
Key Points
-
Encourages professional debate about the provision of adult GA dental extraction service amongst dental professionals.
-
Many clinicians in oral and maxillofacial units currently perceive a strong culture of demand-driven adult GA dental extraction, and there is a need to address this issue.
-
Highlights the need to review the current provision of sedation in oral and maxillofacial units in the UK
Abstract
The case selection for adult dental extraction under general anaesthesia (GA) is inevitably subjective. A culture of overprescription has implications for patient safety as well as for the limited resources of the National Health Service. We explored the current perceptions and opinions of clinicians in oral and maxillofacial surgery (OMFS) units throughout the UK on various aspects of adult dental extraction under general anaesthesia (DGA) service. An email with an electronic survey link was sent to members of the British Association of Oral and Maxillofacial Surgeons and postgraduate dental deaneries. An institutional response rate of 67.3% was reached (241 clinicians of varying grades from 107 out of 159 oral and maxillofacial surgery units in the UK). There was a general consensus that the culture of demand-driven adult DGA exists and needs to be addressed. However, opinions were divided and varied on how this could be achieved. A small majority (58.1%) were in favour of adult DGA guidelines and this group provided suggestions for selection criteria. Those that did not feel such guidelines would improve the situation were pessimistic of the potential for change in patients' attitude towards DGA. This group cited the poor adherence to other existing guidelines, or suggested alternative ideas to guidelines.
Similar content being viewed by others

Introduction
The extraction of teeth under general anaesthesia (GA) is a recent luxury. Brutal extractions were the cultural norm before the discovery of anaesthesia.1 On 19 December 1846, the first anaesthetic in England was given using ether in London by a dentist, Dr James Robinson, for a molar tooth extraction.1 Since then, modern general anaesthetic techniques have evolved, and even after the introduction of lidocaine in 1946,2 the provision of dental extraction under general anaesthesia (DGA) service in the United Kingdom (UK) has continued to exist to meet not only the needs but also the shifted cultural norms.3,4
DGA in general dental practices was stopped on the grounds of safety, following the publication of A conscious decision.5 However, GA continues to be used on a discretionary basis in hospital settings in a healthcare system funded by taxation in the UK.6 Poswillo3 believed that cultural factors and patient demand influenced the decision to use GA. Hastings et al.6 explored this idea and found parents overcame reservations about their children having DGA partly because GA was frequently regarded as normal practice.6 Parents automatically associated dental extractions with 'having gas', reflecting their own and friends' and relatives' past and present experience.6
We currently do not have an accurate national DGA activity monitoring system.7 There was a huge discrepancy between DGA activity recorded by the Hospital Episode Statistics (HES) system (2,817) and that estimated by the postal questionnaire (13,500).7 The HES does not collect information on the anaesthetic modality for a dental procedure, and not all hospital day-case episodes are transferred to the HES.8 Also, some of the ones that are recorded are coded inaccurately.7
The Royal College of Anaesthetists conducted the 5th National Audit Project in an attempt to capture the National Health Service (NHS) anaesthetic activity in 2013.9 This was a questionnaire-based survey distributed to UK hospitals on two consecutive days of a chosen week, and the collected dataset was used to estimate the annual activity.9 The authors estimated annual dental caseload to be 111,600 (all ages), placing dental procedure the 8th most common among the total UK anaesthetic activities.10 A trust-wide study in Cornwall revealed that 1,442 DGA episodes took place under GA in 2014 for adults alone.8 This was 42.6% of the total adult extraction cases in this trust in 2014.8 There are 159 oral and maxillofacial surgery (OMFS) units in the UK in addition to other secondary care settings that facilitate DGA service. The activity at these institutions needs to be considered.
The study in Cornwall also revealed that a considerable number of single tooth DGA episodes were seemingly patient demand-driven,8 supporting Poswillo's views regarding the influence of patient demand in DGA prescription.3 While patients are increasingly viewed as consumers who should have access to choices,11 consideration should be given to the risks of GA and utilisation of resources provided by taxpayers. In addition, there is an important issue for the exercise of conscience by healthcare providers in selecting DGA cases. The clinician's duty to act in the best interest of patients may conflict with the principle of respect for patient autonomy, particularly when patients choose an option that clinicians feel is less appropriate.12
In this survey, we further explored the discussion points raised in the aforementioned study;8 what drives the demand for DGA in the UK and how can it be changed?
