
Key Points
-
31.4% of the UK orthodontic workforce is female.
-
Female providers work slightly fewer sessions than males per week.
-
Discusses the use of various triage systems in emergency departments in dental schools.
-
Women and men complete similar numbers of cases per session.
-
Cumulatively, male providers complete 17% more cases than female providers per year.
-
As women replace men in the workforce, 17% more orthodontists will be required to achieve the same output if current working patterns remain the same.
Abstract
Objective To describe the status and activity of women in the UK orthodontic workforce.
Design and setting Postal questionnaire based on the UK orthodontic workforce.
Subjects All orthodontic providers in the UK.
Materials and methods A questionnaire was circulated to the total study population. The variables studied relating to sex were numbers, age, number of sessions worked, productivity, professional status and retirement intentions.
Results The response rate was 72.7%. 31.4% of the participants were female. The average age of female providers was 42.7 (SE 0.48) years, who were on average 4 years younger than males. Sixty-six percent of specialist trainees are women and 34% men. 41.5% of male providers and 31.6% of female providers plan to retire in the next 15 years. The mean number of sessions worked by women was 7.2 (SE 0.1) and men 8.2 (SE 0.1). Women completed 24.2 (SE 1.9) cases per session and men 25.6 (SE 1.3).
Conclusions The orthodontic workforce is becoming increasingly feminised. The cumulative effect of more women completing fewer cases will mean that workforce planners will need to consider increasing numbers to allow for this feminisation.
Similar content being viewed by others
Introduction
It was only in 1895 that the first women dentist in the UK, Lilian Lindsay, graduated from Edinburgh Dental School, and a further 17 years until a woman was granted a dental qualification from The Royal College of Surgeons of England.1 Today, females play an ever increasing role in the provision of oral and dental health care in the UK and several previous studies have reported the working patterns of female dentists in the UK2,3,4,5 and elsewhere.6,7
A survey on 'The provision of dental care by women dentists in England and Wales' undertaken in 1975 established data on the careers and work pattern of women dentists.8 A further survey2 in 1985 to determine the work pattern and commitment to career of women dentists in the 1980s allowed comparison with the data from 1975 and in June 2000, the Department of Health commissioned a review to examine the need for improvements to the employment opportunities for women dentists in the National Health Service across England. The review was undertaken in the light of the widespread perception that women found it difficult to return to dentistry after taking a career break and that 50% of women in dentistry worked no more than the equivalent of two days per week for the NHS. This was again carried out by Dame Margaret Seward and published in September 2001.9
Women will increasingly be major players in the future dental workforce. The proportion of registrations by women has risen from one quarter of new entrants in 1975, to over one third in 1985, to one half in 1991.10 By the end of the 20th century 50% of new entrants to dental undergraduate courses in the UK were female11 and by 2020 over 50% of practising dentists will be female.12
However, a greater role for women may have implications for the wider workforce. The frequency and duration of career breaks taken by female dentists is longer than that for men. The median length of career breaks for male dentists is four months but for female dental practitioners it is nine months. Female general dental practitioners (GDPs) who take a career break can be expected to have a working life 25% shorter than a GDP who does not take a career break.13 Conversely, in Ireland female orthodontists work a similar number of sessions to men.14
The working patterns of different groups amongst the workforce are important, especially if the balance between groups changes. The relationships between these patterns will determine the volume of activity undertaken by the entire workforce and so must be considered in terms of output for future planning. Therefore, this study aimed to investigate the current status and activity of women in the orthodontic workforce.
Method
This paper reports findings in relation to gender from the BOS workforce study, which was the first complete survey of the orthodontic workforce in the UK and was carried out from December 2003 until March 2004. The aim of the larger survey was to assess the UK orthodontic workforce in relation to current and future population needs.
Details of the method are provided in the substantive report but are summarised here. A rationalised database was created of all orthodontists who were identified as orthodontic providers in the UK on 31 December 2003. This included all members of the British Orthodontic Society, all dentists registered on the General Dental Council Specialist List and known to be in clinical practice, plus all non-specialist dentists who treated 30 or more orthodontic cases under the General Dental Services in the previous calendar year and identified by the Dental Practice Boards of England and Wales and Northern Ireland. The database did not include non-specialist providers not on the Specialist list in Scotland, as the Scottish DPB declined to take part in the study.
