
Abstract
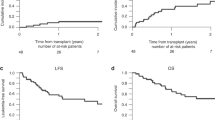
We investigated a dose-reduced conditioning regimen consisting of treosulfan and fludarabine followed by allogeneic stem cell transplantation (SCT) in 26 patients with secondary AML or MDS. Twenty patients were transplanted from matched or mismatched unrelated donors and six from HLA-identical sibling donors. The median age of the patients was 60 years (range, 44–70). None of the patients was eligible for a standard myeloablative preparative regimen. No graft-failure was observed, and leukocyte and platelet engraftment were observed after a median of 16 and 17 days, respectively. Acute graft-versus-host disease (GvHD) grade II–IV was seen in 23% and severe grade III GvHD in 12% of the patients. No patients experienced grade IV acute GvHD. Chronic GvHD was noted in 36% of the patients, which was extensive disease in 18%. The 2-year cumulative incidence of relapse was 21%. The relapse rate was higher in patients beyond CR1 or with intermediate two or high risk MDS (P=0.02). The treatment-related mortality at day 100 was 28%. The 2-year estimated overall and disease-free survival was 36–34%, respectively. No difference in survival was seen between unrelated and related SCT.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others

References
Anderson JE, Appelbaum FR, Fisher LD, Schoch G, Shulman H, Anasetti C et al. Allogeneic bone marrow transplantation for 93 patients with myelodysplastic syndrome. Blood 1993; 82: 677–681.
de Witte T, Hermans J, Vossen J, Bacigalupo A, Meloni G, Jacobsen N et al. Haematopoietic stem cell transplantation for patients with myelo-dysplastic syndromes and secondary acute myeloid leukaemias: a report on behalf of the Chronic Leukaemia Working Party of the European Group for Blood and Marrow Transplantation (EBMT). Br J Haematol 2000; 110: 620–630.
Longmore G, Guinan EC, Weinstein HJ, Gelber RD, Rappeport JM, Antin JH . Bone marrow transplantation for myelodysplasia and secondary acute nonlymphoblastic leukemia. J Clin Oncol 1990; 8: 1707–1714.
Arnold R, de Witte T, van Biezen A, Hermans J, Jacobsen N, Runde V et al. Unrelated bone marrow transplantation in patients with myelodysplastic syndromes and secondary acute myeloid leukemia: an EBMT survey European Blood and Marrow Transplantation Group. Bone Marrow Transplant 1998; 21: 1213–1216.
Slavin S, Nagler A, Naparstek E, Kapelushnik Y, Aker M, Cividalli G et al. Nonmyeloablative stem cell transplantation and cell therapy as an alternative to conventional bone marrow transplantation with lethal cytoreduction for the treatment of malignant and nonmalignant hematologic diseases. Blood 1998; 91: 756–763.
Giralt S, Estey E, Albitar M, van Besien K, Rondon G, Anderlini P et al. Engraftment of allogeneic hematopoietic progenitor cells with purine analog-containing chemotherapy: harnessing graft-versus-leukemia without myeloablative therapy. Blood 1997; 89: 4531–4536.
McSweeney PA, Niederwieser D, Shizuru JA, Sandmaier BM, Molina AJ, Maloney DG et al. Hematopoietic cell transplantation in older patients with hematologic malignancies: replacing high-dose cytotoxic therapy with graft-versus-tumor effects. Blood 2001; 97: 3390–3400.
Martino R, Caballero MD, Simon JA, Canals C, Solano C, Urbano-Ispizua A, et al., AML and alloPBSCT Subcommittees of the Spanish Group for Hematopoietic Transplantation. Evidence for a graft-versus-leukemia effect after allogeneic peripheral blood stem cell transplantation with reduced-intensity conditioning in acute myelogenous leukemia and myelodysplastic syndromes. Blood 2002; 100: 2243–2245.
Kroger N, Schetelig J, Zabelina T, Kruger W, Renges H, Stute N et al. A fludarabine-based dose-reduced conditioning regimen followed by allogeneic stem cell transplantation from related or unrelated donors in patients with myelodysplastic syndrome. Bone Marrow Transplant 2001; 28: 643–647.
Kroger N, Bornhauser M, Ehninger G, Schwerdtfeger R, Biersack H, Sayer HG et al. German Cooperative Transplant Study Group Allogeneic stem cell transplantation after a fludarabine/busulfan-based reduced-intensity conditioning in patients with myelodysplastic syndrome or secondary acute myeloid leukemia. Ann Hematol 2003; 82: 336–342 E-pub 2003 May 1.
Ho AY, Pagliuca A, Kenyon M, Parker JE, Mijovic A, Devereux S et al. Reduced-intensity allogeneic hematopoietic stem cell transplantation for myelodysplastic syndrome and acute myeloid leukemia with multilineage dysplasia using fludarabine, busulphan, and alemtuzumab (FBC) conditioning. Blood 2004; 104: 1616–1623 E-pub 2004 Apr 1.
