
Abstract
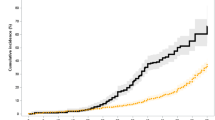
We analyzed long-term outcomes and psycho-social aspects in 112 children with malignancies surviving 1 year after hematopoietic stem cell transplantation. At 10 years, overall survival was 75±5%, TRM 18±4% and relapse 14±3%; 10-year cumulative incidence of infections was 31±4%, cataract 44±4%, pulmonary dysfunction 20±4%, bone and joint complications 29±5%, hypothyroidism 36±4%, cardiac complications 11±3% and secondary malignancies 7±3%. Total body irradiation (TBI) was the most significant risk factor associated with cataract, pulmonary impairment, osteoarticular complications and hypothyroidism. Chronic graft-versus-host disease was associated with higher incidence of pulmonary dysfunction. The number of complications per patient increased with time. Half of the patients had psychological disturbance, 13 signs of depression and 16 a history of eating behavior disorders; 54% of patients with one or more long-term complications had psychological problems. Sixty-nine patients had learning difficulties and 36 achieved normal scholarship. With increased follow-up, development of late effects and of psycho-social disturbance are of major concern. While the use of single-dose TBI has now been abandoned, other risk factors are still of concern in the early 2000s.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others


References
Socie G, Salooja N, Cohen A, Rovelli A, Carreras E, Locasciulli A et al. Nonmalignant late effects after allogeneic stem cell transplantation. Blood 2003; 101: 3373–3385.
Deeg HJ, Socie G, Schoch G, Henry-Amar M, Witherspoon RP, Devergie A et al. Malignancies after marrow transplantation for aplastic anemia and fanconi anemia: a joint Seattle and Paris analysis of results in 700 patients. Blood 1996; 87: 386–392.
Curtis RE, Rowlings PA, Deeg HJ, Shriner DA, Socie G, Travis LB et al. Solid cancers after bone marrow transplantation. N Engl J Med 1997; 336: 897–904.
Socie G, Curtis RE, Deeg HJ, Sobocinski KA, Filipovich AH, Travis LB et al. New malignant diseases after allogeneic marrow transplantation for childhood acute leukemia. J Clin Oncol 2000; 18: 348–357.
Deeg HJ, Leisenring W, Storb R, Nims J, Flowers ME, Witherspoon RP et al. Long-term outcome after marrow transplantation for severe aplastic anemia. Blood 1998; 91: 3637–3645.
Sakaida E, Nakaseko C, Harima A, Yokota A, Cho R, Saito Y et al. Late-onset noninfectious pulmonary complications after allogeneic stem cell transplantation are significantly associated with chronic graft-versus-host disease and with the graft-versus-leukemia effect. Blood 2003; 102: 4236–4242.
Faraci M, Calevo MG, Lanino E, Caruso S, Messina C, Favr C et al. Osteonecrosis after allogeneic stem cell transplantation in childhood. A case–control study in Italy. Haematologica 2006; 91: 1096–1099.
Ochs L, Shu XO, Miller J, Enright H, Wagner J, Filipovich A et al. Late infections after allogeneic bone marrow transplantations: comparison of incidence in related and unrelated donor transplant recipients. Blood 1995; 86: 3979–3986.
Barrera M, Boyd-Pringle LA, Sumbler K, Saunders F . Quality of life and behavioral adjustment after pediatric bone marrow transplantation. Bone Marrow Transplant 2000; 26: 427–435.
Andrykowski MA, Carpenter JS, Greiner CB, Altmaier EM, Burish TG, Antin JH et al. Energy level and sleep quality following bone marrow transplantation. Bone Marrow Transplant 1997; 20: 669–679.
Leung W, Hudson MM, Strickland DK, Phipps S, Srivastava DK, Ribeiro RC et al. Late effects of treatment in survivors of childhood acute myeloid leukemia. J Clin Oncol 2000; 18: 3273–3279.
Thompson JR, Gustafson KE . Adaptation to Chronic Childhood Illness. American Psychological Association: Washington, DC, 1996.
Baker F, Zabora J, Polland A, Wingard J . Reintegration after bone marrow transplantation. Cancer Pract 1999; 7: 190–197.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ferry, C., Gemayel, G., Rocha, V. et al. Long-term outcomes after allogeneic stem cell transplantation for children with hematological malignancies. Bone Marrow Transplant 40, 219–224 (2007). https://doi.org/10.1038/sj.bmt.1705710
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1705710
Keywords
This article is cited by
-
Late endocrine effects after hematopoietic stem cell transplantation in children with nonmalignant diseases
Bone Marrow Transplantation (2022)
-
Radiation-sparing reduced-intensity unrelated umbilical cord blood transplantation for rare hematological disorders in children
International Journal of Hematology (2022)
-
Post-transplant multimorbidity index and quality of life in patients with chronic graft-versus-host disease—results from a joint evaluation of a prospective German multicenter validation trial and a cohort from the National Institutes of Health
Bone Marrow Transplantation (2021)
-
Important factors associated with sick leave after allogeneic haematopoietic stem cell transplantation—a 1-year prospective study
Journal of Cancer Survivorship (2021)
-
Anxiety, depression, and mental health-related quality of life in survivors of pediatric allogeneic hematopoietic stem cell transplantation: a systematic review
Bone Marrow Transplantation (2020)
