
Abstract
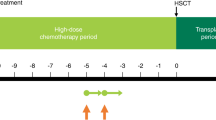
Myeloablative chemotherapy with autologous hematopoietic progenitor cell rescue has been evaluated in the treatment of children and young adults with brain tumors for whom conventional therapy is either too toxic (for example, radiotherapy in infants) or ineffective (for example, recurrent malignant tumors). With this strategy, myeloablative chemotherapy is administered to patients after initial surgery, and standard-dose chemotherapy. The success of myeloablative chemotherapy depends on the histological type of tumor, extent of disease and of surgical resection, and response to prior chemotherapy. Here, we review results of myeloablative chemotherapy with hematopoietic progenitor cell rescue in brain tumors of different histologies.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

References
Packer RJ, Meadows AT, Rorke LB, Goldwein JL, D'Angio G . Long-term sequelae of cancer treatment on the central nervous system in childhood. Med Pediatr Oncol 1987; 15: 241–253.
Packer RJ, Goldwein J, Nicholson HS, Vezina LG, Allen JC, Ris MD et al. Treatment of children with medulloblastomas with reduced-dose craniospinal radiation therapy and adjuvant chemotherapy: a Children's Cancer Group Study. J Clin Oncol 1999; 17: 2127–2136.
Finlay JL . The role of high-dose chemotherapy and stem cell rescue in the treatment of malignant brain tumors. Bone Marrow Transplant 1996; 18: S1–S5.
Mahoney Jr DH, Strother D, Camitta B, Bowen T, Ghim T, Pick T et al. High-dose melphalan and cyclophosphamide with autologous bone marrow rescue for recurrent/progressive malignant brain tumors in children: a pilot Pediatric Oncology Group Study. J Clin Oncol 1996; 14: 382–388.
Kalifa C, Hartmann O, Demeocq F, Vassal G, Couanet D, Terrier-Lacombe MJ et al. High-dose busulfan and thiotepa with autologous bone marrow transplantation in childhood malignant brain tumors: a phase II study. Bone Marrow Transplant 1992; 9: 227–233.
Dunkel IJ, Boyett JM, Yates A, Rosenblum M, Garvin Jr JH, Bostrom BC et al. High-dose carboplatin, thiotepa, and etoposide with autologous stem-cell rescue for patients with recurrent medulloblastoma. Children's Cancer Group. J Clin Oncol 1998; 16: 222–228.
Massimino M, Gandola L, Spreafico F, Luksch P, Collini P, Solero C et al. No salvage for relapsing already irradiated medulloblastoma if rescued with high-dose chemotherapy ± re-irradiation. Haematologica Rep 2007; 2: 11 (abstract).
Valteau-Couanet D, Fillipini B, Benhamou E, Grill J, Kalifa C, Couanet D et al. High-dose busulfan and thiotepa followed by autologous stem cell transplantation (ASCT) in previously irradiated medulloblastoma patients: high toxicity and lack of efficacy. Bone Marrow Transplant 2005; 36: 939–945.
Dupuis-Girod S, Hartmann O, Benhamou E, Doz F, Mechinaud F, Bouffet E et al. High-dose chemotherapy in relapse of medulloblastoma in young children. Bull Cancer 1997; 84: 264–272.
Guruangan S, Dunkel IJ, Goldman S, Garvin JH, Rosenblum M, Boyett JM et al. Myeloablative chemotherapy with autologous bone marrow rescue in young children with recurrent malignant brain tumors. J Clin Oncol 1998; 16: 2486–2493.
Chi SN, Gardner SL, Levy AS, Knopp EA, Miller DC, Wisoff JH et al. Feasibility and response to induction chemotherapy intensified with high-dose methotrexate for young children with newly diagnosed high-risk disseminated medulloblastoma. J Clin Oncol 2004; 22: 4881–4887.
