
Key Points
-
A technique to manage an unusual presentation of an implant abutment screw fracture is presented.
-
Causes of abutment screw loosening and fracture are reviewed.
-
Design features that improve the efficiency of the implant-abutment interface are discussed.
Abstract
This report describes the management of a loose cement-retained implant supported crown where the thread of the abutment screw had fractured away from the body of the screw and was retained within the implant. The importance of multi-disciplinary skills in the treatment of patients with implants is discussed.
Similar content being viewed by others


Introduction
Implant therapy is an effective and reliable prosthodontic treatment option.1,2,3,4 The longevity of an implant retained or supported prosthesis is dependent upon both biological and mechanical factors. Biologically, long-term osseointegration is sensitive to atraumatic implant placement and restoration.2 Mechanically, the implant, its component parts (the transmucosal abutment and abutment screw), or the prosthesis (including prosthetic screws where applicable) may fail. Mechanical complications include screw loosening, screw fracture, prosthesis fracture and problems with attachments for overdentures.5,6
Implants with a butt-joint and external hex connection to the abutment are especially prone to screw loosening when compared with internal-taper/cone joints with an anti-rotation feature.7,8 In the former, all forces, with the exception of compressive force, are concentrated on the abutment screw. The latter has the advantage of both friction and form lock, with off-axis loading mostly resisted by the taper interface.7 A review of in vivo butt-joint implant studies reported abutment screw or prosthesis screw loosening as the most frequent mechanical complication.5 Complications were most common with single crowns, particularly in the premolar and molar areas. An incidence of 0.5% to 8% was reported for abutment screw fracture. Improved clinical outcomes are reported for internal-taper joints. The incidence of abutment loosening in such a system has been reported as very low.9,10
Case report
A 24-year-old male patient attended an accident and emergency department following an alleged assault. At that time, his injuries were noted to include left peri-orbital swelling and bruising, bruising to his upper lip and a loose implant-supported crown on the maxillary left central incisor. He was referred for further prosthodontic opinion and treatment. At assessment, the maxillary left central incisor was noted to be a cement-retained implant supported crown which was loose. The clinical impression was of a loosened abutment screw: radiographically, a discrepancy could be seen between the transmucosal abutment and the fixture head (Fig. 1).

Discrepancy between abutment and fixture visible radiographically
As the loose crown was causing some discomfort to the patient, it was sectioned, the screw and abutment retrieved, and the space restored with a temporary denture. Once implant details had been confirmed (Branemark Tiunite Mk3 RP, placed three years previously and restored six months after placement with an Esthetic Abutment [3 mm] and a cemented crown), a fixture-level impression was taken and a new abutment and crown constructed. At the appointment to fit the new abutment and crown, difficulty was noted in fully seating the abutment. A small flap was raised to ensure that the fixture head was clearly exposed. The fixture head was clear, however with magnification a small fragment of metal could be seen in the implant body (Fig. 2). Visualised through a clinical microscope, the fragment was seen to be a portion of the screw-thread of the abutment screw which had fractured away from the body of the screw and was retained within the implant. Although technically demanding, it was possible to remove this fragment using endodontic instruments (Figs 3,4). The abutment was then placed and seating confirmed radiographically prior to final tightening using a torque driver at 25 Ncm (Fig. 5). At subsequent review, the patient was happy with the result (Figs 6,7), and declined further treatment to improve the gingival appearance (aesthetics were acceptable due to a low lip line).

