
Abstract
Objective To investigate the puncture resistance of a recently introduced non-latex, nitrile dental glove in comparison with a latex glove worn during routine clinical dental procedures.
Setting Dentists in general dental practice working within the UK during 1999.
Subjects and methods 2,020 gloves worn by five general dental practitioners were examined for punctures following standard clinical use by a water inflation method. Procedures undertaken during glove usage and length of time worn were recorded.
Results Following clinical use, 1.9% of the latex gloves and 5.3% of the nitrile gloves had punctures, a statistically significant difference (P < 0.0001). The puncture resistance of the nitrile gloves was superior to the puncture resistance of previously tested worn non-latex (vinyl) gloves. There was no evidence of a statistically significant difference between operators for the percentage or incidence of punctured gloves (P = 0.787) after correcting for glove type. No statistically significant difference was noted between incidence of puncture in the control, unused gloves (n = 200 for each type) and the gloves examined following clinical use (P = 0.907 for nitrile, P = 0.613 for latex).
Conclusion No increase in the number of punctures was noted following clinical use for either glove type. This could be considered to indicate good puncture resistance of the gloves tested in clinical use.
Similar content being viewed by others
Main
Since the mid-1980s, the wearing of gloves by dental healthcare workers (DHCWs) has been an essential element of dental surgery cross-infection control procedures.1,2,3,4 Gloves may be punctured during use, with the incidence of puncture varying with different gloves and between operators.5 The risk of puncture has been shown to increase significantly when gloves are worn for dental procedures lasting longer than 2 hours.6 Until recently, gloves manufactured in latex have been most commonly used by DHCWs. However, the number of healthcare workers and DHCWs who have experienced skin problems as a result of latex sensitivity, rather than glove wearing per se, may currently be a significant proportion of the healthcare population.7,8,9,10 In this respect, 6.2% of operating theatre staff have been shown to be hypersensitive to latex proteins,11 as have 17% of hospital staff.12 It has been considered that the wearing of latex gloves is not without risk to either dental clinician or patient.13,14,15 Furthermore, the incidence of this problem would appear to be increasing – or, at least, increasingly reported. A search of Index Medicus on the key words latex, hypersensitivity and gloves revealed that the number of papers published annually on these subjects has increased from zero in 1985–6 to 36 in 1996.16
Accordingly, non-latex materials suitable for glove manufacture have been developed and introduced. Among these is nitrile, a 100% synthetic co-polymer of acrylonitrile and butadiene combined with carboxylic acid with no added softeners or plasticizers. With an absence of proteins within the glove, nitrile gloves have advantages over latex gloves in not provoking a glove type 1 allergy. Since glove puncture is a potential breach in the barrier procedures, a study of the incidence of glove puncture within a recently introduced nitrile glove type worn by DHCWs whilst carrying out different dental procedures would appear to be appropriate.
It was therefore the aim of this pilot investigation to compare the number of glove punctures occurring within two glove types – a commonly used latex type and a recently introduced non-latex, nitrile glove – during usage in everyday clinical practice by general dental practitioners.
Materials and methods
Five dentists in general practice were recruited from the members of the PREP Panel,17 a group of GDPs who undertake research projects within their dental practice. Two non-powdered glove types were identified for investigation. One was latex (Dermaclean: Ansell UK, London) and the other nitrile (Nitratex: Ansell UK, London).
All five practitioners were right handed. Each participant was sent circa 400 gloves of the correct size, 200 being latex and 200 nitrile. The participants were asked to wear one pair of gloves per patient on successive patients unless the patient's medical history precluded the wearing of latex gloves. Following treatment, their gloved hands were washed using a solution of Hibiscrub (ICI Pharmaceuticals, Macclesfield, Cheshire), the gloves were removed and placed in a labelled plastic bag. Details of the procedure(s) undertaken whilst wearing the gloves and the time for which the gloves were worn were marked on the label of each bag. Gloves that were obviously torn or punctured were also washed and placed in the bags. The gloves were returned to Glasgow Dental School for investigation.
