
Abstract
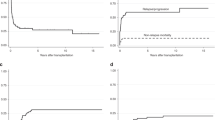
The prognosis for many pediatric and young adult patients with solid tumors that have metastasized at the time of diagnosis or have relapsed after therapy remains very poor. The steep dose–response curve of many of these tumors to alkylating agents makes myeloablative chemotherapy followed by autologous stem cell transplantation (ASCT) an attractive potential therapy. The role of ASCT for these high-risk patients is yet to be conclusively determined. We have transplanted 36 patients on two consecutive protocols with a variety of histological diagnoses. Overall survival (OS) was 63% (95% CI: 47–79%) at 1 year and 33% (95% CI: 16–50%) at 3 years. Patients with a diagnosis of Ewing's sarcoma (ES) or desmoplastic small round cell tumor (DSRCT) had significantly better survival than those with other diagnoses with estimated 3-year OS of 54% (95% CI: 29–79%) for this group of patients (P=0.03). There were two transplant-related deaths both attributable to hepatic veno-occlusive disease. Median follow-up among survivors is 3.5 years (range: 0.6–7.9 years). These data justify continued investigation of ASCT as a consolidation therapy in patients with metastatic or relapsed ES and DSRCT.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others


References
Meyers PA . High-dose therapy with autologous stem cell rescue for pediatric sarcomas. Curr Opin Oncol 2004; 16: 120–125.
Chen AR, Civin CI . Hematopoietic cell transplantation for pediatric patients with solid tumors. In: Blume KJ, Forman SJ, Appelbaum FR (eds). Thomas’ Hematopoietic Cell Transplantation. Blackwell Publishing: Massachusetts, 2004, pp 1354–1368.
Frei EJ, Canellos GP . Dose: a critical factor in cancer chemotherapy. Am J Med 1980; 69: 585–594.
Houghton JA, Cook RL, Lutz PJ, Houghton PJ . Melphalan: a potential new agent in the treatment of childhood rhabdomyosarcoma. Cancer Treat Rep 1985; 59: 91–96.
Cornbleet M, Corringham HG, Prentice HG, Boesen EM, McElwain TJ . Treatment of Ewing's sarcoma with high dose melphalan and autologous bone marrow rescue. Cancer Treat Rep 1981; 63: 241–244.
Gehan EA . Dose response relationship in clinical oncology. Cancer 1984; 54: 1204–1207.
Hartmann O, Vassal G, Valteau D, Brugieres L, Lemerle J . Autologous bone marrow transplantation in pediatric solid tumours: phase II studies. Bone Marrow Transplant 1991; 7: 106–111.
Perentesis JP, Katsanis E, DeFor TE, Neglia J, Ramsay N . Autologous stem cell transplantation for high risk pediatric solid tumors. Bone Marrow Transplant 1999; 24: 609–615.
Kaplan EL, Meier P . Nonparametric estimation from incomplete observations. J Amer Stat Assoc 1958; 53: 457–481.
Lin DY . Non-parametric inference for cumulative incidence functions in competing risks studies. Stat Med 1997; 16: 457–481.
Matthay KK, Villablanca JG, Seeger RC, Stram DO, Harris RE, Ramsay NK et al. Treatment of high risk neuroblastoma with intensive chemotherapy, radiotherapy, autologous bone marrow transplantation, and 13-cis-retinoic acid. Children's Cancer Group. New Engl J Med 1999; 341: 1165–1173.
Pein F, Michon J, Valteau-Couanet D, Quintana P, Frappaz D, Vannier JP et al. High dose melphalan, etoposide and carboplatin followed by autologous stem-cell rescue in pediatric high-risk recurrent Wilm's tumor: a French Society of Pediatric Oncology Study. J Clin Oncol 1998; 16: 3295–3301.
Campbell AD, Cohn SL, Reynolds M, Seshadri R, Morgan E, Geissler G et al. Treatment of relapsed Wilm's tumor with high dose therapy and autologous hematopoietic stem cell rescue: the experience at Children's Memorial Hospital. J Clin Oncol 2004; 22: 2885–2890.
Kremens B, Gruhn B, Klingebiel T, Hasan C, Laws HJ, Koscielniak E et al. High-dose chemotherapy with autologous stem cell rescue in children with nephroblastoma. Bone Marrow Transplant 2002; 30: 893–898.
Nishimura S, Sato T, Fujita N, Yamaoka H, Hiyama E, Yokoyama T et al. High dose chemotherapy in children with metastatic hepatoblastoma. Pediatr Int 2002; 44: 300–305.
Jubran RF, Erdreich-Epstein A, Butturini A, Murphree AL, Villablanca JG . Approaches to treatment for extraocular retinoblastoma: Children's Hospital Los Angeles experience. J Pediatr Hematol Oncol 2004; 26: 31–34.
Kremens B, Wieland R, Reinhard H, Neubert D, Beck JD, Klingebiel T et al. High-dose chemotherapy with autologous stem cell rescue in children with retinoblastoma. Bone Marrow Transplant 2003; 31: 281–284.
Kushner BH, LaQuaglia MP, Wollner N, Meyers PA, Lindsley KL, Ghavimi F et al. Desmoplastic small round cell tumor: prolonged progression-free survival with aggressive multimodality therapy. J Clin Oncol 1996; 14: 1526–1531.
Valteau-Couanet D, Kalifa C, Benhamou E . Phase II study of high dose thiotepa and hematopoietic stem cell transplantation support in children with metastatic osteosarcoma. Med Pediatr Oncol 1996; 24: 239a.
