysis). Also the effect of the precision of DXA on the interpretation of changes in fat mass and BMC over time was assessed in infants. DXA also offers the option to conduct regional analysis of identified areas of interest on a scan, but whether these estimates have the same accuracy and precision as obtained with specialized software for specific bone regions has not been evaluated in small infants. Therefore, the second aim was to assess the accuracy and precision of regional analyses of BMC in small bones by comparing in vivo measurements in piglet femurs with ash weight.
To optimize the conditions for DXA measures of whole body composition, consideration must be made for artifacts that may interfere with the attenuation of the photons. For ethical and practical purposes, infants must wear diapers and be kept warm with blankets. To minimize the radiation dose delivered to the infant, a device called an Infant Table Pad was provided as an option for use with the InfWB. It was designed to improve the linearity within the thin regions of the infant (product literature). Variations in the estimates of body composition as a result of such artifacts in the scan field have not been thoroughly assessed. Therefore, the third objective was to determine the influence of artifacts in the scan field, including the Infant Table Pad, on the precision and absolute results of DXA estimates of whole body composition.
METHODS
Piglets used in the present analysis were involved in different studies(1, 12), but all were obtained from the Swine Research Facility, Arkell Farms (Guelph, ON) and transported to the McMaster University Central Animal Facility. Details of the methods of piglet care and chemical carcass analysis have been published(1, 13). In the previous study two specific weight groups of piglets were targeted for measurements, 1.6 kg (small piglets, n = 10) and 6.0 kg(large piglets, n = 10)(1). These weights were chosen to approximate the lowest and mid-range weight of infants who would be of clinical research interest.
DXA scan procedure. Scans were performed using a Hologic QDR-1000/W (Hologic Inc., Waltham, MA). The principles of dual photon absorptiometry to estimate tissue composition are described in detail elsewhere(14). Triplicate whole body scans were conducted with piglets uncovered and with legs extended from the body. The Infant Table Pad was not used. Upon completion of the scans, the piglets were killed with an injection of sodium pentobarbital. The whole carcass was immediately frozen for subsequent chemical analysis as described previously(1).
Whole body scan analysis in piglets. Individual scans were originally analyzed using the PedWB Option (V5.35). The software upgrade(InfWB V5.56) had the capability to reanalyze scans from previous software versions, thus the original scans were loaded into the program and re-analyzed by a single operator (J.A.B.). According to the manufacturer, the new InfWB software included a revised algorithm which separated the image into small local regions of tissue in which was evaluated the bone mineral content. The estimates of soft tissue mass were supposed to be the same between the two software versions.
Accuracy and precision of InfWB regional analysis of BMC. Thirty-nine male piglets between 2.5 and 15 kg were anesthetized and measured at 22 (n = 6) and 37 (n = 33) d of age to estimate left femur BMC by two different DXA scan modes: 1) InfWB-estimated BMC was determined by regional isolation of the left femur by a single operator(H.A.W.), 2) subsequently, the F program V4.47P was used to estimate BMC of the left femur. After the DXA measures, the piglets were killed by an injection of sodium pentobarbital, and the left femurs were removed. The femurs were cleaned with a scalpel then ashed at 600 °C for 14 d in a muffle furnace and ash weights determined. To evaluate whether the accuracy of DXA is influenced by body weight, the piglets were divided into weight categories: 1) less than 5.99 kg, 2) 6.00-7.99 kg, and 3) greater than 8.00 kg. Precision of InfWB and F was determined by triplicate scans of four piglets without repositioning. Average intraobserver precision (i.e. femur isolation) was determined by triplicate analyses of individual InfWB and F scans by the same operator (H.A.W.).
Infant whole body scans. Serial DXA whole body measurements of infants were conducted to determine whether DXA was sensitive enough to detect significant or true changes. This was evaluated using the CV% determined from the piglet experiments in the equation(15): Prematurely born female infants (n = 26, gestational age = 25.7 ± 1.7 wk, birth weight = 800 ± 151 g) were recruited from the neonatal intensive care unit at the Children's Hospital at Chedoke McMaster, Hamilton, ON, as part of an ongoing clinical nutrition trial. The study was approved by the Research Project Advisory Committee, and informed parental consent was obtained. During routine visits to the Growth and Development Follow-up Clinic at term and at 3, 6, and 12 mo(adjusted for prematurity), serial DXA measures were conducted. Caregivers were asked to bring their infants to the clinic hungry and were asked not to let their infants sleep on the way to the clinic visit. An experienced pediatric research nurse fed and cuddled the infants until sleep was induced. Infants were laid on the scan bed on their stomachs and were scanned once using the InfWB software without the Infant Table Pad. No sedation was used.