All 1660 orthodontists on this database were sent postal questionnaires either directly from the University of Sheffield or via the Dental Practice Board. Two follow up questionnaires were sent to orthodontists who did not respond to the earlier mailings.
The questionnaire was developed from one used earlier by Willmot15 and from piloting a revised questionnaire amongst 20 orthodontists local to the Sheffield area, checking for question error and relevance.
The findings in this paper relate to the following areas of enquiry:
-
Demographic factors (sex, age and retirement plans)
-
The professional status of the respondent
-
The number of clinical sessions worked (a session was regarded as a notional half-day or 3 ½ hours)
-
The number of clinical cases completed per year.
Simple descriptive analyses were used to describe demographic factors in the workforce. Productivity calculations were based on the number of sessions worked each week and the number of clinical cases completed each year per weekly session worked.
Results
The response rate for the questionnaire was 72.7% with no response bias detected. For example, women comprised 29.3, 35.3 and 33.8% of respondents to the first, second and third waves respectively.
Almost one third (31.4%) of the participants were female. The average age of female and male providers was 42.7 (SE 0.5) and 46.4 (SE 0.3) years respectively. Proportionately more male providers plan to retire in the next 15 years (Table 1).
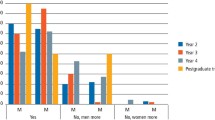
Figure 1 compares the professional status of male and female orthodontic providers. Proportionately, fewer women than men were GDPs, although women were better represented than men as Specialist Practitioners, Specialist Registrars and in the CDS. These should be interpreted with care, however, because two thirds of providers are male. Therefore when similar proportions of men and women work in the same professional group (for example as consultants) there will be twice as many men as women.

Distribution of providers according to sex in each professional group
The mean number of sessions worked by male orthodontic providers (8.2, SE 0.1) was slightly greater than women (7.2, SE 0.1) and there was a small productivity difference between genders. Women completed 24.2 (SE 1.9) treatments per session per year and men completed 25.6 (SE 1.3). Cumulatively each male provider completes 209.9 (8.2 × 25.6) cases per year. This is 17.1% more than females, who complete 174.2 (7.2 × 24.2) cases per year.
Discussion
This study aimed to investigate the status and activity of women in the orthodontic workforce in 2003. Women were younger and were less likely to be GDPs. They worked fewer sessions and completed fewer cases per session than men. Cumulatively, a female orthodontist completes 17.1% fewer cases per year than her male counterpart.
These data are interesting as they provide the first picture of the role of women in British orthodontics and indicate a feminisation of the orthodontic workforce. Moreover, the data are robust. With a response rate of 73%, no indication of trends in response by wave and a 100% sample, there is little risk of response bias or sampling error.
Women are on average four years younger than their male counterparts, reflecting the greater entry of women into the speciality in recent years. Likewise, the greater proportion of women as trainees than men again indicates that the number of women in the orthodontic workforce is rising. In addition, as the present generation of predominantly male senior orthodontists retires, the proportion of providers who are women will rise dramatically.
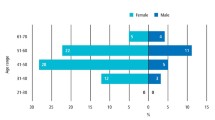
However, this phenomenon is not exclusive to orthodontics. A study on the UK workforce as a whole undertaken in November 200416 showed that an increasing proportion of women are working, with around 44% of them working part-time. The employment rate for women with pre-school children was 54%, for women with children of primary school age it was 70% and for those with children aged 11-15 it was 76%.
Changes such as these have prompted one social commentator to write: 'Unless men change, the collective evidence seems to suggest that they could become economically, socially and biologically redundant.' The crisis of masculinity is also discussed further by feminist writers,17,18 with the question being raised whether men are now facing a crisis of identity in combination with a feeling of loss for what they once had.
Ironically, a survey in 200219 found that women in general are increasingly dissatisfied with work. They reported finding it hard to juggle their responsibilities and requested an improvement in their work-life balance. Interestingly, however, the same may not be said for female dentists, with 80% of those surveyed in 2000 reporting that they would choose dentistry again and 62% saying they would recommend dentistry to other women as a career.