Objectives
-
To find out clinicians' perception on the current anaesthetic provision for adult dental extractions in their unit
-
To explore clinicians' views on the drivers of patient demand for DGA and on the availability of patient demand-driven GA dental service on the NHS
-
To ask clinicians' opinions on whether adult GA extraction case selection criteria would be beneficial and if so, which criteria should be included.
Methods
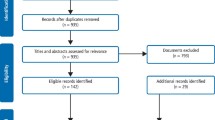
This anonymous electronic survey targeted clinicians working in OMFS units in the UK. We designed the survey, ensuring it met the requirements of the British Association of Oral and Maxillofacial Surgery (BAOMS) Research Standard Operating Procedure. The survey contained questions about GA and sedation services. We circulated an email containing the survey web-link to the UK members of the BAOMS via the association administrator. We also made an attempt to reach non-BAOMS member dental core trainees in OMFS by requesting postgraduate dental deanery administrators to distribute this email. The email recipients were encouraged to forward the email to clinicians working in an OMFS unit. Responses were collected over two months. We used Microsoft Excel to produce descriptive statistics. We categorised free text responses into themes and representative quotes are given in the results.
Results
The survey had a total minimum UK institutional response rate of 67.3%, excluding one response from Jersey (241 clinicians of varying grades from 107 out of the 159 oral and maxillofacial surgery units in the UK – nine respondents did not state their institution). The highest number of responses was from North West of England. Response rate per question varied between 90.0% and 100% because some people skipped questions. Respondents included 125 consultants (51.7%) and clinicians with varying years of experience from less than or equal to one year (n = 26, 10.7%) to longer than 20 years (n = 98, 40.5%). The characteristics of respondents are summarised in Table 1.
Clinicians' perception on the current practice in their unit
Which factor most affects your judgement when assessing whether an adult's dental anxiety is severe enough to require DGA?
The most selected option was 'failure of previous attempt to carry out dental treatment under alternative anaesthetic modality' (118), followed by 'patients declaring severe anxiety and persistently requesting GA' (53). Those who chose 'other (35)' stated the following factors; multifactorial (23), technical difficulty (5), referral information (1), incision and drainage of abscess (1), patient choice after fully informed and persuasive argument (1).
Your perceived proportion of adult DGA driven by patient demand rather than clinical need in your unit
The percentage of respondents who chose 'always' or 'most of the time' added up to 44.3%, with the addition of the responses for 'sometimes' increasing the percentage to 87.7%.
Your perceived proportion of adults listed for DGA in your unit as a result of the failure of attempts under sedation or local anaesthesia (LA)
The percentage of respondents who chose 'less than half', 'small minority', or 'none' added up to 84.5%.
Your perceived proportion of adults having DGA in your unit, who previously had dental treatment (restoration/extraction) without GA
Over half of the respondents (57.9%) perceived that 'the vast majority' (77) or 'more than half' (59) of adults having DGA in their unit previously had dental treatment without GA. The addition of 'approximately half' (33) increases the percentage to 71.9%.
Figure 1 provides a visual summary of responses to these four questions asked in this section.

(a) Factors that most affect clinicians' judgement when assessing whether an adult's dental anxiety is severe enough to require DGA; (b) Clinicians' perceived proportion of adult DGA cases driven by patient demand rather than clinical need in their unit; (c) Clinicians' perceived proportion of adults listed for DGA in their unit as a result of failure of attempts under sedation or LA; (d) Clinicians' perceived proportion of adults having DGA in their unit, who previously had dental treatment (restoration/extraction) without GA
Current provision of sedation in respondents' units
Who primarily provides sedation for adult dental extractions in your unit?
The majority of respondents (195) from 94 units stated that sedation was provided in their unit primarily by either anaesthetists (87) or dentists (101), or by both (7). However, 39 respondents from 27 units stated that sedation was not routinely offered in their unit. The responses were not always unanimous about the same unit.