Returned gloves were tested for punctures by a previously reported water inflation method.18 Briefly, the gloves were filled with 0.5 litre of water, held up against a dark background and gentle pressure applied at the cuff of the glove whilst observing for punctures during a 20 second period (Fig. 1). The number of punctures was recorded and their position marked on a chart. As control, 200 unused gloves of each type were also inflated by the same method and monitored for defects.

Water inflation method for puncture detection
The results were subjected to statistical analysis using tests to compare two proportions and ANOVA to examine whether the percentage of punctured gloves and the mean time of glove usage to puncture were significantly influenced by the operator and/or glove types. A chi-square test of homogeneity was used to examine whether the proportions of punctured gloves in each procedure category were homogeneous, for the two glove types.
Results
The total number of gloves used in the investigation was 2020. Of these 1,020 were nitrile and 1,000 were latex. The two glove types were worn for similar lengths of time as shown in Table 1. Details of the total number and percentage of gloves punctured and the mean time to puncture for each operator are shown in Table 2. A control of 200 unused gloves of each glove type was tested for punctures. Punctures were found in 2.5% (n = 5) of the unused latex gloves and 5.5% (n = 11) of the unused nitrile gloves.
Statistical analysis by tests to compare two proportions showed that the used nitrile gloves had a significantly greater proportion of punctures than the used latex type (P < 0.0001). However, statistical analysis of the results also showed that both the latex and nitrile gloves worn for treatment procedures did not have a significantly higher proportion of punctures (P = 0.907 for the nitrile gloves, and P = 0.613 for the latex gloves) than the unused/control group.
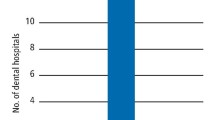
The distribution of the punctures within all used gloves is shown in Figure 2. Analysis of the type of procedures undertaken whilst wearing gloves indicated that there was no difference in the clinical procedures for which the two glove types were worn. There was no evidence to suggest a difference in the proportions of punctured gloves for each procedure category between the two glove types (P = 0.626 for chi-square test of homogeneity). The number of punctures in relation to clinical procedure is shown in Table 3 and the percentage of used glove punctures for each operator in Figure 3. There was no evidence to suggest a significant difference between operators in respect of the mean time of glove usage to puncture (P = 0.794). In addition there was no evidence to suggest a statistically significant difference between operators for the percentage or incidence of punctured gloves (P = 0.787) after correcting for glove type.

Position and overall percentage distribution of punctures for used gloves

Percentage of used glove puncture related to glove type and operator
Discussion
This investigation was a preliminary examination of the puncture resistance of one type of nitrile glove when worn during routine clinical procedures within general dental practice. No information on this subject is currently available in the literature. However, the testing of non-latex glove types may be considered important in view of the increasing adverse responses reported by dental healthcare workers18 and patients.19
The methodology used in the study has previously been applied for assessing resistance to glove puncture and represents a readily reproducible method by which large numbers of gloves may be tested without great expense or the need to purchase additional equipment.6,20,21,22 Indeed, it has been reported that electrical glove hole detection devices are unreliable when used on latex free gloves.23 However, it has been suggested, by Smith and Grant, that the water inflation method may underestimate punctures by at least 25%,24 and by Nikawa and co-workers by approximately 10%.25 The results of the present study should be interpreted in this light.
Since obvious tears or punctures on donning gloves should cause the operator to discard those gloves, this study was principally involved in the investigation of undiagnosed glove punctures ie those punctures for which the operator was unaware. However, the operators subsequently reported that only one glove had to be discarded because of obvious defects, punctures or tears during the time of participation in the investigation. No statistical difference in puncture rate was noted between operators thus discounting factors such as finger nail length and the wearing of jewellery in increasing punctures/tears in the used gloves.
The operative procedures during which the gloves were worn may be considered to be representative of those performed within a typical UK dental practice, in which different types of treatment have a different risk of glove puncture.22 However, the results indicated that the percentage of used gloves which were punctured within both glove groups in this study did not vary significantly between different operative procedures.