Carli M, Colombatti R, Oberlin O, Stevens M, Masiero L, Frascella E et al. High-dose melphalan with autologous stem-cell rescue in metastatic rhabdomyosarcoma. J Clin Oncol 1999; 17: 2796–2803.
Grier HE, Krailo MD, Tarbell NJ, Link MP, Fryer CJ, Pritchard DJ et al. Addition of ifosfamide and etoposide to standard chemotherapy in Ewing's sarcoma and primitive neuroectodermal tumor of bone. N Engl J Med 2003; 384: 694–701.
Miser JS, Krailo MD, Tarbell NJ, Link MP, Fryer CJ, Pritchard DJ et al. Treatment of metastatic Ewing's sarcoma or primitive neuroectodermal tumor of bone: evaluation of combination ifosfamide and etoposide – a Children's Cancer Group and Pediatric Oncology Group study. J Clin Oncol 2004; 22: 2873–2876.
Cotterill SJ, Ahrens S, Paulussen M, Jurgens HF, Voute PA, Gadner H et al. Prognostic factors in Ewing's tumor of bone: analysis of 975 patients from the European Intergroup Co-operative Ewing's Sarcoma Study Group. J Clin Oncol 2000; 18: 3104–3108.
Rodriguez-Galindo C, Billups CA, Kun LE, Rao BN, Pratt CB, Merchant TE et al. Survival after recurrence of Ewing tumors. The St Jude Children's Research Hospital Experience, 1979–1999. Cancer 2002; 94: 561–569.
Barker LM, Pendergrass TW, Sanders JE, Hawkins DS . Survival after recurrence of Ewing's sarcoma family of tumors. J Clin Oncol 2005; 23: 4354–4362.
Kalambakas SA, Moore TB, Feig SA . Megatherapy and stem cell transplantation for Ewing's family of tumors: a critical review of current literature. Pediatr Transplant 2004; 8 (Suppl 5): 83–88.
Burdach S, Jurgens H, Peters C, Nurnberger W, Mauz-Korholz C, Korholz D et al. Myeloablative radiochemotherapy and hematopoietic stem-cell rescue in poor prognosis Ewing's sarcoma. J Clin Oncol 1993; 11: 1482–1488.
Rosti G, Ferrante P, Ledermann J, Leyvraz S, Ladenstein R, Koscileniak E et al. High-dose chemotherapy for solid tumors: results of the EBMT. Crit Rev Oncol Hematol 2002; 41: 129–140.
Burdach S, Meyer-Bahlburg A, Laws HJ, Haase R, van Kaik B, Metzner B et al. High-dose therapy for patients with primary multifocal and early relapsed Ewing's tumors: Results of two consecutive regimens assessing the role of total-body irradiation. J Clin Oncol 2003; 16: 3072–3078.
Kushner BH, Meyers PA . How effective is dose-intensive/myeloablative therapy against Ewing's sarcoma/primitive neuroectodermal tumor metastatic to bone or bone marrow? The Memorial Sloan–Kettering experience and a literature review. J Clin Oncol 2001; 19: 870–880.
Meyers PA, Krailo MD, Ladanyi M, Chan KW, Sailer SL, Dickman PS et al. High-dose melphalan, etoposide, total body irradiation, and autologous stem cell reconstitution as consolidation therapy for high risk Ewing's sarcoma does not improve prognosis. J Clin Oncol 2001; 19: 2812–2820.
Ladanyi M, Gerald W . Fusion of the EWS and WT1 genes in the desmoplastic small round cell tumor. Cancer Res 1994; 54: 2837–2840.
Gerald WL, Miller HK, Battifora H, Miettinen M, Silva EG, Rosai J et al. Intra-abdominal desmoplastic small round cell tumor: report of 19 cases of a distinctive type of high grade polyphenotypic malignancy affecting young individuals. Am J Surg Pathol 1991; 15: 499–513.
Kretschmar CS, Colbach C, Bhan I, Crombleholme TM . Desmoplastic small round cell tumor: a report of three cases and review of the literature. J Pediatr Hematol Oncol 1996; 18: 293–298.
Kurre P, Felgenhauer JL, Miser JS, Patterson K, Hawkins DS . Successful dose-intensive treatment of desmoplastic small round cell tumor in three children. J Pediatr Hematol Oncol 2000; 22: 446–450.
Acknowledgements
This work was supported in part by a grant from the Children's Cancer Research Fund.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fraser, C., Weigel, B., Perentesis, J. et al. Autologous stem cell transplantation for high-risk Ewing's sarcoma and other pediatric solid tumors. Bone Marrow Transplant 37, 175–181 (2006). https://doi.org/10.1038/sj.bmt.1705224
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1705224
Keywords
This article is cited by
-
A phase I/II study of CY and topotecan in patients with high-risk malignancies undergoing autologous hematopoietic cell transplantation: the St Jude long-term follow-up
Bone Marrow Transplantation (2012)
-
Clinical outcomes of patients with desmoplastic small round cell tumor of the peritoneum undergoing autologous HCT: a CIBMTR retrospective analysis
Bone Marrow Transplantation (2012)
-
Sequential intensified chemotherapy with stem cell rescue for children and adolescents with desmoplastic small round-cell tumor
Bone Marrow Transplantation (2010)
-
Myeloablative therapy with autologous stem cell rescue for patients with Ewing sarcoma
Bone Marrow Transplantation (2008)
-
High-dose therapy with hematopoietic stem cell rescue in patients with poor prognosis Ewing family tumors
Bone Marrow Transplantation (2008)