Some of the respondents who reported sedation was not routinely offered in their unit provided the following comments:
'We do not offer an outpatient sedation service currently. All patients having sedation have a day-case procedure in theatre, therefore it is often as easy to offer GA', 'Sedation provision in our unit is nearly non-existent and is therefore not discussed. We would benefit from better provision', 'Very little sedation is used in my hospital, it is usually an alternative to a GA in a medically compromised patient'.
How fully are different sedation techniques discussed in your unit for adults due to undergo dental extraction?
'Only intravenous sedation' (101), 'sedation in general' (63), 'two different sedation techniques' (13), 'more than two different techniques' (1), 'full range of sedation techniques comprehensively discussed' (5).
Clinicians' opinions on adult GA dental extraction service
What do you think is the most fundamental cause that drives patient demand for GA extractions in the UK?
'Dental anxiety' (65), 'availability on the NHS' (50), 'referral from primary care for GA extraction' (45), 'low confidence/competence in minor oral surgery among primary care clinicians' (34), 'lack of specific guidelines' (16), and 'other' (22) including 'multifactorial' (7). The rest of the free text responses in the 'other' group are categorised as below.
Primary care
'Relative ignorance at primary care level of the true justification for GA', 'General dental practitioners raising patient expectations for GA for commercial imperative to get patient out of room as soon as possible, but also because of inability to extract teeth', 'Lack of trained oral surgeons in the high street, poor remuneration for more difficult extractions...'
Provision of sedation services
'Lack of availability of sedation', 'No clearly defined sedation service pathway'.
Patient factors
'Mass hysteria in the population regarding dental treatment', 'Misconception of pain experienced during extractions', 'Folklore about the ready availability of extractions under GA as a routine and acceptable treatment'.
Do you feel that adult GA dental extraction service should be available on the NHS for patients requesting it without clinical need?
Yes (n = 44, 19.1%)
Current barriers to alternative anaesthetic modalities
'The present system does not allow enough time for clinicians to extensively counsel a phobic patient', 'Perception of severe anxiety is a barrier to LA treatment', 'There should be more widely available sedation service'.
Subjectivity in assessing and defining clinical need
'There should be some scope for manoeuvrability in the system unless we are able to establish evidence-based guidelines for appropriately assessing clinical needs'. 'What is 'clinical need?', 'How incredibly arrogant it is to assume we can absolutely define clinical need', 'Is anxiety clinical need?', 'Anxiety is clinical need'.
Consent and autonomy
'It's an issue for consent', 'We as a speciality control most of the access to GA in exodontia and hence we must be guardians of this service, and patients need to be guided by clinicians as to when GA is appropriate', 'Patient choice is one of the principles of modern practice'.
Emergency cases
'Removing GA service for those without clinical need would result in increased prevalence in emergency dental infection cases'.
No (n = 186, 80.9%)
While recognising that this service should be available for those who need it (eg severe anxiety, psychiatric problems), the majority of the respondents answered 'No' to providing this service on the NHS for those without 'clinical need'. The two most frequently mentioned reasons were 'a waste of resources' (39) and 'the risks of GA' (22). The rest of the free text responses from this group could be categorised into the following themes.
Culture
'The NHS is not an à la carte menu', 'GA is a cultural issue in the UK', '...Occasionally at the end of a long clinic, I can lose the will to argue – life is too short so I can be brow beaten and agree against my better judgement. Overall, it's a culture of expectation', 'Depends on the unit's attitudes towards GA. Big drive towards LA and patients rarely complain in one unit. While at another unit, every pt got a GA at request unless medical problem pertaining to receive LA only'.
System-related
'In a well-constructed service, the number of people for whom a GA is the optimum treatment option is small'. 'No barrier access promotes the philosophy of turning to GA for increasingly minor care', 'Coming from a country where added cost is incurred by the patient, they often overcome that dental fear', 'If GA had to be self-funded we would not see the level of GAs that we currently do in the UK', '18-week referral-to-treatment times constantly under pressure with 'managed' backlog of patients having already breached', 'GA should not be considered as a restrictive item under OMFS as it will only lead to individual funding requests being required for those patients'.