It is of interest to note that there was also no statistical difference between the proportions of punctures in the used and unused gloves for both glove types. This would tend to suggest that the majority of recorded punctures could have been present prior to use rather than arising during clinical procedures. This consideration is further confirmed by comparing the results of the present study with the findings in previous work,20 in which in-service punctures in gloves worn in dental practices occurred principally in the upper parts of the fingers and along the whole length of the thumb. This contrasts with the sites of punctures indicated in Figure 2, which demonstrates a diffuse pattern of punctures. The results therefore indicate that the gloves tested had good puncture resistance whilst being worn for a wide variety of clinical procedures.
The results also show that the in-service puncture resistance of gloves tested in the present study was an improvement over previously tested non-latex (vinyl) gloves and some other latex glove types.20 In the previous study, the mean time of glove wearing per puncture was 51 minutes for a vinyl glove and ranged from 328 to 2,008 minutes for latex gloves. The results of the present study indicate that the used latex glove performance tested in this study was similar to previously-tested latex gloves20 and that the incidence of puncture was lower than the incidence of glove puncture recently recorded during prosthodontic treatment.25
There seems little doubt that the number of DHCWs and patients whom exhibit sensitivity to latex will continue to increase and that the need for non-latex operating gloves will increase correspondingly. The results of this pilot study appear to imply that current nitrile gloves are more resistant to puncture during use in the treatment of patients in the dental surgery than previously tested non-latex (vinyl) glove types. However, the used nitrile glove type was seen to have a greater glove puncture rate compared with the used latex type which is in contrast with recent reports that nitrile gloves show superior puncture resistance in comparison with latex gloves.26 However, this must be taken in context with the higher incidence of punctures already present in the unused nitrile glove control group. This would suggest that, in clinical use, the nitrile gloves have at least an equivalent level of puncture resistance when compared with currently used latex gloves, with the majority of punctures present before clinical use.
It has previously been shown that the repeated use of dental gloves can lead to a higher incidence of glove puncture.27 This present study suggests that use of gloves in routine dental practice for single operative procedures may not result in a higher puncture rate compared with unused gloves, thus supporting the recommendation of changing gloves between patients.
This study has examined a large number of gloves worn during clinical practice by a group of five dental practitioners using only one nitrile glove type and one latex glove type. There is a need for further clinical studies to be carried out testing a wider range of nitrile gloves. However, the data from this project establishes that the use of nitrile gloves within dental practice shows promise and this finding may be of particular relevance to those who are unable to wear latex gloves.
Conclusion
Following use by dentists treating patients in general dental practice two non powdered glove types — one latex and one nitrile — were tested for puncture resistance. No statistically significant increase in puncture rate was noted following clinical use for either glove type compared with unused controls. Significantly greater proportions of punctures were noted in the non-latex, nitrile, unused gloves compared with unused latex gloves. The incidence of punctures at baseline was 2.5% for the latex gloves compared with 5.5% for the nitrile gloves tested.
References
Crawford J J . State-of-the-art; practical infection control in dentistry. J Am Dent Assoc 1985; 110: 629–633.
British Dental Association. Guide to blood borne viruses and the control of cross infection in dentistry. British Dental Association, 1987.
Council on Dental Materials, Instruments and Equipment, American Dental Association. Infection control recommendations for the dental office and the dental laboratory. J Am Dent Assoc 1988; 116: 241–248.
British Dental Association Advisory Service. Advice Sheet A12. The control of cross-infection in dentistry. British Dental Association, 1991.
Burke F J T, Wilson N H F . The incidence of undiagnosed punctures in non-sterile gloves. Br Dent J 1990; 168: 67–71.
Otis L L, Cottone J A . Prevalence of perforations in disposable latex gloves during routine dental treatment. J Am Dent Assoc 1989; 118: 321–324.
Burke F J T, Wilson N H F, Cheung S W . Factors associated with skin irritation of the hand experienced by general dental practitioners. Contact Dermatitis 1995; 32: 35–38.