The influence of artifacts in the scan field. Two additional piglets (1.7 and 6.4 kg) were killed with an injection of sodium pentobarbital and weighed on an electronic scale accurate to 1 g (Sartorius, Germany), then immediately frozen in the scanning position. In our previous study, we assessed the effect of scanning a live anesthetized piglet versus the frozen carcass, and found no difference(1). In each of the conditions tested, the small piglet was scanned four times, and the large piglet was scanned three times. The conditions included measurements with and without: 1) the Infant Table Pad under the piglets, 2) a flannel receiving blanket wrapped tightly around the piglets, 3) a disposable diaper on the piglets, or 4) a cotton flannel nightgown on the piglets.
Statistics. CV% were calculated for the repeated measures. The relationship between DXA estimates and whole carcass or femur analysis was determined by regression analyses (FigP, 6.0, Biosoft, Ferguson, MO). Also, the percent difference of DXA estimates of weight, fat and lean mass, and BMC compared with chemical analysis and with and without artifacts was calculated. The method of Bland and Altman(16) was used to assess the agreement between scan modes (InfWB and F) for interpretation of DXA small bone analysis. For the infant studies, the percent change necessary to detect a true change (calculated from the CV%) was compared with the actual mean percent change (%▵) determined from serial scans of infants. The level of significance for all tests was p < 0.05.
RESULTS
Piglet whole body scan analysis. With the revised software a loss of precision in the measurement of fat was observed(Table 1). The range of CV values using InfWB for fat mass for the 10 small and large piglets, respectively, was 0.40-16.4% and 0.9-16.9%.
Reanalysis of scans using the InfWB software resulted in an improvement in the accuracy of the estimation of total BMC and fat mass in the small piglets, and a slight improvement in the fat measurement in large piglets relative to chemical carcass analysis (Table 2). As the overestimation of fat mass in the small piglet was reduced, the estimate of lean tissue improved reciprocally.
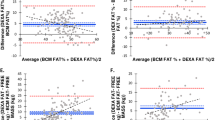
Comparison of the two software versions with chemical analysis of the small piglets (Fig. 1) showed fat mass using InfWB was still overestimated in the small piglets, but was significantly correlated to values from chemical analysis. For the large piglets, the correlations between the InfWB and carcass analysis changed very little compared with PedWB, and all were highly significant (Table 3).

Linear regression comparing PedWB and InfWB scan results with (A) body weight measured by scale, (B) total carcass ash, (C) total carcass lean mass, and (D) total carcass fat mass in small piglets. Solid line represents the line of identity, indicating exact agreement.
Accuracy and precision of InfWB regional analysis of BMC. The InfWB regional analysis of piglet femurs more accurately estimated the total ash content than did the F analysis, regardless of piglet size(Table 4). The mean femur BMC was 5.71 ± 1.99 g by InfWB and 4.87 ± 1.71 g by F, compared with the mean ash weight of 6.39± 2.49 g. The regression equation for InfWB BMC versus ash weight was y = 0.73x + 1.06, r = 0.91,p < 0.01, and y = 0.62x + 0.93, r = 0.89, p < 0.01 for F BMC versus ash weight. The intercepts were significantly different from zero. When body weight was not considered, regression analysis of InfWB femur BMC versus ash weight demonstrated that single InfWB scans are preferred for estimating BMC of small bones rather than performing two separate scans. InfWB and F estimates of femur BMC were highly correlated (Fig. 2A). However, using the method of Bland and Altman(16), it was evident that the greater the femur BMC the greater the difference was between DXA estimates (Fig. 2B).

Linear regression comparing (A) InfWB BMC to F BMC (y = 0.83x + 0.10, r = 0.97, p< 0.01) and (B) the difference between InfWB and F BMC plotted against the mean BMC by the method of Bland and Altman(16). Hatched lines in B represent the mean± 2 SD, y = 0.15x + 0.04, r = 0.52,p < 0.01.
The average CV for femur BMC measures were similar between InfWB and F (3.3± 1.8% and 2.0 ± 1.2%, respectively). The intraobserver variation for the isolation of the femur was 1.5 ± 1.2% for the InfWB and 1.2 ± 0.9% for the F.
Whole body scans in infants. In the group of premature infants, fat accretion as estimated by DXA between term (40 wk) and 3 mo, and 3 and 6 mo adjusted age exceeded the variability of the measurement (Fig. 3A). Between 6 and 12 mo the rate of fat deposition appeared to decline; thus DXA-estimated changes in fat mass may be confounded by the degree of imprecision of the measurement. Changes in whole body BMC of the premature infants (Fig. 3B) between all time points measured exceeded the variability of InfWB measurement of BMC.