Sedation
'GA should be clinician-driven if sedation fails', 'For procedures that are amenable to LA/sedation, this should be the mode of anaesthesia offered and defended where possible'.
Patient attitude towards GA
'Not helpful for patients long-term for overcoming dental anxiety', 'Patients bully their way into GA but don't accept ownership of the risks of resource demands', 'Patients increasingly demanding and I have experience of formal complaints lodged if told inappropriate', 'Patients as a rule do not interest themselves in the consequences, merely gratification by getting what they want or feel they need', 'Often big argument with patients demanding GA. Having waited 10 weeks for consult do not want to go back to own dentist', 'Often patients have significant medical history but still demand GA against advice. There is a real need for a separate consent form for the anaesthetic', 'Often not worth the effort of trying to convince someone with pre-convinced notions.'
Subjectivity in assessing and defining clinical need
'The responsibility for the patient lies with the clinician making the decision to provide GA and therefore it should only be provided for those cases where the surgeon feels it is warranted', 'Clinical need should be the only reason and if patients refuse then they should go private'.
'...We do lots of things people don't need (eg minor orthognathic surgery)', 'What a stupid question. If there was no clinical need who would offer them treatment? And what has the NHS got to do with it? If treatment denied by the NHS then how is it ethical to do it privately?'
Do you feel that guidelines with adult GA dental extraction case selection criteria would help reduce the number of demand-driven GA extractions?
No (n=91, 41.9%)
Patients' attitude
'Patient will not listen to clinicians' opinion and will not respect the criteria', 'Some of our patients are quoted 30% chance of stroke and 10% mortality and still want GA, 'I'll sign anything, doc', no chance these patients will get GA but it shows mindset'. 'In my experience, if a patient wants a GA they will always end up receiving by making a formal complaint to the hospital or the primary care trust. Most of these organisations will always give in to patient demands to avoid negative media attention rather than stand up for what is clinically right', 'A number of my colleagues have had patient complaints against them simply for declining general anaesthetic treatment for simple single tooth extractions. The patients have consequently made a complaint resulting in reversal of the clinician's decision.'
Alternative ideas to guidelines
'This problem is deeper seated and relates to education of general dental practitioners', 'Unless formal advice from speciality of what should be available on NHS, complaints will still drive GA availability', 'If not required, patients should be offered private supplement if demanding GA without clinical need', 'All the anxiety indices can easily be skewed ... Extending the waiting times for GAs would be more effective...', 'Train better dentists and remuneration for treatment needs revision...'
Pessimism rooted in other existing guidelines
'There are guidelines for many things, for example impacted wisdom tooth extraction guidelines, which aren't adhered to', 'They'll soon get round it like how fast track has been inappropriately used'.
Emergency cases
'You can stop elective cases but non-elective patients will present to emergency department or GP. How many will end up as acute oro-facial infections?'
Yes (n = 126, 58.1%)
The selection criteria suggested by the respondents (Table 2) could be categorised into four themes; anxiety-based, surgical factors, medical history-related, and referral triage.
Representative quotes from this group are as follows:
'This must be dictated by commissioners and patients told it is a service that is limited by these rules', 'We still get many patients demanding GA – this has led to many patient complaints which is time consuming. I get feeling rightly or wrongly that it is sometimes easier to list for GA', 'There should be concrete sedation services available within outpatient departments. Currently sedation is done in theatre with anaesthetists using polypharmacy intravenous agents. Dentists should be able to do conscious sedation within OMFS outpatients...', '...paradoxically inner city areas are not always the most deprived; need to sample what it is like outside teaching hospitals!'
Discussion
The growing number of paediatric extractions under GA in the UK is a long-standing problem,13 and receives media attention from time to time which highlights the seriousness of the issue to the public. Interestingly, despite the risks and the cost implications of over-prescription of GA being no more acceptable in adults than in children, the provision of DGA for adults receives far less attention. Currently, there are far fewer numbers of publications about adult DGA services in the literature, compared to those about paediatric DGA services.