Amin A, Palenik C J, Cheung S W, Burke F J T . Latex exposure and allergy: a survey of general dental practitioners and dental students. Int Dent J 1998; 48: 77–83.
Lonnroth E-C, Shahnavaz H . Hand dermatitis and symptoms from the fingers among Swedish Dental Personnel. Swed Dent J 1998; 22: 23–32.
Hill J G, Grimwood R E, Hermesch C B, Marks J G . Prevalence of occupationally related hand dermatitis in dental workers. J Amer Dent Assoc 1998; 129: 212–217.
Turjanmaa J . Incidence of immediate allergy to latex gloves in hospital. Contact Dermatitis 1987; 17: 270–275.
Yassin M S, Lieri M, Fischer T . Latex allergy in hospital employees.. Ann Allergy 1994: 72: 245–249.
ADA Council on Scientific Affairs. The dental team and latex hypersensitivity. J Amer Dent Assoc 1999; 130: 257–264.
Spina A M, Levine H J . Latex allergy – A review for the dental professional. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 87: 5–11.
Amin A, Palenik C J, Cheung S W, Burke F J T . Latex exposure and allergy: a survey of general dental practitioners and dental students. Int Dental J 1998; 48: 77–83.
Newsom S W B, Shaw P, Owen Smith M . A randomised trial of the durability of non-allergenic latex-free surgical gloves versus latex gloves. Ann R Coll Surg Engl 1998; 80: 288–292.
Burke F J T, Wilson N H F . Introducing the PREP Panel. Dent Pract 1994; 32: 30.
Burke F J T, Wilson N H F . Cheung S W . Factors associated with skin irritation of the hands experienced by general dental practitioners. Contact Dermatitis 1995; 32: 35–38.
Burke F J T, Wilson M A, McCord J F . Allergy to latex gloves in clinical practice: Case Reports. Quintessence Int 1995; 26: 859–863.
Burke F J T, Wilson N H F, The incidence of undiagnosed punctures in non-sterile gloves. Br Dent J 1990; 168: 67–71.
Church J, Sanderson P . Surgical glove punctures. J Hosp Med 1980; 1: 84.
Baggett F J, Burke F J T, Wilson N H F . An assessment of the incidence of punctures in gloves when worn for routine operative procedures. Br Dent J 1993; 174: 412–415.
Neal J G, Jackson E M, Cox M J, Thacker J G, Edlich R F . Failure of glove hole detection device for synthetic gloves. J Biomed Mater Res 1999; 48: 24–26.
Smith J R and Grant J M . Does wearing two pairs of gloves protect against skin contamination? Br Med J 1988; 297: 1193.
Nikawa H, Hamada T, Tamamoto M, Abekura H, Murata H . Perforation of dental gloves during prosthodontic treatments as assessed by the conductivity and water inflation tests. Int J Prosthodont 1996; 9: 362–366.
Jackson E M, Williams F M, Neal J G, Suber F, Thacker J G, Edlich R F . Biomechanical performance of examination gloves. J Biomed Mater Res 1999; 48: 572–527.
Adams D, Bagg J, Limaye M, Parsons K, Absi E G . A clinical evaluation of glove washing and re-use in dental practice. J Hosp Infect 1992; 20: 153–62.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Murray, C., Burke, F. & McHugh, S. An assessment of the incidence of punctures in latex and non-latex dental examination gloves in routine clinical practice. Br Dent J 190, 377–380 (2001). https://doi.org/10.1038/sj.bdj.4800978
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4800978
This article is cited by
-
Contemporary dental practice in the UK: demographic data and practising arrangements
British Dental Journal (2005)
-
Puncture resistance and stiffness of nitrile and latex dental examination gloves
British Dental Journal (2004)
-
A preliminary report on the incidence of pre-existing pinhole defects in nitrile dental gloves
British Dental Journal (2003)
-
For those of you allergic to latex, nitrile could be the glove material for you
British Dental Journal (2001)