The data from this study indicate that female orthodontic providers work slightly fewer sessions than their male counterparts. A similar finding was noted in Ireland,14 where female orthodontists also work a similar number of sessions to men. The findings contrast with those in the dental population as a whole. Seward9 reported that 12% of female GDPs are not practising, the principle reasons being 'taking a break to care for children', 'on maternity leave', 'not working through personal choice' and 'working outside of dentistry'. Of those women who were working, nearly half (47%) worked part-time. The relative similarity between female and male work patterns in the orthodontic workforce may reflect that women who have invested in specialist training are less willing to reduce their sessions of work than their counterparts in general practice.
Although female and male orthodontists work similar patterns, cumulatively the difference in productivity per orthodontist trained or employed is tangible. In part, this difference may also be explained by the settings of the orthodontists, where the nature of cases treated by specialists, trainees and CDS dentists may reduce productivity. However, the difference in the number of sessions worked by women and men accounts for a 12.2% (8.2-7.2/8.2 × 100) difference in productivity.
These findings have consequences for the training and employment of orthodontists. As women replace men in the workforce then 17% more orthodontists will be required to achieve the same output if current working patterns remain the same. To many planners this will seem like a small price to pay for ensuring equal opportunities for women continue to prosper and to ensure diversity in the workforce, although, the additional cost will need to be met if the supply of care is to be maintained.
References
Stewart F M, Drummond J R . Women and the world of dentistry. Br Dent J 2000; 188: 7–8.
McEwen E M, Seward M H . The contribution of women to dentistry in the 1980s. Br Dent J 1988; 165: 339–341.
Boyle C A . The career pattern of Scottish female dental graduates from 1974-1983. Br Dent J 1986; 160: 138–139.
Seward M H, McEwen E M . The provision of dental care by women dentists in England and Wales in 1985: a ten year review. Br Dent J 1987; 162: 50–51.
McEwen E M, Seward M H . Women dentists at work. Br Dent J 1988; 165: 380–382.
Price S S . A profile of women dentists. J Am Dent Assoc 1990; 120: 403–408.
Pack A R, Lala J A, Sue M P, Taylor K M, Wadsworth L M . Professional and family commitments of women dentists in New Zealand. New Zeal Dent J 1987; 83: 94–97.
Seward M H . The provision of dental care by women dentists in England and Wales in 1975. London: British Postgraduate Medical Federation, 1976.
Seward M H . Better opportunities for women dentists. Crown Copyright, 2001.
Matthews R W, Scully C . Working patterns of male and female dentists in the UK. Br Dent J 1994; 176: 463–466.
Seward M . The gender challenge. Br Dent J 2000; 189: 525.
Murray J J . Better opportunities for women dentists: a review of the contribution of women dentists to the workforce. Br Dent J 2002; 192: 191–196.
Newton J T, Buck D, Gibbons D E . Workforce planning in dentistry: the impact of shorter and more varied career patterns. Community Dent Health 2001; 18: 236–241.
Blake M, Garvey M T, Healy B . An update on orthodontic manpower in Ireland. J Orthod 2001; 28: 93–95.
Willmot D R . Orthodontic workforce survey 2001. British Orthodontic Society, 2001.
Stanfield C, Campbell M, Giles L . The UK workforce: realising our potential. Sector Skills Development Agency, 2004.
Coward R . Sacred Cows – is feminism relevant to the new millennium? London: HarperCollins, 1999.
Faludi S . Stiffed: the betrayal of modern man. Chatto and Windus, 2000.
Taylor R . Diversity in Britain's labour market. ESRC Future of work programme seminar series, 2002.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Murphy, T., Parkin, N., Willmot, D. et al. The feminisation of the orthodontic workforce. Br Dent J 201, 355–357 (2006). https://doi.org/10.1038/sj.bdj.4814011
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4814011
This article is cited by
-
Flexibility and access to dental postgraduate speciality training
British Dental Journal (2023)
-
Ten years on: an online questionnaire evaluation of the UK special care dentistry specialist workforce
British Dental Journal (2021)
-
The United Kingdom's specialist workforce in paediatric dentistry: current and future trends
British Dental Journal (2010)
-
Factors which influence working patterns of orthodontists in the United Kingdom
British Dental Journal (2009)
-
Changes in the gender and ethnic balance of the United Kingdom orthodontic workforce
British Dental Journal (2008)