This article reports the perceptions, assumptions, and speculations of 241 clinicians working in the majority of OMFS units in the UK on the anaesthetic provision for routine adult dental extraction procedures. Our results revealed a general consensus that clinicians in OMFS units perceived a strong patient demand for DGA. Many respondents expressed that their decision to prescribe GA was influenced by non-clinical reasons including patient complaints, insufficient time to counsel patients, and losing the will to argue with patients.
Many respondents chose 'failure of previous attempt under alternative anaesthetic modality' as the factor that most affected their judgement when assessing the severity of dental anxiety to prescribe DGA. However, somewhat paradoxically, their perceived reality was that a relatively small proportion of adults were listed for DGA as a result of the failure of attempts under sedation or LA. Also, 71.9% of the respondents perceived that a high proportion of adults having DGA in their unit previously had dental treatment (restoration/extraction) without GA. One possible explanation for this could be that patient demand potentially has a bigger impact on the actual decision than clinical judgement.
In 1994, before removal of the DGA service from the general dental practice, Hastings et al.6 found that although dentists offered patients options, the reality of the process was that the opinion/preference of the dentist was accepted. This led to the question whether dentists' opinion played a part in generating public demand and acceptance of GA.6 Twenty-two years later, in our survey, clinicians in OMFS units identified the drivers of demand for DGA to be factors related to patients, primary care practitioners, and the lack of robust sedation service provision.
Dental anxiety received the highest response (28.0%) as the most fundamental driver for patient demand for DGA. This leads to the question, what is the most effective management of dental anxiety? Conscious sedation is a safer technique that allows higher turnover of patients at a considerably lower cost than GA.14 It is concerning that 27 of the participating OMFS units did not routinely provide sedation. In addition, our survey revealed that, in many OMFS units where sedation service was available, this was primarily provided by anaesthetists. There are implications of these findings for practice and future research; does the availability of anaesthetists and multiple theatre facilities equipped for GA increase the likelihood of patients having DGA? Kim et al.15 conducted a study in West Midlands and found that two hospitals with GA facilities relied heavily on the use of day-case GA for third molar removals. Another unit without GA facilities predominantly used LA with intravenous sedation successfully. Moreover, Sammut et al.16 compared the practice of two institutions in Edinburgh; a dedicated oral surgery department without onsite theatre facilities for GA and an OMFS unit. Both units offered LA and sedation, but patients seen at the OMFS unit were almost twice as likely to be listed for GA for mandibular third molar surgery. The authors stated this difference was not related to the difficulty of the cases, but rather attributable to the nature of a maxillofacial unit and possibly the socioeconomic differences. Such evidence on a wider scale would strengthen the case for appropriate funding to improve the provision of sedation service in both primary and secondary care. Another question derived from our results was whether the anaesthetists are providing an appropriate level of 'conscious' sedation in these units. As mentioned previously, one of our respondents stated '...Currently sedation is done in theatre with anaesthetists using polypharmacy intravenous agents... Dentists should be able to do conscious sedation within OMFS outpatients...'.
Dental anxiety was followed by 'the availability on the NHS' (21.6%) as the most fundamental driver for patient demand for DGA. Furthermore, the majority (80.9%) did not support the availability of this service on the NHS for those without 'clinical need'. One of the repeatedly mentioned opinions throughout the survey was that patient demand-driven DGA should be offered privately – but, there was also an opposing opinion from a respondent: 'if treatment denied by the NHS then how is it ethical to do it privately?' Another question to ask would be 'how is it ethical to keep this service on the NHS if the fact that DGA is free at the point of service influences patients' decision?' A Canadian study17 found that some people (12.3%) in the no or low dental fear group were definitely interested in sedation or GA for their dentistry, but there was a larger proportion of people (42.3%) who were interested in sedation or GA depending on cost. Similarly, with high fear, 31.1% were definitely interested, with 54.1% interested depending on cost.17
Guidelines
The word 'clinical need' in the survey questions generated many responses in the free text boxes with a lot of respondents questioning or giving their own version of its definition. It is perhaps reasonable to imagine some people would question what the General Dental Council18 meant by 'GA should only be considered if there is overriding clinical need'. In 2000, the Department of Health5 stated that all other alternative ways to manage anxiety should be excluded before recourse to GA. The terms used in this guidance were arguably broad and simplistic, and more stringent referral criteria guidelines19,20 have been produced to clarify justifications for paediatric DGA. While it would not be possible to establish an absolute, exhaustive list of indications for DGA, is it incumbent for more stringent guidelines to be produced for adults, too?