The mean DXA-estimated (A) fat mass and(B) whole body BMC of a group of prematurely born infants measured serially from term age to 12 mo adjusted age. (A) To detect a true or significant change in fat mass, the percent difference (%▵) between measurements must be > 18.7% (based on a CV of 6.6%)(15). Premature infants: A%▵ = 60.2%, B%▵ = 26.5%, C%▵ = 14.0%.(B) To detect a true or significant change in BMC, the percent difference (%▵) between measurements must be > 3.1% (based on a CV of 1.1%)(15). Premature infants: A%▵= 60.0%, B%▵ = 47.7%, C%▵ = 42.3%.
Influence of artifacts in the scan field. Scanning the small piglet with the Infant Table Pad appeared to improve the CV of the measurement of total body fat (2.8% versus 8.9% without the pad), but the absolute weight of fat increased by almost 50%. The measurement of BMC was more variable (higher CV%) with all artifacts tested (Table 5). Part of the weight of each artifact was reflected in higher DXA-estimated body weights when the piglets were scanned with an artifact compared with without an artifact. Heavier artifacts produced a greater error in the measurements (Table 5).
DISCUSSION
Both technical and biologic factors have a bearing on our ability to accurately interpret changes in body composition in rapidly growing infants. Currently, there is no method for measuring total body fat in small infants that has been demonstrated as safe, accurate, and precise. Methods used include skin fold measurements, dilution space, TOBEC, and DXA. However, these methods often do not agree(17) and may misrepresent patterns of change in body fat in individual infants over time. TOBEC measures FFM, but unlike DXA, estimates total fat by subtracting FFM from body weight. Fiorotto et al.(3) reported that TOBEC estimates of FFM in infants less than 2.8 kg were unreliable and often greater than the body weight. In addition, the difference in small piglets (1-10 kg) between chemical carcass analysis and TOBEC ranged from -8.2 to 10.2%(3), which would translate into significant errors in total body fat mass. In our study, DXA was accurate in estimating lean mass and suggests that DXA rather than TOBEC may be the more appropriate method of measuring FFM in small infants. The new software for DXA measurements provided with the Hologic QDR1000W machine improved the estimates of both lean and fat mass; however, absolute fat mass was still overestimated compared with fat extraction from the carcass in all piglets. Unlike the previous software, the values for fat determined by InfWB and chemical analysis were significantly correlated. The overestimation of fat mass by DXA produced a systematic error, in contrast to TOBEC in which the error in measurement was variable(3). A significant correlation does not imply accuracy(18), but provides a basis from which a mathematical model may be developed to correct InfWB fat values. However, such a model would be limited in its application to animals of similar size and body composition. Further validation is required to determine whether the error in accuracy of fat mass by DXA in a piglet with less than 6% body fat can be extrapolated to human infants who normally have a much higher proportion of body weight as fat (i.e. > 20%).
DXA estimates of fat are subject to low precision (CV = 6.6%) even in large piglets. Li et al.(10) reported a CV of 7.0% for total body fat calculated from duplicate scans in infants of 3-17 mo of age using a Hologic QDR 1000W machine. If one accepts this precision value in infants, then it appears that measurement error is not influenced by differences in the proportion of body fat between piglets and infants. Unless fat accretion between DXA scans exceeds the variability of the measurement, interpretation of serial DXA measures may be difficult. Our longitudinal measures of body composition in small infants demonstrated the importance of timing of serial DXA measurements for total body fat Fig. 3A). Between 6 and 12 mo the mean delta fat was less than the variability of the measurement. However, when the motive is to collect data to develop reference standards, or to conduct a clinical intervention trial, it is possible to calculate a sample size large enough to overcome the lack of precision(15). For our infants measured at ages 6 and 12 mo, it would take only four infants to confirm that the 14% change in body fat is not an error of precision.
In contrast to other validation studies(8, 9, 11, 19), we did not find a significant correlation between InfWB and carcass ash in small piglets. The small piglets were within a narrow body weight range (1431-1710 g), thus the range of total mineral ash was also quite narrow (31-43 g). This minimizes the possibility of a significant correlation between DXA-estimated BMC and carcass analysis(16). Even though the new InfWB is improved over the PedWB software (Table 2), our results and others(8, 9) suggest that DXA underestimates BMC in small subjects. The lack of accuracy in estimating BMC has been attributed to nonosseous mineral in total carcass ash(8, 19). However, DXA underestimated BMC for small piglet whole body (16%,Table 2) and femur (12.5%, Table 4) to a similar degree implying that nonosseous mineral does not account for differences between DXA-estimated BMC and carcass ash. It does, however, imply that the InfWB program for this DXA instrument has a detection limit for estimating BMC and as mineral content decreases, the error of estimation increases.