Mason WP, Grovas A, Halpern S, Dunkel IJ, Garvin J, Heller G et al. Intensive chemotherapy and bone marrow rescue for young children with newly diagnosed malignant brain tumors. J Clin Oncol 1998; 16: 210–221.
Fouladi M, Gilger E, Kocak M, Wallace D, Buchanan G, Reeves C et al. Intellectual and functional outcome of children 3 years old or younger who have CNS malignancies. J Clin Oncol 2005; 23: 7152–7160.
Mulhern RK, Palmer SL, Merchant TE, Wallace D, Kocak M, Brouwers P et al. Neurocognitive consequences of risk-adapted therapy for childhood medulloblastorna. J Clin Oncol 2005; 23: 5511–5519.
Packer RJ, Gurney JG, Punyko JA, Donaldson SS, Inskip PD, Stovall M et al. Long-term neurologic and neurosensory sequelae in adult survivors of a childhood brain tumor: childhood cancer survivor study. J Clin Oncol 2003; 21: 3255–3261.
Fangusaro J, Gardner S, Abromowitch M, Allen J, Atlas M, Asgharzadeh S et al. Supratentorial primitive neuroectodermal tumors: final outcome for children enrolled on head start I and II. Neuro-oncology 2007; 9: 192.
Dunkel IJ, Garvin Jr JH, Goldman S, Ettinger LJ, Kaplan AM, Cairo M et al. High dose chemotherapy with autologous bone marrow rescue for children with diffuse pontine brain stem tumors. Children's Cancer Group. J Neurooncol 1998; 37: 67–73.
Bouffet E, Raquin M, Doz F, Gentet JC, Rodary C, Demeocq F et al. Radiotherapy followed by high dose busulfan and thiotepa: a prospective assessment of high dose chemotherapy in children with diffuse pontine gliomas. Cancer 2000; 88: 685–692.
Fangusaro J, Jubran R, Gardner S, Gonzalez I, Miller D, Finlay JL . Brainstem primitive neuroectodermal tumors (bsPNET): results of treatment with Head Start protocols. Neuro-oncology 2007; 9: 207.
Gajjar A, Chintagumpala M, Ashley D, Kellie S, Kun LE, Merchant TE et al. Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96): long-term results from a prospective, multicentre trial. Lancet Oncol 2006; 7: 813–820.
Strother D, Ashley D, Kellie SJ, Patel A, Jones-Wallace D, Thompson S et al. Feasibility of four consecutive high-dose chemotherapy cycles with stem-cell rescue for patients with newly diagnosed medulloblastoma or supratentorial primitive neuroectodermal tumor after craniospinal radiotherapy: results of a collaborative study. J Clin Oncol 2001; 19: 2696–2704.
Cohen BH, Geyer R . A pilot study of intensive chemotherapy with peripheral stem cell support for infants with malignant brain tumors. Haematologica Rep 2007; 2 (Abstract).
Dufour C, Grill J, Valteau-Couanet D, Boccacio C, Couanet D, Hartmann O et al. Feasibility and efficacy of tandem high-dose chemotherapy for patients with high-risk medulloblastoma and supratentorial primitive neuroectodermal tumors at diagnosis. Neuro-oncology 2007; 9: 193.
Foreman NK, Schissel D, Le T, Strain J, Fleitz J, Quinones R et al. A study of sequential high dose cyclophosphamide and high dose carboplatin with peripheral stem-cell rescue in resistant or recurrent pediatric brain tumors. J Neurooncol 2005; 71: 181–187.
Vassal G, Tranchand B, Valteau-Couanet D, Mahe C, Couanet D, Schoeppfer C et al. Pharmacodynamics of tandem high-dose melphalan with peripheral blood stem cell transplantation in children with neuroblastoma and medulloblastoma. Bone Marrow Transplant 2001; 27: 471–477.