Although there was a general consensus that the demand-driven DGA culture needs to be addressed, some were pro- and others were anti-guidelines. A small majority (58.1%) of the respondents felt guidelines with adult DGA case selection criteria would help reduce the number of demand-driven GA extractions with many providing criteria that they would like to see in the guidelines (Table 2). Some of the suggested criteria, such as psychiatric conditions and incapacity, appear in the paediatric DGA guidelines,19,20 but others were more applicable for and prevalent in adults – indications such as technical difficulties of mandibular third molar removals, high risk of mandibular fracture, and urgency due to impending medical treatment needs. On the other hand, the 42% who did not feel that such guidelines would improve the situation were pessimistic of the potential for change in patients' attitude towards DGA, and some cited the poor adherence to other existing guidelines. Some respondents suggested alternative ideas to guidelines such as privatisation, revision of remuneration, and improving education and training.
A few people speculated that emergency cases may rise if patients are refused GA because patients may adopt avoidance for dental extraction under other anaesthetic modalities. One of the important aspects to consider regarding the emergency DGA cases would be the number of these cases we are already encountering as a result of the long DGA waiting list. It was found that the average waiting time for DGA was 136 days in one hospital trust in 2014.8 North et al.21 reported on the effects of a six month waiting list for children's DGA; 41.0% of their cohort required analgesics, 49.4% received antibiotics, and 32.9% had problems eating. Similarly, a study conducted in the Netherlands found that, during the eight weeks of waiting period for DGA, 43% of the cohort developed complications, and with every week of waiting, the likelihood of children developing complications increased by 6.7%.22
One of the strengths of this survey was its uniqueness in that it captured one of the important dimensions that should be considered when planning the future: how clinicians feel about the current situation and how they think we should move forward with regards the provision of routine adult DGA. The responses were from the majority of OMFS units in the UK, and revealed that over-prescription of DGA is a widespread issue in the UK. The results also highlighted the lack of sedation provision in some OMFS units and the need to improve this. However, the survey had limitations; we asked our respondents their perceptions on the current practice in their unit, rather than factual information. Also, it should be noted that, although the survey yielded an institutional response rate of 67.3%, the number of our respondents (241 clinicians) constitute a relatively small proportion of the whole targeted population.
Going back to the beginning, there was a time when having a tooth out without anaesthesia was the cultural norm. Since 1846 when anaesthesia was first performed in England,1 the cultural norm has gradually shifted to the other extreme of automatically associating dental extraction with GA in spite of the advent of effective LA and sedation techniques. Today, the demand for DGA is perceived to be so strong that clinicians' decisions are influenced, or reversed even, by patient driven factors such as complaints, for example. This topic requires attention for future research. The authors are currently further investigating the scope of the problem in quantitative terms.
Conclusion
This survey demonstrated the presence of a strong culture of patient demand-driven adult DGA in the UK as perceived by many of our respondents. There was a general consensus that this culture needs to be addressed, but opinions were varied on how this could be achieved. What would it take to shift the cultural norm again?
References
Enever G . The history of dental anaesthesia. In Shaw I, Kumar C, Dodds C. Oxford textbook of anaesthesia for oral and maxillofacial surgery. 1st ed. Oxford: Oxford University Press. 2010.
Howe L G, Whitehead F I M . The development of local anaesthesia in dentistry. In Howe L G, Whitehead F I M. Local anaesthesia in dentistry. 2nd ed. pp 11–15. Bristol: John Wright and Sons, 1946.
General anaesthesia, sedation and resuscitation in dentistry: report of an expert working party. London: Department of Health, 1990.
Landes D P . The provision of general anaesthesia in dental practice, an end which had to come? Br Dent J 2002; 192: 129–131.