Small fragment of metal visible in implant body with magnification

Endodontic file used to retrieve fractured thread

Fractured thread removed from implant

Abutment seating confirmed radiographically

Definitive restoration

Low lip-line covering gingival margin
Discussion
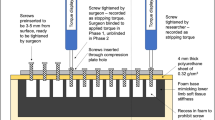
Torquing an abutment screw has a clamping effect, called the preload, which holds the abutment to the implant.11 In external hex designs, as featured in this report, the integrity of the implant-abutment joint is principally reliant on this clamping.12,13 The absence of form lock and friction, as found in internal-taper designs, results in lack of protection against the bending forces in the system implicated in screw loosening.14,15 Causes of screw loosening or fracture have been identified as inadequate tightening, adverse occlusal forces, and fatigue character and yielding strength of the screw material.16,17 Additionally, the surface of a new metal screw has microscopic surface imperfections in the form of high spots, grooves, and irregularities, such that when initial torque is applied only the high spots in the system will be in contact. Flattening and wear of these high spots is described as screw settling, and will result in the loss of some of the initial preload.18 Also, during occlusal function, the vibration and damping effect at the screw joint can result in a loss of screw preload and hence loosening.
The relationship between torque and preload is not linear.19 Friction must also be considered. Approximately 90% of the applied torque is lost as friction.20 Depending on the manufacturer and the system, recommended abutment screw torque varies from 15 Ncm to 45 Ncm.21 Even experienced clinicians have been shown to under-tighten abutment screws by 30-50%.22 However, if a screw is tightened until plastic deformation takes place, loss of preload may occur, with the possibilities of screw loosening or fracture. Therefore, torque wrenches should be used to reduce the possibility of sub-optimal torque.
The general design of abutment screws in external hex systems is worth consideration given their critical role. For optimal elongation and preload they have a long stem. Six thread lengths is typical and is said to reduce friction, with the first three threads carrying most of the load. For frictional resistance and maximum preload, the screw head seat is flat.21 They are made from gold, titanium or gold-coated titanium with the tensile and yield strengths being highest for gold screws.23,24 The yield strength of the screw material has a significant affect on preload, 75% of the yield strength of a gold screw and a titanium screw allows a preload of 890 N and 400 N respectively.21 Additionally, gold screws prevent the 'galling' effect which occurs between like for like metals used as mating parts. In metallogical terms, galling describes the excessive friction between high spots in two mating metal parts. Consequently, localised welding, subsequent splitting and further roughening of the mating parts can occur. Decreased friction between the threads also enhances the preload when a gold abutment screw is used.19 Five year retrospective studies have shown that the introduction of gold abutment screws in the single tooth Cera One implant system on butt-joint external hex Branemark implants has significantly reduced the incidence of screw loosening and fracture.6,25
Screw fracture and screw loosening are closely linked. It has been suggested that screw loosening is the first stage of screw fracture.26 When a screw loosens, surface damage occurs at high stress locations, particularly the screw head and the first thread. Consequently, some authors recommend that loose abutment screws should always be replaced as a loose screw could have a fatigue history predisposing it to fracture.11,26
Published case reports describe abutment screw fracture occurring horizontally,27,28,29,30 unlike the present case where the thread had fractured away from the body of the screw. A study of the fracture mechanisms of a retrieved titanium implant screw reported that a shear crack initiated at the root of the screw thread and propagated into the screw body;31 observation of the surface features suggested brittle fracture. Hydrogen embrittlement of titanium in a biological environment can affect the service life of titanium metal devices and the rate of absorption of hydrogen may be accelerated by plastic deformation of a screw.31
'Endodontic' techniques were required to retrieve the thread in the case described. In most cases of horizontal abutment screw fracture, the screw can be held and rotated out with an appropriate instrument if above the head of the implant, or if fracture occurs below the head of the implant, the retrieval methods are based around drilling a hole or slot into the centre of the fractured screw and engaging it with a 'screwdriver', either fashioned from regular dental surgery armamentarium or part of a manufacturer's fractured screw retrieval kit.27,30,32 Alternatively, one report describes salvaging an implant supported crown with a fractured abutment screw, by modifying the screw hole and fabricating a post crown.28
This case demonstrates the need to consider all possibilities when faced with an apparent loose abutment screw and further highlights the need for multi-disciplinary skills in the treatment of patients with implants.
References
Adell R, Eriksson B, Lekholm U, Branemark P I, Jemt T . Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. Int J Oral Maxillofac Implants 1990; 5: 347–359.