Hilden JM, Meerbaum S, Burger P, Finlay J, Janss A, Scheithauer BW et al. Central nervous system atypical teratoid/rhabdoid tumor: results of therapy in children enrolled in a registry. J Clin Oncol 2004; 22: 2877–2884.
Bouffet E, Finkelstein T, Bartels U, Huang A, Taylor M, Doyle J . High dose chemotherapy in children with intracranial rhabdoid/teratoid tumorus (AT/RT); review of an institutional experience. Haematologica Rep 2007; 2 (Abstract).
Gardner S, Diez B, Green A, Horn B, Kellie S, Knopp E et al. Intensive induction chemotherapy followed by high-dose chemotherapy with autologous stem cell rescue (ASCR) in young children newly diagnosed with central nervous system (CNS) atypical teratoid rhabdoid tumors (ATT/RT)—The ‘Head Start’ regimens. Neuro-oncology 2004; 6: 455.
Finlay JL, Boyett JM, Yates AJ, Wisoff JH, Milstein JM, Geyer JR et al. Randomized phase III trial in childhood high-grade astrocytoma comparing vincristine, lomustine, and prednisone with the eight-drugs-in-1-day regimen. Childrens Cancer Group. J Clin Oncol 1995; 13: 112–123.
Sposto R, Ertel IJ, Jenkin RDT, Boesel CP, Venes JL, Ortega JA et al. The effectiveness of chemotherapy for treatment of high-grade astrocytoma in children—results of a randomized trial—a report from the Childrens-Cancer-Study-Group. J Neurooncol 1989; 7: 165–177.
Bouffet E, Khelfaoui F, Philip I, Biron P, Brunat-Mentigny M, Philip T . High-dose carmustine for high-grade gliomas in childhood. Cancer Chemother Pharmacol 1997; 39: 376–379.
Heideman RL, Douglass EC, Krance RA, Fontanesi J, Langston JA, Sanford RA et al. High-dose chemotherapy and autologous bone marrow rescue followed by interstitial and external-beam radiotherapy in newly diagnosed pediatric malignant gliomas. J Clin Oncol 1993; 11: 1458–1465.
Kedar A, Maria BL, Graham-Pole J, Ringdahl DM, Quisling RG, Mickle JP et al. High-dose chemotherapy with marrow reinfusion and hyperfractionated irradiation for children with high-risk brain tumors. Med Pediatr Oncol 1994; 23: 428–436.
Finlay JL, Goldman S, Wong MC, Cairo M, Garvin J, August C et al. Pilot study of high-dose thiotepa and etoposide with autologous bone marrow rescue in children and young adults with recurrent CNS tumors. The Children's Cancer Group. J Clin Oncol 1996; 14: 2495–2503.
Grovas AC, Boyett JM, Lindsley K, Rosenblum M, Yates AJ, Finlay JL . Regimen-related toxicity of myeloablative chemotherapy with BCNU, thiotepa, and etoposide followed by autologous stem cell rescue for children with newly diagnosed glioblastoma multiforme: report from the Children's Cancer Group. Med Pediatr Oncol 1999; 33: 83–87.
Massimino M, Gandola L, Luksch R, Spreafico F, Riva D, Solero C et al. Sequential chemotherapy, high-dose thiotepa, circulating progenitor cell rescue, and radiotherapy for childhood high-grade glioma. Neuro-oncology 2005; 7: 41–48.
Gardner S, Baker D, Belasco J, Fisher M, Phillips P, Finlay J . Phase I dose escalation of temozolomide with thiotepa and carboplatin and autologous stem cell infusion in patients with recrurrent/refractory malignant brain tumors with minimal residual disease. Haematologica Rep 2007; 2 Ref Type: Abstract.
Grill J, Kalifa C, Doz F, Schoepfer C, Sainte-Rose C, Couanet D et al. A high-dose busulfan-thiotepa combination followed by autologous bone marrow transplantation in childhood recurrent ependymoma. A phase-II study. Pediatr Neurosurg 1996; 25: 7–12.