A conscious decision, a review of the use of general anaesthesia and conscious sedation in primary dental care. London: Department of Health, 2000.
Hastings G B, Lawther S, Eadie D R, Haywood A, Lowry R, Evans D . General anaesthesia: who decides, and why? Br Dent J 1994; 177: 332–334.
Robertson S, Chaollai A N, Dyer T A . What do we really know about UK paediatric dental general anaesthesia services? Br Dent J 2012; 212: 165–167.
Hong B, Birnie A . A retrospective analysis of episodes of single tooth extraction under general anaesthesia. Br Dent J 2016; 220: 21–24.
Sury M R J, Palmer J H M G, Cook T M, Pandit J J . The State of UK Dental Anaesthesia: Results From The NAP5 Activity Survey. A national survey by the 5th National Audit Project of the Royal College of Anaesthetists and the Association of Anaesthetists of Great Britain and Ireland. SAAD Dig 2016; 32: 34–36.
Sury M R J, Palmer J H M G, Cook T M, Pandit J J . The state of UK anaesthesia: a survey of National Health Service activity in 2013. Br J Anaesth 2014; 113: 575–584.
Khalique N . Informed consent: the dawning of a new era. Br J Oral Maxillofac Surg 2015; 53: 479–484.
Beauchamp T L, Childress J F . Principles of biomedical ethics. 5th ed. New York: Oxford University Press, 2001.
Royal College of Surgeons of England. Faculty of Dental Surgery. The state of children's oral health in England. January 2015. Available at: http://www.rcseng.ac.uk/fds/policy/documents/fdsreportonthestateofchildrensoralhealth (accessed October 2016).
Jameson K, Averley P A, Shackley P, Steele J . A comparison of the 'cost per child treated' at a primary care-based sedation referral service, compared to a general anaesthetic in hospital. Br Dent J 2007; 203: E13.
Kim D S, Lopes J, Higgins A, Lopes V . Influence of NICE guidelines on removal of third molars in a region of the UK. Br J Oral Maxillofac Surg 2006; 44: 504–506.
Sammut S, Lopes V, Morrison A, Malden N J . Predicting the choice of anaesthesia for third molar surgery guideline or the easy-line? Br Dent J 2013; 214: E8.
Chanpong B, Haas D A, Locker D . Need and demand for sedation or general anaesthesia in dentistry: a national survey of the Canadian population. Anaesth Prog 2005; 52: 3–11.
General Dental Council. Maintaining standards guidance to dentists on professional and personal conduct. London: GDC, 1997.
Davies C, Harrison M, Roberts G . UK national clinical guidelines in paediatric dentistry: guideline for the use of general anaesthesia in paediatric dentistry. London: Royal College of Surgeons of England, 2008.
Adewale L, Morton N, Blayney M . Guidelines for management of children referred for dental extractions under general anaesthesia. London: Association of Paediatric Anaesthetists of Great Britain and Ireland. 2011. Online article available at http://www.apagbi.org.uk/sites/default/files/images/Main%20Dental%20Guidelines%5B1%5D_0.pdf (accessed July 2016).
North S, Davidson L E, Blinkhorn A S, Mackie I C . The effects of a long wait for children's dental general anaesthesia. Int J Paediatr Dent 2007; 17: 105–109.
Boehmer J, Stoffels J A W, Rooij IALM van, Heyboer A . Complicaties door wachttijd voor behandeling onder algehele anesthesie. Ned Tijdschr Tandheelkd 2007; 114: 69–75.
Acknowledgements
We are grateful to BAOMS and postgraduate dental deaneries for helping in the circulation of this survey.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Hong, B., Baker, A. General anaesthetic service for adult dental extractions: an 'À La Carte Menu'? Survey results. Br Dent J 222, 261–267 (2017). https://doi.org/10.1038/sj.bdj.2017.171
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2017.171
This article is cited by
-
The resurgence of sedation
British Dental Journal (2020)
-
Frequency, variation and cost of dental extractions for adults in secondary care in Great Britain
British Dental Journal (2019)
-
Is general anaesthesia still the easiest option?
British Dental Journal (2017)
-
OMFS: GA rights
British Dental Journal (2017)