Parker JE, Shafi T, Pagliuca A, Mijovic A, Devereux S, Potter M et al. Allogeneic stem cell transplantation in the myelodysplastic syndromes: interim results of outcome following reduced-intensity conditioning compared with standard preparative regimens. Br J Haematol 2002; 119: 144–154.
Casper J, Knauf W, Kiefer T, Wolff D, Steiner B, Hammer U et al. Treosulfan and fludarabine: a new toxicity-reduced conditioning regimen for allogeneic hematopoietic stem cell transplantation. Blood 2004; 103: 725–731 E-pub 2003 Aug 28.
Beelen DW, Trenschel R, Casper J, Freund M, Hilger RA, Scheulen ME et al. Dose-escalated treosulphan in combination with cyclophosphamide as a new preparative regimen for allogeneic haematopoietic stem cell transplantation in patients with an increased risk for regimen-related complications. Bone Marrow Transplant 2005; 35: 233–241.
Ploemacher RE, Johnson KW, Rombouts EJ, Etienne K, Westerhof GR, Baumgart J et al. Addition of treosulfan to a nonmyeloablative conditioning regimen results in enhanced chimerism and immunologic tolerance in an experimental allogeneic bone marrow transplant model. Biol Blood Marrow Transplant 2004; 10: 236–245.
Schmidmaier R, Oellerich M, Baumgart J, Emmerich B, Meinhardt G . Treosulfan-induced apoptosis in acute myeloid leukemia cells is accompanied by translocation of protein kinase C delta and enhanced by bryostatin-1. Exp Hematol 2004; 32: 76–86.
Bearman SI, Appelbaum FR, Buckner CD, Petersen FB, Fisher LD, Clift RA et al. Regimen-related toxicity in patients undergoing bone marrow transplantation. J Clin Oncol 1988; 6: 1562–1568.
Fehse B, Chukhlovin A, Kuhlcke K, Marinetz O, Vorwig O, Renges H et al. Real-time quantitative Y chromosome-specific PCR (QYCS-PCR) for monitoring hematopoietic chimerism after sex-mismatched allogeneic stem cell transplantation. J Hematother Stem Cell Res 2001; 10: 419–425.
Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty P, Hows J et al. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant 1995; 15: 825–828.
Westerhof GR, Ploemacher RE, Boudewijn A, Blokland I, Dillingh JH, McGown AT et al. Comparison of different busulfan analogues for depletion of hematopoietic stem cells and promotion of donor-type chimerism in murine bone marrow transplant recipients. Cancer Res 2000; 60: 5470–5478.
Harstrick A, Wilke H, Eberhardt W, Scheulen ME . A phase I dose escalation trial of intravenous treosulfan in refractory cancer. Onkologie 1996; 19: 153–156.
Scheulen ME, Hilger RA, Oberhoff C, Casper J, Freund M, Josten KM et al. Clinical phase I dose escalation and pharmacokinetic study of high-dose chemotherapy with treosulfan and autologous peripheral blood stem cell transplantation in patients with advanced malignancies. Clin Cancer Res 2000; 6: 4209–4216.
Trenschel R, Ditschkowski M, Elmaagacli A, Steckel N, Hlinka M, Peceny R et al. Myeloablative treosulfan as preparative regimen for allogeneic haematopoietic stem cell transplantation: a single-centre experience. Bone Marrow Transplantation 2005; 35: 754 (Abstract).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kröger, N., Shimoni, A., Zabelina, T. et al. Reduced-toxicity conditioning with treosulfan, fludarabine and ATG as preparative regimen for allogeneic stem cell transplantation (alloSCT) in elderly patients with secondary acute myeloid leukemia (sAML) or myelodysplastic syndrome (MDS). Bone Marrow Transplant 37, 339–344 (2006). https://doi.org/10.1038/sj.bmt.1705259
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1705259
Keywords
This article is cited by
-
Combination of treosulfan, fludarabine and cytarabine as conditioning in patients with acute myeloid leukemia, myelodysplastic syndrome and myeloproliferative neoplasms
Journal of Cancer Research and Clinical Oncology (2022)
-
Conditioning with fludarabine and treosulfan compared to FLAMSA-RIC in allogeneic stem cell transplantation for myeloid malignancies: a retrospective single-center analysis
Annals of Hematology (2022)
-
Comparative study of treosulfan plus Fludarabine (FT14) with busulfan plus Fludarabine (FB4) for acute myeloid leukemia in first or second complete remission: An analysis from the European Society for Blood and Marrow Transplantation (EBMT) Acute Leukemia Working Party (ALWP)
Bone Marrow Transplantation (2022)
-
Treosulfan-Based Conditioning Regimen in Haematopoietic Stem Cell Transplantation with TCRαβ/CD19 Depletion in Nijmegen Breakage Syndrome.
Journal of Clinical Immunology (2020)
-
Comparison of FLAMSA-based reduced intensity conditioning with treosulfan/fludarabine conditioning for patients with acute myeloid leukemia: an ALWP/EBMT analysis
Bone Marrow Transplantation (2019)