Adell R, Lekholm U, Rockler B, Branemark P I . A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int J Oral Surg 1981; 10: 387–416.
Zarb G A, Schmitt A . The longitudinal clinical effectiveness of osseointegrated dental implants: the Toronto Study. Part II: the prosthetic results. J Prosthet Dent 1990; 64: 53–61.
Zarb G A, Schmitt A . The longitudinal clinical effectiveness of osseointegrated dental implants: the Toronto study. Part I: surgical results. J Prosthet Dent 1990; 63: 451–457.
Goodacre C J, Kan J Y, Rungcharassaeng K . Clinical complications of osseointegrated implants. J Prosthet Dent 1999; 81: 537–552.
Henry P J, Laney W R, Jemt T et al. Osseointegrated implants for single-tooth replacement: a prospective 5-year multicenter study. Int J Oral Maxillofac Implants 1996; 11: 450–455.
Merz B R, Hunenbart S, Belser U C . Mechanics of the implant-abutment connection: an 8-degree taper compared to a butt joint connection. Int J Oral Maxillofac Implants 2000; 15: 519–526.
Akour S N, Fayyad M A, Nayfeh J F . Finite element analyses of two antirotational designs of implants fixtures. Implant Dent 2005; 14: 77–81.
Levine R A, Clem D S, Wilson T G, Higginbottom F, Solnit G . Multicentre retrospective analysis of the ITI implant system used for single-tooth replacements: results of loading for 2 or more years. Int J Oral Maxillofac Implants 1999; 14: 516–520.
Behneke A, Behneke N, d'Hoedt B . The longitudinal clinical effectiveness of ITI solid-screw implants in partially edentulous patients: a 5-year follow-up report. Int J Oral Maxillofac Implants 2000; 15: 633–645.
Schwarz M S . Mechanical complications of dental implants. Clin Oral Implants Res 2000; 11 Suppl 1: 156–158.
Haack J E, Sakaguchi R L, Sun T, Coffey J P . Elongation and preload stress in dental and abutment screws. Int J Oral Maxillofac Implants 1995; 10: 529–536.
Burgette R L, Johns R B, King T, Patterson E A . Tightening characteristics for screwed joints in osseointegrated dental implants. J Prosthet Dent 1994; 71: 592–599.
Jorneus L, Jemt T, Carlsson L . Loads and designs of screw joints for single crowns supported by osseointegrated implants. Int J Oral Maxillofac Implants 1992; 7: 353–359.
Norton M R . An in-vitro evaluation of the strength of an internal conical interface compared to a butt joint interface in implant design. Clin Oral Implants Res 1997; 8: 290–298.
Jemt T . Failures and complications in 391 consecutively inserted fixed prostheses supported by Branemark implants in edentulous jaws: a study of treatment from the time of prosthesis placement to the first annual checkup. Int J Oral Maxillofac Implants 1991; 6: 270–276.
Jorneus L, Jemt T, Carlsson L . Loads and designs of screw joints for single crowns supported by osseointegrated implants. Int J Oral Maxillofac Implants 1992; 7: 353–359.
Tzenakis G K, Nagy W W, Fournelle R A, Dhuru V B . The effect of repeated torque and salivary contamination on the preload of slotted gold implant prosthetic screws. J Prosthet Dent 2002; 88: 183–191.
Drago C J . A clinical study of the efficacy of gold-tite square abutment screws in cement-retained implant restorations. Int J Oral Maxillofac Implants 2003; 18: 273–278.
Yousef H, Luke A, Ricci J, Weiner S . Analysis of changes in implant screws subject to occlusal loading: a preliminary analysis. Implant Dent 2005; 14: 378–382.
Tan K B, Nicholls J I . Implant-abutment screw joint preload of 7 hex-top abutment systems. Int J Oral Maxillofac Implants 2001; 16: 367–377.
Goheen K L, Vermilyea S G, Vossoughi J, Agar J R . Torque generated by handheld screwdrivers and mechanical torquing devices for osseointegrated implants. Int J Oral Maxillofac Implants 1994; 9: 149–1 55.
McGlumphy E A, Mendel D A, Holloway J A . Implant screw mechanics. Dent Clin North Am 1998; 42: 71–89.
Rangert B, Jemt T, Jorneus L . Forces and moments on Branemark implants. Int J Oral Maxillofac Implants 1989; 4: 241–247.
Scheller H, Urgell J P, Kultje C et al. A 5-year multicenter study on implant supported single crown restorations. Int J Oral Maxillofac Implants 1998; 13: 212–218.
Quek C E, Tan K B, Nicholls J I . Load fatigue performance of a single-tooth implant abutment system: effect of diameter. Int J Oral Maxillofac Implants 2006; 21: 929–936.
Nergiz I, Schmage P, Shahin R . Removal of a fractured implant abutment screw: a clinical report. J Prosthet Dent 2004; 91: 513–517.
Pow E H, Wat P Y . A technique for salvaging an implant-supported crown with a fractured abutment screw. J Prosthet Dent 2006; 95: 169–170.
Rosen H . Salvaging endosseous implants with fractured abutment screws. Implant Dent 1995; 4: 174–176.
Williamson R T, Robinson F G . Retrieval technique for fractured implant screws. J Prosthet Dent 2001; 86: 549–550.
Yokoyama K, Ichikawa T, Murakami H, Miyamoto Y, Asaoka K . Fracture mechanisms of retrieved titanium screw thread in dental implant. Biomaterials 2002; 23: 2459–2465.
Luterbacher S, Fourmousis I, Lang N P, Bragger U . Fractured prosthetic abutments in osseointegrated implants: a technical complication to cope with. Clin Oral Implants Res 2000; 11: 163–170.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Satterthwaite, J., Rickman, L. Retrieval of a fractured abutment screw thread from an implant: a case report. Br Dent J 204, 177–180 (2008). https://doi.org/10.1038/bdj.2008.99
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bdj.2008.99
This article is cited by
-
Removal of broken abutment screws using ultrasonic tip – a heat development in-vitro study
BMC Oral Health (2024)