The high correlation but lack of absolute agreement between InfWB and F estimates of femur BMC demonstrates the inappropriateness of comparing two nonreference methods by regression analysis(16). To compare InfWB and F regional scan results, the difference in DXA-estimated BMC between the two methods was compared with the mean of the two estimates(16) (Fig. 2). This revealed a trend for the difference between scan results to increase as the size of the femur increased. However, by expressing the difference between scan estimates of femur BMC as a percent, the relationship between the error of estimate and bone size disappears, implying a systematic error.
Reliable measures of body composition in infants using DXA are further confounded by movement artifacts and clothing such as diapers and covers. Although it might be easier to restrict movement while scanning a single appendage such as the femur rather than the whole body, our data show that the accuracy of the femur bone mineral content was better using the regional analysis (InfWB) of the bone rather than the available software program for the hip (F). The greater inaccuracy of the isolated bone measurement with increasing bone size is likely a reflection of the differences in bone thickness in small and large piglets in comparison with the whole body and to that found in adults for whom the software was intended. Furthermore, both our data and that of Koo et al.(8) showed that artifacts such as the Infant Table Pad provided by Hologic or diapers and blankets do not interfere with the accuracy or precision of bone mineral measurements. Based on these results, we conclude that any regional analysis of bone in infants is likely best estimated from whole body scans.
Measures of fat and lean by DXA are more influenced than bone by artifacts. The Infant Table Pad demonstrated no convincing evidence of an advantage with its use. The radiation exposure for an infant whole body scan is very low at 7μSv (0.7 mrem) without the Infant Table Pad, and 3 μSv (0.3 mrem) with the Pad(8). This minimal change in safety value must be weighed against measurement differences, because InfWB-estimated total fat mass increased from 105 to 155 g with the use of the Pad. Further study of the influence of the Infant Table Pad on the measurement of soft tissue is required before the Pad should be used for routine use with infants. Until accurate measures of soft tissue are demonstrated with the Pad, single infant scans will minimize radiation exposure while avoiding the use of sedatives to accommodate prolonged scan times.
It is apparent that larger artifacts in the scan field have a more profound effect than smaller artifacts, likely affecting both the precision and accuracy of soft tissue estimates. When blankets or nightgowns are tightly bundled around the piglet, InfWB cannot completely distinguish between animal and artifact. It is likely that only the portion of the artifact that is very close to the subject's body (i.e. under and over the subject) is included in the scan as soft tissue. The flannel material was divided as lean and fat tissue, although it was not a consistent division, with lean mass accounting for 63-95% of the weight added by the various flannel artifacts tested. Diapers also altered fat and lean mass to variable degrees depending on the size of the diaper (data not shown). This may be the result of different manufacturing practices, or it may also be a reflection of the lack of precision and accuracy of InfWB measurement of fat mass.
DXA technology has improved such that it is a useful tool for estimating the total body composition of rapidly growing infants if used with caution. The experiments with various artifacts exemplify the need to conduct measurements in a consistent manner with respect to blanketing practices and diaper use. The lack of accuracy of the measurement of total body BMC in very small piglets and thus likely in small infants needs to be further addressed. The errors in accuracy of soft tissue measures are now small and systematic. Clinically useful data can be obtained in small growing subjects using DXA with a specially designed software application program such as InfWB, if serial measures of body composition are at intervals which take into account the change expected, and the precision of the instrument.