Mason WP, Goldman S, Yates AJ, Boyett J, Li H, Finlay JL . Survival following intensive chemotherapy with bone marrow reconstitution for children with recurrent intracranial ependymoma—a report of the Children's Cancer Group. J Neurooncol 1998; 37: 135–143.
Zacharoulis S, Levy A, Chi SN, Gardner S, Rosenblum M, Miller DC et al. Outcome for young children newly diagnosed with ependymoma, treated with intensive induction chemotherapy followed by myeloablative chemotherapy and autologous stem cell rescue. Pediatr Blood Cancer 2007; 49: 34–40.
Frappaz D, Patte C, Peciulyte V, Baranzelli M, Alapetite C, Kalifa C . High dose VP 16-thiotepa with PBSC rescue in relapsing intracranial non germinomatous germ cell tumors: the SFC retrospective experience. Haematologica Rep 2007; 2 Ref Type: Abstract.
Modak S, Gardner S, Dunkel IJ, Balmaceda C, Rosenblum MK, Miller DC et al. Thiotepa-based high-dose chemotherapy with autologous stem-cell rescue in patients with recurrent or progressive CNS germ cell tumors. J Clin Oncol 2004; 22: 1934–1943.
Faulkner LB, Lindsley KL, Kher U, Heller G, Black P, Finlay JL . High-dose chemotherapy with autologous marrow rescue for malignant brain tumors: analysis of the impact of prior chemotherapy and cranio-spinal irradiation on hematopoietic recovery. Bone Marrow Transplant 1996; 17: 389–394.
Kramer ED, Packer RJ, Ginsberg J, Goldman S, Thompson S, Bayer LA et al. Acute neurologic dysfunction associated with high-dose chemotherapy and autologous bone marrow rescue for primary malignant brain tumors. Pediatr Neurosurg 1997; 27: 230–237.
Freilich RJ, Kraus DH, Budnick AS, Bayer LA, Finlay JL . Hearing loss in children with brain tumors treated with cisplatin and carboplatin-based high-dose chemotherapy with autologous bone marrow rescue. Med Pediatr Oncol 1996; 26: 95–100.
Sands SA, Van Gorp WG, Finlay JL . Pilot neuropsychological findings from a treatment regimen consisting of intensive chemotherapy and bone marrow rescue for young children with newly diagnosed malignant brain tumors. Childs Nerv Syst 1998; 14: 587–589.
Baker KS, Defor TE, Burns LJ, Ramsay NKC, Neglia JP, Robison LL . New malignancies after blood or marrow stem-cell transplantation in children and adults: Incidence and risk factors. J Clin Oncol 2003; 21: 1352–1358.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Marachelian, A., Butturini, A. & Finlay, J. Myeloablative chemotherapy with autologous hematopoietic progenitor cell rescue for childhood central nervous system tumors. Bone Marrow Transplant 41, 167–172 (2008). https://doi.org/10.1038/sj.bmt.1705953
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1705953
Keywords
This article is cited by
-
Pediatric high-grade glioma: current molecular landscape and therapeutic approaches
Journal of Neuro-Oncology (2017)
-
Phase I study of temozolomide in combination with thiotepa and carboplatin with autologous hematopoietic cell rescue in patients with malignant brain tumors with minimal residual disease
Bone Marrow Transplantation (2016)
-
Toxicity of tandem high-dose chemotherapy and autologous stem cell transplantation using carboplatin-thiotepa-etoposide and cyclophosphamide-melphalan regimens for malignant brain tumors in children and young adults
Journal of Neuro-Oncology (2014)
-
Structural brain alterations in children an average of 5 years after surgery and chemotherapy for brain tumors
Journal of Neuro-Oncology (2014)
-
Tandem high-dose chemotherapy and auto-SCT for malignant brain tumors in children under 3 years of age
Bone Marrow Transplantation (2013)