Abbreviations
- BMC:
-
bone mineral content
- CV:
-
coefficient of variation
- DXA:
-
dual energy x-ray absorptiometry
- F:
-
performance right hip software (V4.47P)
- FFM:
-
fat-free mass
- InfWB:
-
infant whole body software (V5.56P)
- PedWB:
-
pediatric whole body software (V5.35)
- SEE:
-
standard error of the estimate
- TOBEC:
-
total body electrical conductance
References
Brunton JA, Bayley HS, Atkinson SA 1993 Validation and application of dual-energy x-ray absorptiometry to measure bone mass and body composition in small infants. Am J Clin Nutr 58: 839–845
Webber CE 1995 Dual photon transmission measurements of bone mass and body composition during growth. In: Blimkie CJR and Bar-Or O(eds) New Horizons in Pediatric Exercise Science. Human Kinetics Pub Inc, Champaign, IL, pp 57–76
Fiorotto ML, de Bruin NC, Brans YW, Degenhart HJ, Visser HKA 1995 Total body electrical conductivity measurements: an evaluation of current instrumentation for infants. Pediatr Res 37: 94–100
de Bruin NC, van Velthoven KAM, Stijnen T, Juttmann RE, Degenhart HJ, Visser HKA 1995 Quantitative assessment of infant body fat by anthropometry and total-body electrical conductivity. Am J Clin Nutr 61: 279–286
Ellis KJ, Shypailo RJ 1992 Total body potassium in the infant. J Radioanal Nucl Chem 161: 61–69
Whyte RK, Bayley HS, Schwarcz HP 1985 The measurement of whole body water by H218O in newborn pigs. Am J Clin Nutr 41: 801–809
Venkataraman PS, Ahluwalia BW 1992 Total bone mineral content and body composition by x-ray densitometry in newborns. Pediatrics 90: 767–770
Koo WK, Massom LR, Walters J 1995 Validation of accuracy and precision of dual energy x-ray absorptiometry for infants. J Bone Miner Res 10: 1111–1115
Chan G 1992 Performance of dual energy x-ray absorptiometry in evaluating bone, lean body mass and fat in pediatric subjects. J Bone Miner Res 7: 369–374
Li R, O'Connor L, Buckley D, Specker B 1995 Relation of activity levels to body fat in infants 6 to 12 months of age. J Pediatr 126: 353–357
Braillon PM, Salle BL, Brunet J, Glorieux FH, Delmas PD, Meunier PJ 1992 Dual energy x-ray absorptiometry measurement of bone mineral content in newborns: validation of technique. Pediatr Res 32: 77–80
Weiler HA, Atkinson SA 1995 Dietary intervention following dexamethasone (DEX) treatment is effective in ameliorating DEX-induced growth delay and osteoporosis in infant pigs. Am J Clin Nutr 61: 910a
Canadian Council on Animal Care 1984 Guide for the Care and Use of Experimental Animals, Vol 2. Institute of Laboratory Animal Resources of the National Research Council, Ottawa, ON, Canada.
Mazess RB, Barden HS, Bisek JP, Hanson J 1990 Dual-energy x-ray absorptiometry for total-body and regional bone-mineral and soft-tissue composition. Am J Clin Nutr 51: 1106–1112
Hassager C, Jensen SB, Gotfredsen A, Christiansen C 1991 The impact of measurement errors on the diagnostic value of bone mass measurements: theoretical considerations. Osteoporos Int 1: 250–256
Bland JM, Altman DG 1986 Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 2: 307–310
Butte NF, Wong WW, Fiorotto M, O'Brian Smith E, Garza C 1995 Influence of early feeding mode on body composition of infants. Biol Neonate 67: 414–424
Godfrey K 1985 Simple linear regression in medical research. N Engl J Med 313: 1629–1636
Ellis KJ, Shypailo RJ, Pratt JA, Pond WG 1994 Accuracy of dual-energy x-ray absorptiometry for body-composition measurements in children. Am J Clin Nutr 60: 660–665
Acknowledgements
The authors thank Ine Wauben and Michelle Whelan for assisting with the scans in piglets and infants.
Author information
Authors and Affiliations
Additional information
Supported in part by the Ontario Ministry of Health.
Rights and permissions
About this article
Cite this article
Brunton, J., Weiler, H. & Atkinson, S. Improvement in the Accuracy of Dual Energy X-ray Absorptiometry for Whole Body and Regional Analysis of Body Composition: Validation Using Piglets and Methodologic Considerations in Infants. Pediatr Res 41, 590–596 (1997). https://doi.org/10.1203/00006450-199704000-00022
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199704000-00022
This article is cited by
-
Body composition in preterm infants: a systematic review on measurement methods
Pediatric Research (2023)
-
Cross-calibration of two dual-energy X-ray absorptiometry devices for the measurement of body composition in young children
Scientific Reports (2022)
-
Body composition measurement for the preterm neonate: using a clinical utility framework to translate research tools into clinical care
Journal of Perinatology (2022)
-
A comparative study using dual-energy X-ray absorptiometry, air displacement plethysmography, and skinfolds to assess fat mass in preterms at term equivalent age
European Journal of Pediatrics (2021)
-
A comparison of body composition estimates using dual-energy X-ray absorptiometry and air-displacement plethysmography in South African neonates
European Journal of Clinical Nutrition (2016)
